
Abstract
Introduction
Antiphospholipid syndrome (APS) is a systemic autoimmune disease characterized by the combination of arterial or venous thrombosis, fetal losses in the presence of antiphospholipid antibodies (aPL), namely lupus anticoagulant (LA), anticardiolipin antibodies (aCL) or antibodies directed to beta 2-glycoprotein I (β2GPI), or in the presence of all three. 1 First recognized in patients with systemic lupus erythematosus (SLE), it is now well known that the development of this syndrome may also be independent of any underlying disease, being termed ‘primary’ APS. 2 Over the years, the list of clinical signs and symptoms related to aPL has been extended and currently, it is known that the whole renal vasculature can be affected in aPL-associated nephropathy (aPLN). 3 Specifically, glomerular involvement by aPL has been associated with chronic renal ischaemia, 4 – 7 and from the clinical point of view hypertension, acute renal failure and chronic low-grade proteinuria are the most prominent manifestations. 3 Thrombotic microangiopathy (TMA), the best-known lesion related to aPL, represents an acute event. 5 In contrast, fibrous intimal hyperplasia (FIH), fibrocellular arterial occlusion (FAO), focal cortical atrophy (FCA) and tubular thyroidization reflect chronic renal damage. 5
Overall, the prevalence of aPLN in patients with SLE varies from 10.4–34%. 6 – 9 The aPLN is undoubtedly frequent but not specific in patients with APS. In fact, the committee of the last International Consensus on Diagnostic Criteria for APS considered that adoption of aPLN as criterion for definite APS may decrease diagnostic specificity, and it recommends the use of the term ‘aPL-associated nephropathy’ when aPL and the previous histological findings coexist. 1
In the study of Daugas et al., 6 APS nephropathy was related to hypertension and elevated serum creatinine at the time of renal biopsy as well as increased interstitial fibrosis, probably associated with worse renal functional prognosis. In the largest series of aPLN, 7 arterial thromboses, pulmonary embolism, livedo reticularis, aCL, and LA were strongly associated with aPLN. In addition, patients with aPLN develop hypertension, raised serum creatinine levels, and progression of histological lesions in serial kidney biopsy specimens. 7
The purpose of the current study was to evaluate the prevalence of APS nephropathy among patients with lupus nephritis and to describe the clinical, immunological features and renal outcome of these patients.
Subjects and methods
Analysis was performed for 79 renal biopsies from 77 consecutive patients followed at the Departments of Autoimmune Diseases and Nephrology of Hospital Clinic, Barcelona, Catalonia, Spain. Two patients had a second renal biopsy due to recurrent lupus nephritis. All of the patients fulfilled at least four of the ACR criteria for the diagnosis of SLE 10 at the time of kidney biopsy. Renal biopsies were performed between 1991 and 2008 and the World Health Organization (WHO) classification of lupus glomerulonephritis 11 and the WHO activity and chronicity index scores 12 were retrospectively re-evaluated. Patients with suspected vascular lesions associated with other diseases such as systemic sclerosis, thrombotic thrombocytopenic purpura, haemolytic–uremic syndrome, systemic vasculitis, diabetic nephropathy, preeclampsia, and infection by human immunodeficiency virus were excluded. No patient developed malignant hypertension before renal biopsy.
The study was approved by the local ethics committee and performed according to the principles of the Declaration of Helsinki. Informed consent was obtained for all participants.
The following clinical and serological data from each patient obtained at the time of the kidney biopsy were collected from the medical records: age, sex, duration of SLE (time from the diagnosis of SLE to kidney biopsy), time from the kidney biopsy to the end of follow-up, APS according to the Sydney criteria, 1 systemic hypertension (systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg), nephrotic syndrome (urinary protein level >3.5 g/24 h), proteinuria (presence of ≥ 0.5 g/dl of protein in 24 h at least in two determinations), haematuria (presence of ≥ 5 red cells per field (100×) in isolated urine sample at least in two determinations), serum creatinine levels, glomerular filtration rate, serum albumin levels, anti-dsDNA antibody, C3, C4 and CH50, LA, IgG aCL and IgM aCL antibodies. Treatment with anticoagulation, antiplatelet and antimalarial drugs was also recorded.
