
Abstract
The patient’s perspective of how their health affects their function is health-related quality of life (HRQOL). HRQOL is poorer in patients with systemic lupus erythematosus (SLE). Few HRQOL studies in SLE patients have focused on African Americans despite an increased disease burden compared with Caucasians. The African American Gullah population of South Carolina has a homogeneous genetic and environmental background and a high prevalence of multi-patient families with SLE. Demographics, medical history, and Short-Form 36 (SF-36) were measured within a cohort of Gullah SLE cases and related controls. Compared with related controls (n = 37), cases (n = 89) had a lower Physical Component Summary (PCS, 41.8 vs. 52.3, p < 0.01), but not Mental Component Summary (MCS, 55.0 vs. 56.0, p = 0.70). The difference in PCS was no longer significant upon adjustment for working status, disability, and medical conditions. None of the 11 SLE American College of Rheumatology criteria, disease duration, or Systemic Lupus International Collaborating Clinics Damage Index were associated with either PCS or MCS. Cases and controls had similar MCS scores. We hypothesize that this lack of effect of SLE on MCS may be due to disease-coping mechanisms interplaying with cultural factors unique to the Gullah.
Introduction
The way patients perceive the impact of disease on their physical, emotional, and social function, or health-related quality of life (HRQOL), is poorer in patients with systemic lupus erythematosus (SLE) compared with the general population, regardless of measure used. 1 Most studies to date have assessed HRQOL using generic measures such as the Short-Form-36 (SF-36), which is a comprehensive, general health survey with physical and mental health components. 2 SF-36 has been validated as a quality-of-life measure in SLE. 3 However, a limited numberofstudies have included African American patients. 4 – 6
African Americans have a three-fold increased prevalence of SLE, develop SLE at an earlier age, and have increased SLE-related morbidity and mortality compared with Caucasians. 7 – 11 We studied a unique African American cohort that consists of the Gullah population of the Sea Islands of South Carolina and Georgia. The Gullah are descendants of slaves brought over for rice farming in the 1700s from Sierra Leone and the Ivory Coast.12,13 It is estimated that between 100,000 and 300,000 Gullah live on the Sea Islands along the South Carolina coast and adjacent coastal communities. Relative geographic isolation has led to a greater genetic homogeneity with low non-African genetic admixture compared with other African American populations while cultural pride and close-knit family structures have limited environmental heterogeneity. 14 Further, it has been previously described that there is a high prevalence of multi-patient families with SLE within the Gullah population. 15
HRQOL in African Americans with SLE has not been well-characterized. Factors that may be associated with HRQOL, such as individual American College of Rheumatology (ACR) criteria for SLE, socioeconomic and disease factors, 4 also have not been thoroughly investigated. Furthermore, the close-knit family structure of the Gullah presents a unique opportunity to examine HRQOL in relatives of SLE patients to assess a potential caregiver effect. Understanding how SLE affects HRQOL has broad implications for the care of patients with SLE. Modifiable factors associated with HRQOL could be targeted for intervention to lessen the patient’s burden of disease. We conducted this study to quantify the impact of SLE on the HRQOL of the patient and their family members and to determine factors associated with a lower HRQOL.
Patients and methods
This research was carried out with the approval ofthe Institutional Review Board at the Medical University of South Carolina (MUSC). This case–control study was nested in a longitudinal observational cohort called SLE in Gullah Health (SLEIGH), which was started in 2002. A more complete description of the cohort has been previously reported. 15 Briefly, eligible cases were: 1) age two years and above, 2) self-identified as African American ‘Gullah’ from the Sea Island region of South Carolina, 3) diagnosed with SLE by meeting at least four of the 11 classification criteria as designated by the ACR,16,17 4) able to speak and understand English, 5) able and willing to give informed consent. Relatives of cases were also invited to enroll. Classification as Gullah required that the subjects self-identify and confirm that parents and grandparents were of Gullah heritage with no known ancestors that were not of Gullah lineage. Beginning in 2006, participants were asked to complete a SF-36 during a study visit at MUSC. Starting in 2009, participants were also mailed a copyof SF-36. Of the 605 total individuals in the SLEIGH cohort, 128 female subjects (91 cases and 37 related controls) attempted the SF-36 with 96completing the SF-36. Of those who attempted the SF-36, 112 (87%) were administered during a study visit and 16 (12.5%) were administered by mail. Two cases answered only the questions concerning demographics but none of the SF-36 questions and were therefore excluded, leaving 89 cases and 37 related controls included in this analysis.