For each patient, the duration of follow-up was considered as the time from kidney biopsy to the last medical visit. The following data were recorded during this period: systemic hypertension, proteinuria, haematuria, serum creatinine levels, glomerular filtration rate, serum albumin levels, anti-dsDNA antibody, C3, C4 and CH50, LA, IgG aCL and IgM aCL antibodies. In addition, the development of APS, renal failure (creatinine clearance <75 ml/min), end-stage renal disease (ESRD) requiring dialysis or renal transplantation, and death were also recorded. Finally, treatment with anticoagulation, antiplatelet and antimalarial drugs was also recorded. According to the European Consensus on the terminology used in the management of lupus glomerulonephritis, 13 the absence of haematuria, a proteinuria level ≤ 0.2 g/day and normal or stable renal function (normal glomerular filtration rate or variations not greater than 10% of the previous value if the filtrate was previously altered) was considered as complete renal remission. A partial renal remission was considered if the proteinuria level was ≤ 0.5 g/day with normal or stable renal function. According to the SLICC Damage Index, 14 the presence of glomerular filtration rate ≤ 50 ml/min and/or proteinuria ≥ 3.5 g/day maintained for 6 months and/or ESRD with or without replacement therapy was considered established renal damage.
Renal biopsies
Retrospective evaluation was performed using the original slides from renal biopsies processed for routine conventional light microscopy. Specimens were fixed in Bouin or buffered formalin and embedded in paraffin. Sections were stained with hematoxylin–eosin, periodic acid-Schiff (PAS), Jones’ methenamine silver and Masson’s trichrome. Immunofluorescence (IF) results were retrieved from the original reports.
Each biopsy was retrospectively evaluated by a pathologist who was blinded to the aPL status. The following data from each biopsy sample were collected: (1) type of glomerulonephritis according to WHO classification with activity and chronicity indices; (2) lesions suggestive of acute aPLN such as TMA, consisting of the presence of fibrin thrombi in arteries, arterioles and/or glomeruli; (3) lesions suggestive of chronic aPLN such as FIH, consisting of myofibroblastic cellular proliferation in the intima with luminal narrowing of small arteries, FAO consisting of arterial fibrous occlusion and FCA with or without tubular thyroidization; and (4) lesions consistent with arteriosclerosis characterized by fibrous intimal thickening with multilayering of the internal elastica, without specific findings of aPLN. As one of the objectives was to evaluate the interstitial and vascular lesions, we included all biopsies independently of the number of glomeruli.
Laboratory determinations
Anti-dsDNA antibodies, C3, C4, and CH50 were assessed according to standard methods. LA was detected using activated partial thromboplastin time, diluted Russell’s viper venom time, and tissue thromboplastin inhibition test. Tests were also performed in mixtures with control plasmas or phospholipids following the guidelines of the Subcommittee for the Standardisation of Lupus Anticoagulants of the International Society of Thrombosis and Hemostasis. 15 The aCL were determined by enzyme-linked immunosorbent assay (ELISA) (Cheshire Diagnostics, Cheshire, UK). Results were expressed in IgG and IgM phospholipid units and reported as negative (≤ 15 units), low positive (16–25 units), moderate positive (26–40 units), and high positive (>40 units).
Statistical analysis
For statistical studies, we considered the total number of renal biopsies. For comparison purposes, the whole series has been divided in three groups according to the aPL status at the time of renal biopsy and the existence of aPLN. Group 1 was defined as SLE patients without aPL and without aPLN; Group 2 was defined as SLE patients with aPL but without aPLN; and Group 3 was defined as SLE patients with aPL and aPLN. Taking into account that our cohort of patients had SLE, at least one positive determination of aPL at any time before renal biopsy was sufficient to consider a patient as having aPL. However, to analyse the presence of aPLN according to the profile of aPL, we excluded those patients with positive aPL based on only one determination of aCL IgG or aCL IgM at low titres at the time of renal biopsy.
Categorical variables were compared using chi-squared test and Fisher exact test. Continuous variables were analysed by Student’s test in similar large-sample variance test and by Mann–Whitney test for small samples, with results expressed as mean ± standard deviation (SD). The p-value <0.05 was taken as statistically significant difference. Statistical analysis was performed using SPSS 12.0 (SPSS, Chicago, IL).
Results
In total, 79 renal biopsies from 77 consecutive patients with SLE were included. Seventy (88.6%) patients were female. The mean age of SLE patients at time of biopsy was 33.3 ± 11.6 years old (range 14–66). The time from SLE diagnosis to renal biopsy was 71.2 ± 77.3 months. The follow-up period was 73.0 ± 51.0 months (range 1–215).
General characteristics of patients with lupus nephropathy according with aPL status and coexistence of aPLN
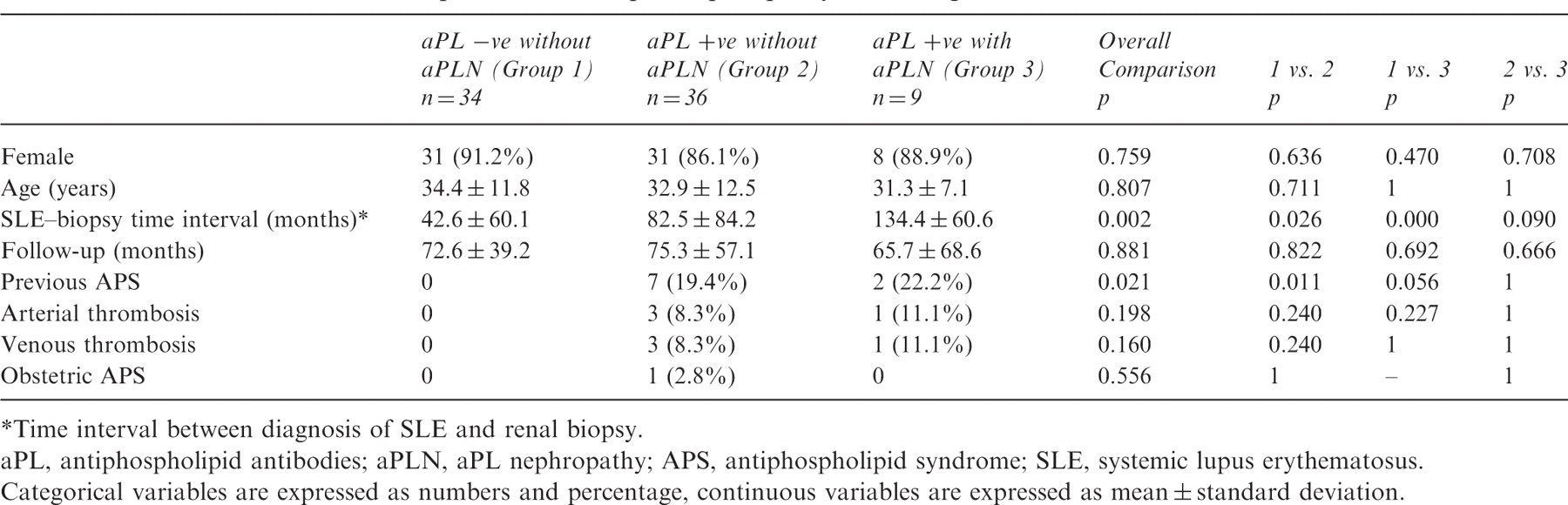
Time interval between diagnosis of SLE and renal biopsy.
aPL, antiphospholipid antibodies; aPLN, aPL nephropathy; APS, antiphospholipid syndrome; SLE, systemic lupus erythematosus.
Categorical variables are expressed as numbers and percentage, continuous variables are expressed as mean ± standard deviation.
Histological features
Histological findings in the analysed subgroups
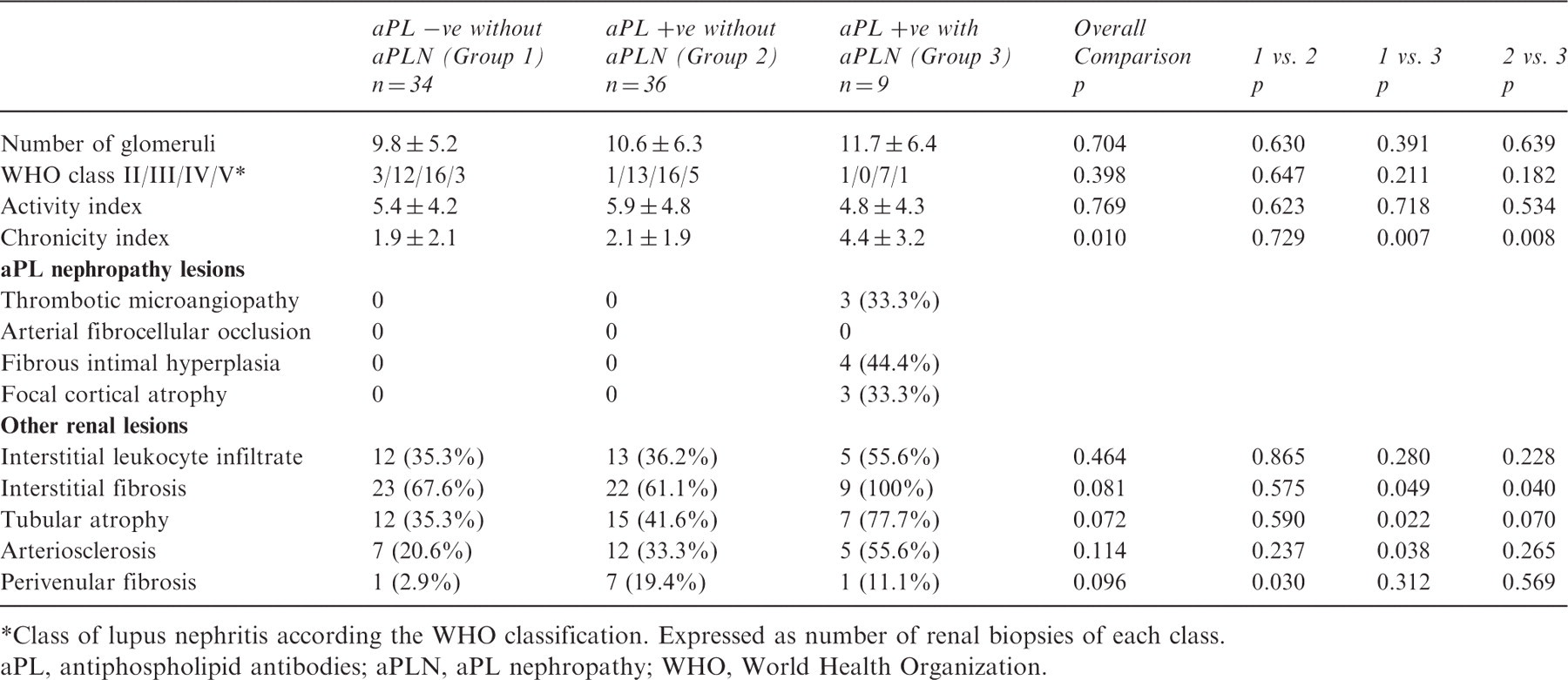
Class of lupus nephritis according the WHO classification. Expressed as number of renal biopsies of each class.
aPL, antiphospholipid antibodies; aPLN, aPL nephropathy; WHO, World Health Organization.
Activity index was similar between the three groups of cases. In contrast, patients with aPLN had the highest chronicity index (p = 0.010) in comparison with the rest of the analysed groups. Regarding other renal lesions, all patients with aPLN had interstitial fibrosis. Moreover, a higher prevalence of interstitial fibrosis (p = 0.049), tubular atrophy (p = 0.022) and arteriosclerosis (p = 0.038) was found in cases with aPLN (Group 3) compared with those without aPL (Group 1). In addition, patients with aPLN (Group 3) had higher prevalence of interstitial fibrosis (100% vs. 61.1%; p = 0.04), tubular atrophy (77.8% vs. 41.7%; p = 0.07) and nephroangiosclerosis (55.6% vs. 33.3%; p = 0.265) in comparison with patients with aPL but without aPLN (Group 2).