We assessed HRQOL using the SF-36, version2. 18 Briefly, the SF-36 consists of 36 questions that are aggregated into eight domains of Physical Functioning (PF), Role-Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role-Emotional (RE), and Mental Health (MH). These eight domains are further summarized into the Physical Component Summary (PCS) and Mental Component Summary (MCS). PCS and MCS are both standardized to population norms with a mean of 50 and standard deviation of 10, range 0 to 100. Higher scores indicate better HRQOL.
Covariates used in our analysis included age, education, employment, disability status, medical insurance coverage, body mass index (BMI), comorbid medical conditions, current medications, disease duration, cumulative disease damage, and each of the 11 ACR classification criteria for SLE.16,17 Disability status was defined as currently receiving disability payments. Medical coverage was defined as receiving health care reimbursements from private insurance, Medicaid, Medicare, or military benefits. BMI was calculated from measured height and weight. Cumulative damage was measured using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI). 19 SDI was considered a dichotomous variable, no damage versus any damage. Comorbid medical conditions were self-reported, although in cases where medication use was not consistent with self-reported comorbidities, a chart review was undertaken to clarify the presence or absence of the condition. Comorbid medical conditions included diabetes mellitus, hypertension, hyperlipidemia, coronary artery disease, myocardial infarction, congestive heart failure, cerebral vascular accident, zoster, malignancy, Raynaud’s phenomenon, thrombosis, vasculitis, dialysis, osteoporosis, and a history of clinical depression.