Clinical characteristics and laboratory features of patients with aPLN
Clinical and laboratory features of the whole series at the time of renal biopsy and at the end of follow-up
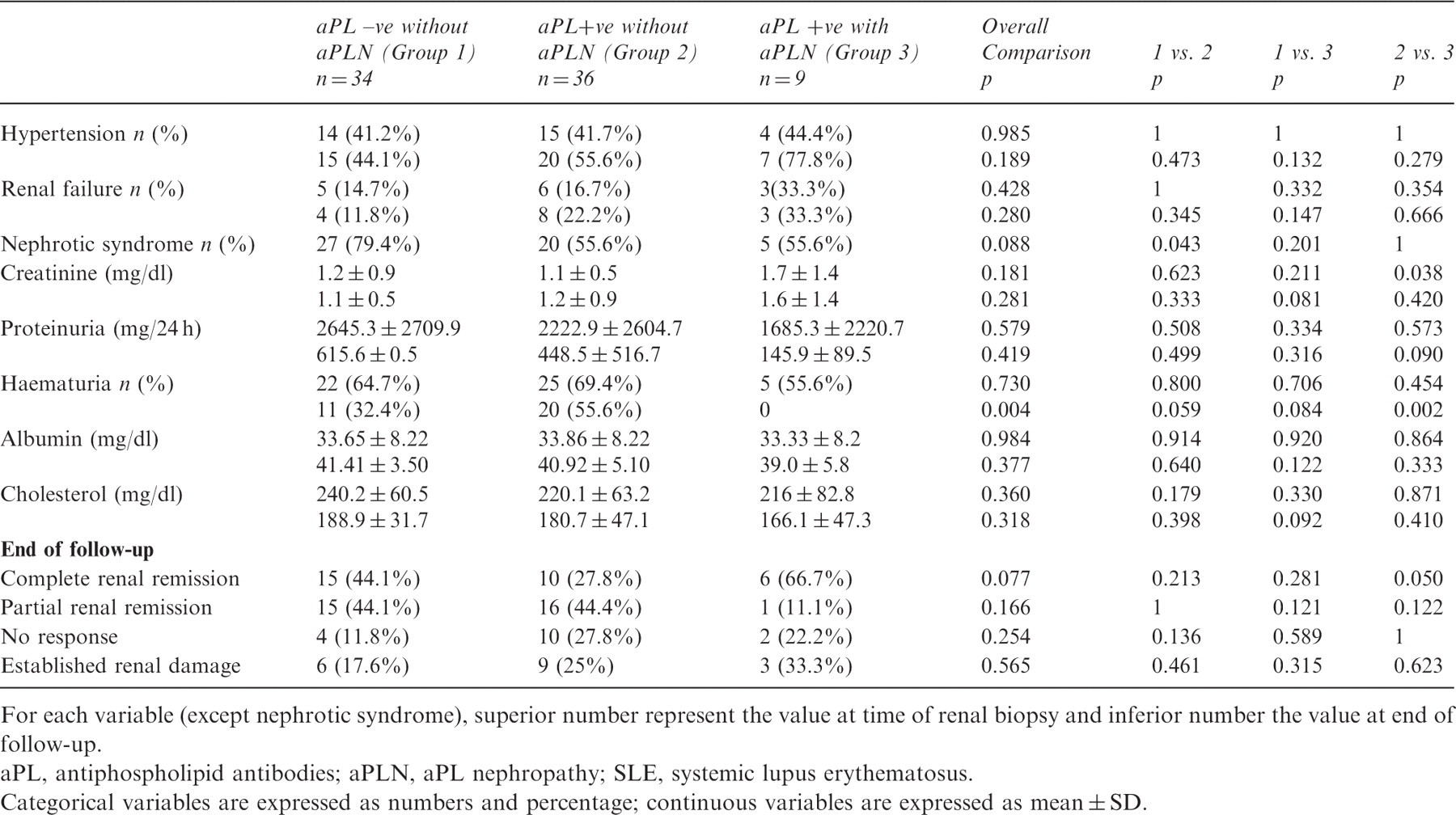
For each variable (except nephrotic syndrome), superior number represent the value at time of renal biopsy and inferior number the value at end of follow-up.
aPL, antiphospholipid antibodies; aPLN, aPL nephropathy; SLE, systemic lupus erythematosus.
Categorical variables are expressed as numbers and percentage; continuous variables are expressed as mean ± SD.
Overall, no difference between patients with and those without aPLN regarding treatment with cyclophosphamide (p = 0.873), azathioprine (p = 0.662), mycophenolate mofetil (p = 0.434), hydroxychloroquine (p = 0.221), or corticosteroids (p = 0.506) was found.
No significant difference in complete renal remission, partial remission and no response between groups were observed. The presence of established renal damage seemed to be more frequent in the group with aPLN compared with the others, although this difference did not achieve statistical significance (33.3% vs. 21.4%; p = 0.42). Regarding the renal functional outcome, no significant differences in proteinuria and haematuria were found at the end of follow-up between the three groups. Serum creatinine levels tended to be higher in patients with aPLN although this difference did not achieve statistical significance (1.6 ± 1.4 vs. 1.1 ± 0.8; p = 0.18). Immunological characteristics represented by complement levels and anti-dsDNA antibody titres were similar in three groups at the time of renal biopsy and at the end of follow-up.
At the end of follow-up, two (2.6%) patients who did not have aPLN required renal transplantation, and only one (1.3%) patient without aPLN died because of catastrophic APS.
Relationship between aPLN and aPL profile
Forty-five (56.9%) patients had at least one positive determination for aPL at any time before renal biopsy. There was no difference in the time period between aPL determinations and renal biopsy in the three groups of patients and between patients with acute aPLN and those with chronic aPLN. However, six patients with only one positive determination of aCL IgG or aCL IgM at low titres at the time of renal biopsy were excluded. The aPL profile in the nine patients with aPLN was the following: two had triple positivity for LA plus aCL IgG and IgM; four had double positivity for LA and aCL IgG; one patient had double positivity for LA and aCL IgM; one had double positivity for aCL IgG and IgM; and the remaining had aCL IgM. Of note, 4/7 patients with aCL IgG had high titres and three had moderate titres. Regarding aCL IgM, 4/5 patients had high titres and the remaining had moderate titres. Conversely, the six patients with only low titres of aCL as a positive determination before renal biopsy did not show any histological feature of aPLN.