Of the 605 participants in the SLEIGH cohort, we restricted our analyses to African American Gullah females who had attempted the SF-36 (n = 126). Only 66 cases and 30 controls completed every item of the survey, while 27 of the 30 with missing data were missing only four or fewer items.As ignoring those with incomplete data can introduce bias, we used multiple imputations to account for the small number of missing values. We performed analyses on both the subset with complete SF-36 data (n = 96), and on the full study population (n = 126) after using multiple imputations to estimate missing values.
Categorical variables were examined by Chi-square test and Fisher’s exact test as appropriate. Differences between the means of continuous variables were tested using Student’s t-test. We tested for differences in MCS and PCS, as well as in each domain, between cases and controls. We assessed therelationship between SF-36 and demographic and socioeconomic data, past medical history, and, among cases, each ACR criterion and SDI using multiple linear regression. Using the standardized mean of 50 and standard deviation of 10, with 89 cases and 37 controls we had 80% power to detect differences of 5.5 points for MCS and PCS, with an α of 0.05. Two-sided p-values < 0.05 were considered significant. All analyses were conducted using SAS 9.1 (SAS Institute, Cary, NC, USA). Multiple imputations were conducted using Proc MI.
Results
Characteristics of African American Gullah female SLE cases compared with related controls
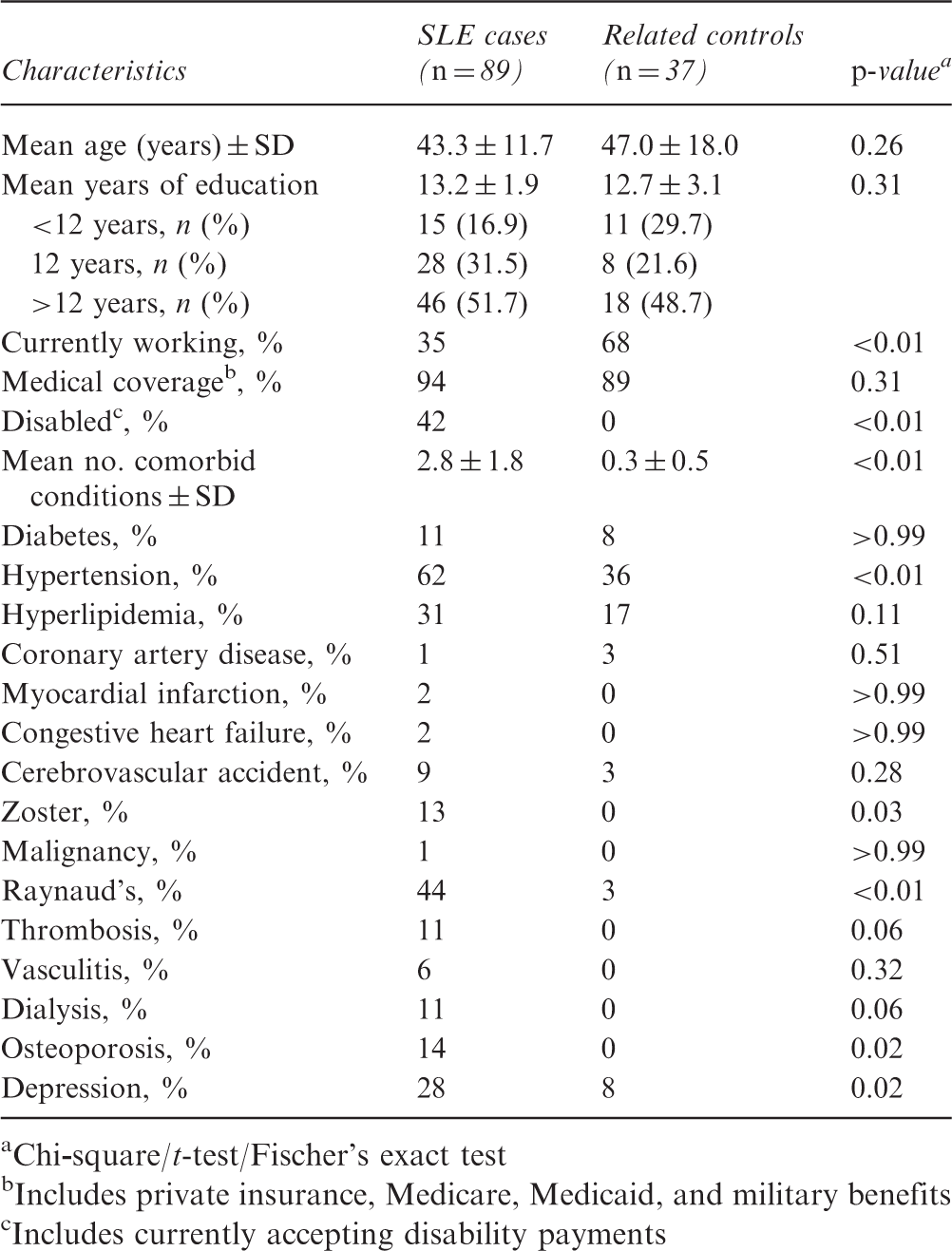
Chi
Includes private insurance, Medicare, Medicaid, and military benefits
Includes currently accepting disability payments
Disease characteristics among SLE cases
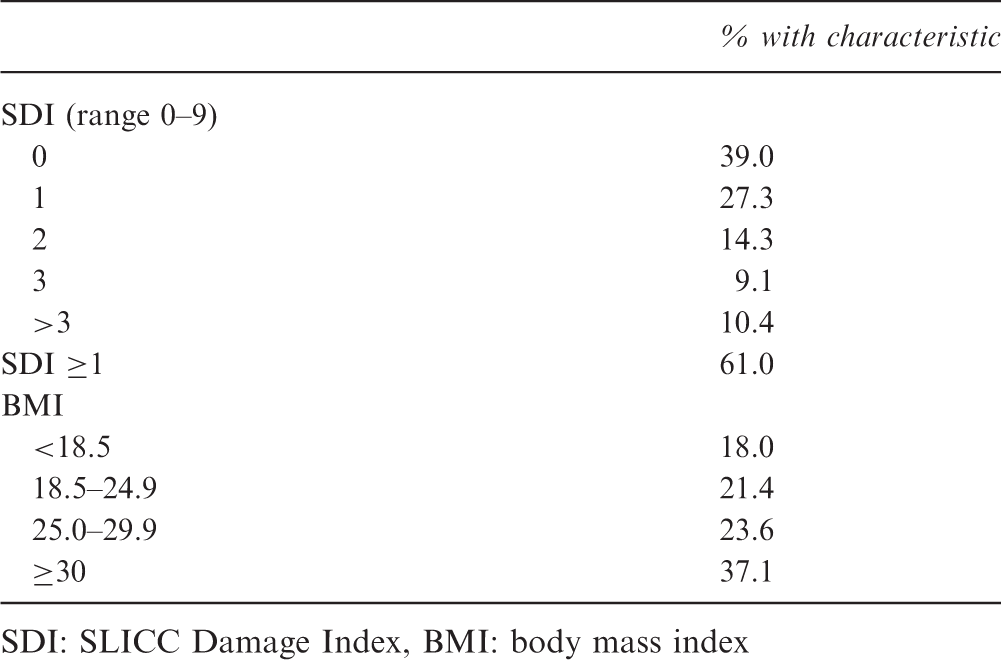
SDI: SLICC Damage Index, BMI: body mass index
Differences in summary and domain scores for HRQOL between SLE cases and related controls
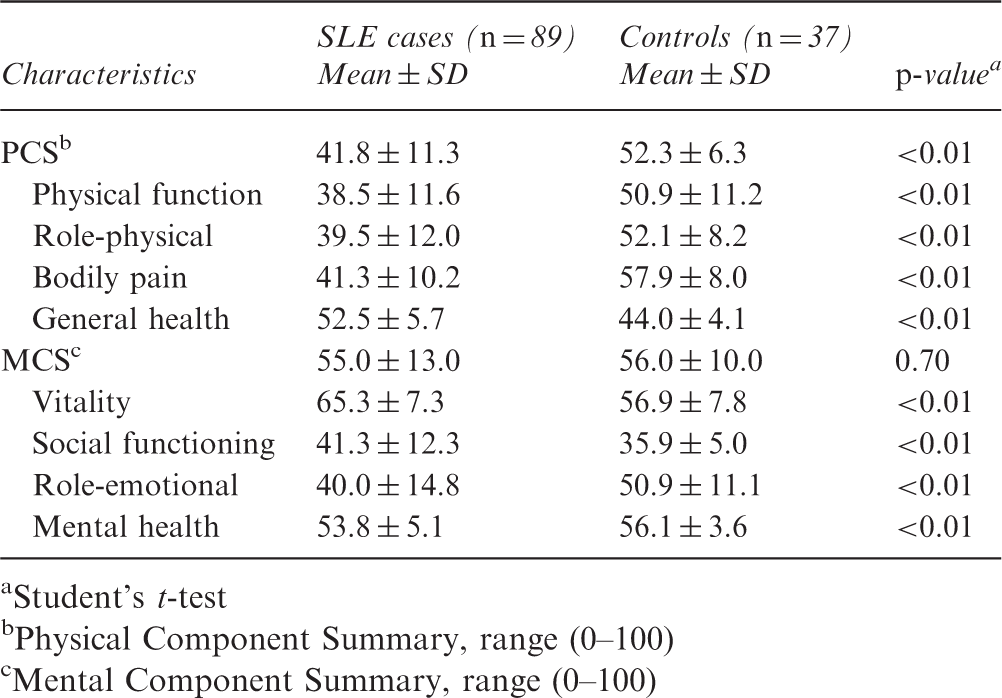
Student’s t-test
Physical Component Summary, range (0–100)
Mental Component Summary, range (0–100)
Compared with related controls, cases had a significantly lower PCS (42 vs. 52), but not MCS (55 vs. 56). There were significant differences between cases and controls for each of the four MCS domains (Table 3). This similarity in MCS scores could be explained by domains vitality and social functioning being significantly lower in