Profile of aPL at the time of renal biopsy according the presence of aPLN*
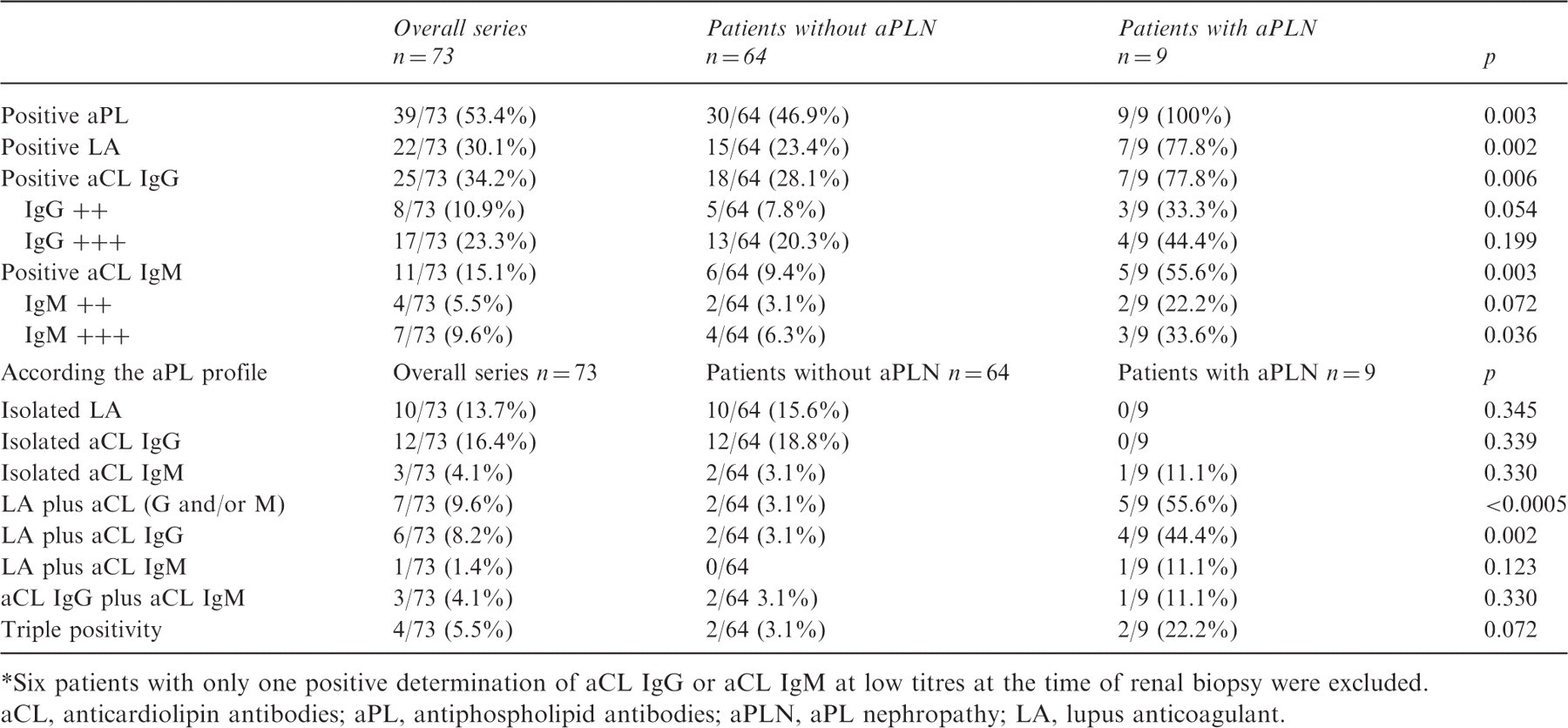
Six patients with only one positive determination of aCL IgG or aCL IgM at low titres at the time of renal biopsy were excluded.
aCL, anticardiolipin antibodies; aPL, antiphospholipid antibodies; aPLN, aPL nephropathy; LA, lupus anticoagulant.
Regarding the specific aPL profile, the association of LA plus aCL was related to the presence of aPLN (OR: 3.65, 95% confidence interval (CI) 1.73–5.58; p < 0.0005). In fact, patients with LA plus aCL IgG showed an increased prevalence of aPLN (OR: 3.61, 95% CI 1.28–5.14; p = 0.002).
Overall, 10 out of 14 (66.7%) patients with positive aPL based on one determination at the time of renal biopsy were persistently positive for aPL during their follow-up. Of note, two of the remaining four patients had a follow-up period below 18 months. An additional patient was missing after renal biopsy.
Relationship between aPLN and APS
Patients with aPLN did not have an increased prevalence of APS at the time of renal biopsy (Table 1). Moreover, no differences in venous thrombosis, arterial thrombosis or obstetric morbidity were found when cases with aPLN were compared with those with aPL but without aPLN. Clinical events related to APS were arterial thrombosis in four patients, venous thrombosis in four, and obstetric morbidity in one patient. Two patients with previous arterial thrombosis were receiving antiaggregant platelet therapy at the time of biopsy, one patient was treated with antimalarials, and the remainder who were not receiving anticoagulation or antiplatelet therapy had APS nephropathy. The four patients with previous venous thrombosis were receiving oral anticoagulation at the time of lupus nephritis. Patients with obstetric morbidity were under antiplatelet therapy. Owing to the low number of cases with aPLN, the potential protective role of anticoagulation could not be analysed.
As a consequence of retrospective character of the analysis, the presence of aPLN did not assume change in the treatment of patients included in the study. At the end of follow-up, five (6.5%) patients presented new thrombotic events (two venous thromboses and three arterial thromboses). Only one patient with arterial thrombosis had aPLN. This patient was the same one who suffered previous arterial thrombosis with aPLN without anticoagulation. No significant association between the presence of aPLN and subsequent development of thrombotic events (p = 0.46) was found.
Twelve patients without aPL at the time of renal biopsy showed positive aPL at the end of follow-up. None of them presented aPLN, and no thrombotic events, obstetric morbidity or renal involvement were observed during follow up in this group.
Discussion
We found a significant association between the presence of aPL and aPLN. Moreover, patients with LA plus IgG aCL showed an increased prevalence of APS nephropathy, suggesting that these aPL play a direct role in the development of aPLN. Interestingly, the presence of at least one positive determination of aPL at the time of renal biopsy was enough to establish this association.
Clinical, laboratory, and histological features of patients with aPLN at the time of renal biopsy according to different reported series
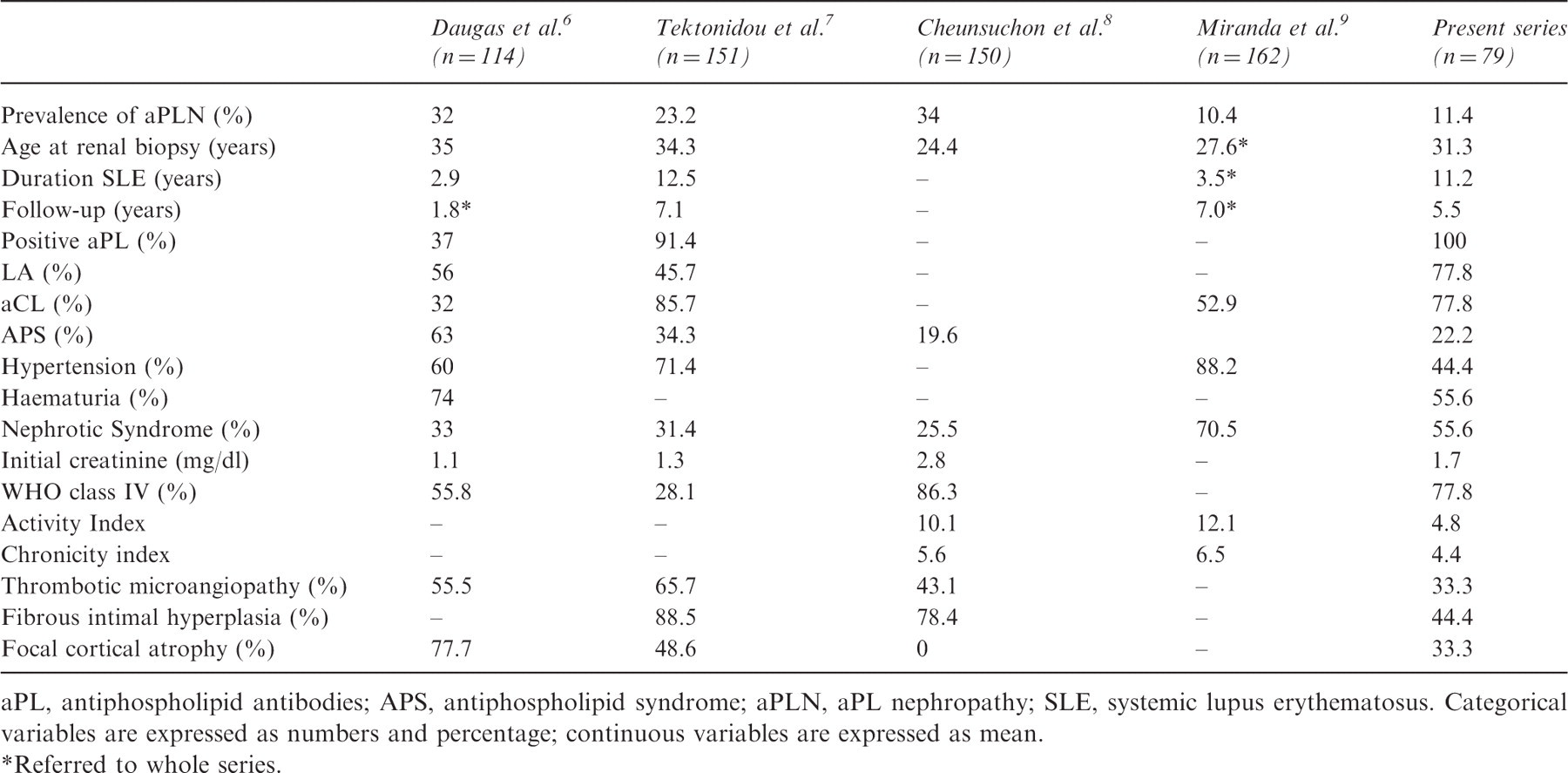
aPL, antiphospholipid antibodies; APS, antiphospholipid syndrome; aPLN, aPL nephropathy; SLE, systemic lupus erythematosus. Categorical variables are expressed as numbers and percentage; continuous variables are expressed as mean.