controls and domains role emotional and mental health being significantly lower in cases. For cases, PCS and its four domains, except general health, all rated significantly lower than related controls. Compared with population norms, cases (42 vs. 50, p < 0.0001) but not controls (52 vs. 50, p = 0.0647) had a significantly lower PCS. However, both cases (55 vs. 50, p < 0.0001) and controls (56 vs. 50, p < 0.0001) had a significantly higher MCS.
Linear regression models for the association between SLE diagnosis and PCS and MCS before and after adjusting for potential confounders
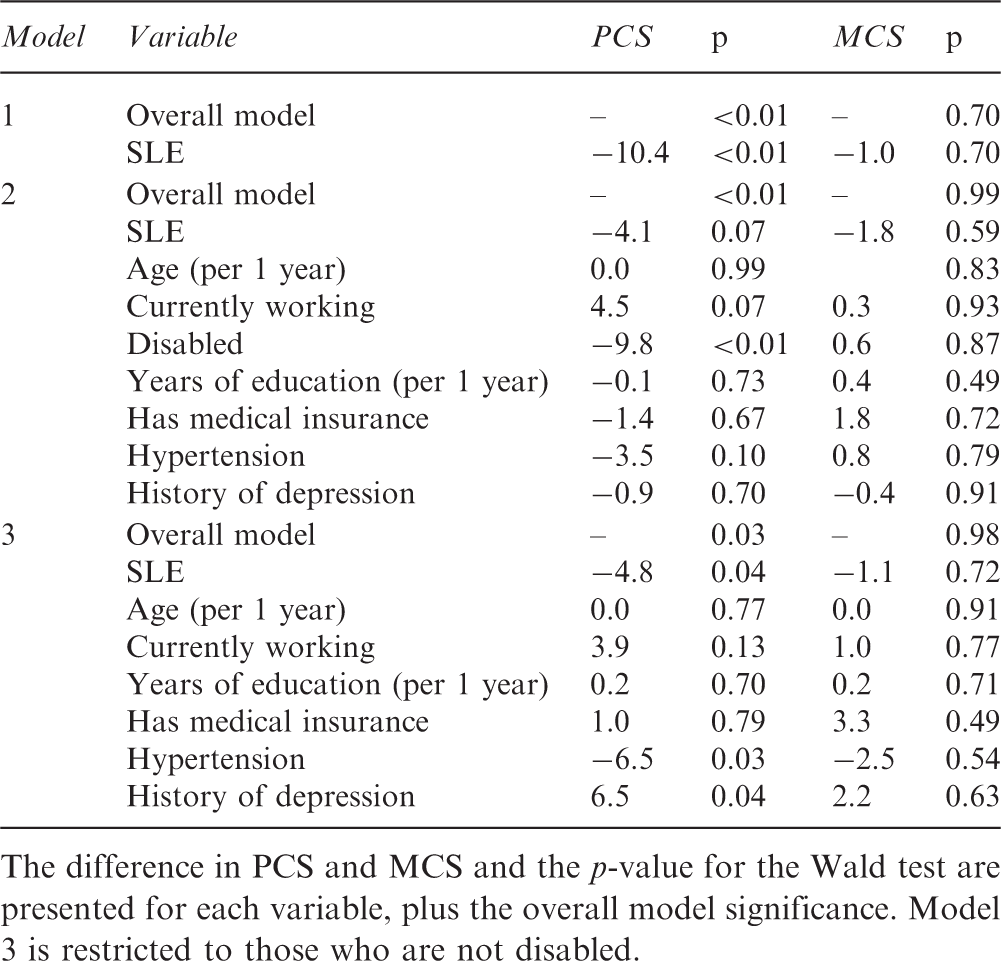
The difference in PCS and MCS and the p-value for the Wald test are presented for each variable, plus the overall model significance. Model 3 is restricted to those who are not disabled.
To determine whether individual ACR criteria or other disease-specific factors were associated with PCS or MCS, we restricted the following analyses to cases only. There were no significant differences in MCS for any individual ACR criterion, though nine of the 11 examined showed a lower score among those presenting with the criterion. In bivariate analyses for PCS, the presence of oral and/or nasal ulcers was associated with a score that was six points lower compared with those without it (p = 0.04) and renal disorder with a score 6.5 point higher (p = 0.02). Cases with renal criterion who were on hemodialysis or had undergone renal transplantation had a similar PCS and MCS (p = 0.27 and p = 0.47, respectively) compared with cases without these treatments (data not shown). There were no differences in PCS or MCS based on disease durationmodeled continuously or by quartiles, or by SDI modeled continuously or dichotomously (no damage versus any damage), though there were few individuals with SDI > 1.
Discussion
In this cohort of African American Gullah females, we found, as expected, that SLE cases had significantly lower PCS compared with related controls and population norms