Referred to whole series.
There were no differences in the mean age of SLE patients at the time of renal biopsy between the different series. Similarly to the study from Tektonidou et al., 7 a longer evolution of SLE in patients with aPLN compared with those without aPLN was observed. However, no reasonable explanation for this finding was found. In agreement with the study from Cheunsuchon et al., 8 a higher chronicity index in the aPLN group was found. In our study, this finding could be closely related to a longer evolution of SLE in this group and to the fact that patients with aPLN had a higher prevalence of chronic renal lesions such as interstitial fibrosis, tubular atrophy, and arteriosclerosis. Delay in the lupus nephritis diagnosis might explain these renal functional characteristics and chronic histological findings. However, patients with aPLN had similar mean age at time of renal biopsy compared with the other two groups of patients.
Concerning the renal outcome, no differences in the presence of hypertension and nephrotic syndrome between the three groups were found. Conversely, serum creatinine levels were significantly increased at the time of renal biopsy and tended to be higher at the end of follow-up in cases with aPLN. Despite this higher prevalence of chronic lesions, no difference was observed in the frequency of renal failure or established renal damage at the end of follow-up between patients with and without aPLN. This discrepancy could be explained by the limited follow-up of our series. It is possible that with a longer time of follow-up, patients with aPLN could develop renal failure. In fact, the much longer follow-up in the retrospective studies was 7 years. 7,9 Another explanation is that patients with aPLN had a mild renal failure at the time of renal biopsy (mean creatinine of 1.7 ± 1.4 mg/dl) which was probably reversible with the immunosuppressive treatment.
In this sense, the higher prevalence of acute renal failure and ESRD described by Cheunsuchon et al. 8 may be explained by the Asian genetic background of the included patients with more severe initial renal function impairment and chronic, irreversible changes in the kidneys, probably unresponsive to immunosuppressive treatment.
Owing to the fact that all patients included in this study had SLE, we considered patients as having aPL if they had at least one positive determination of aPL at the time of renal biopsy. In fact, these patients persisted with positive aPL during the entire follow-up period. Interestingly, the present study demonstrated that in SLE patients with lupus nephritis, the presence of a single positive determination of aPL was enough to increase the risk of suffering from aPLN.
The presence of LA was more frequent in patients with aPLN compared with those without aPLN (77.8% vs. 41.7%). However, and conversely to previous studies, 6,7 the presence of LA was not statistically related to aPLN. This discrepancy could be explained by the low number of patients with aPLN.
Our study had some limitations. Owing to the retrospective design of our analysis, some points such as the potential protective role of anticoagulation could not be analysed. The small number of patients with aPLN might hamper the ability to identify some significant associations such as the relationship of LA and aPLN. We have considered as medium–high aCL levels those titres >26 GPL or MPL units. This is important, taking into account the fact that these titres have been previously related with a higher risk of thrombosis in patients with SLE. 16 In the data collected, the number of patients receiving antiaggregant therapy and/or anticoagulation at the time of biopsy was low; therefore the association between these drugs and the development of aPLN was not analysed.
In conclusion, aPLN occurred in 20% of SLE patients with aPL and in 0% of those without aPL, confirming the role of aPL in the pathogenesis of the renal lesions currently used for the definition of aPLN. Despite the higher prevalence of chronic lesions in patients with aPLN, no difference was observed in the frequency of renal failure or established renal damage at the end of follow-up between patients with and those without aPLN. Possibly, a longer follow-up could disclose a possible worse renal prognosis of aPLN. Prospective studies are needed to address the role of aPLN in the long-term outcome of SLE patients with positive aPL.
Footnotes
Funding
Francesc Sant, Department of Pathology, Fundació Althaia, was the recipient of a grant ‘Francisco Mampaso’ from the Spanish Nephrology Society, 2008.
Conflict of interest
The authors declare that they have no conflicts of interest.