In contrast, cases had a MCS similar to related controls that did not change following adjustment. Previous studies4,5 showed MCS to be significantly lower compared with population norms, while we found that MCS in our population was significantly higher than population norms. We hypothesize thatthe positive effect of SLE on MCS may be due to disease-coping mechanisms interplaying with cultural and religious factors unique to the African American Gullah. While we did not attempt to measure coping mechanisms, we know that within the Gullah population exists a close-knit family and community structure that would allow for the kind of social support that has been associated with increased HRQOL in some SLE cohorts,20,21 but not all. 22 Further, in the Gullah population, there is a high prevalence of multi-patient families with SLE that would allow for unique support for SLE.13,15
Older age was associated with lower HRQOL scores in related controls but not cases. While there is a predominance of studies showing older age having a negative impact on HRQOL, there are a few studies showing no effect of age on HRQOL using SF-36 version 1. 23 – 25 Longer duration of disease was not associated with HRQOL, as others have observed;21,26 however, this has been an inconsistent finding in the literature. 1
Although over half of the patients with SLE hadsome disease-associated damage at the time of SF-36 administration, their SDI score was not associated with HRQOL. Similar to disease duration, there has been an inconsistent association between SDI and SF-36 scores in the literature. 1 One study followed changes in SF-36 scores over two years, finding that only new organ damage assessed by SDI, rather than total damage, was associated with decreases in HRQOL. 27 We had multiple surveys for very few of our cohort members, so we were unable to conduct these analyses. Our observations of age, disease duration, and SDI not correlating with HRQOL could be consistent with our hypothesis that coping mechanisms may be affecting HRQOL in our cases. Over time, cases may adapt to their disease and its associated morbidity and disability. One recent study found that HRQOL in patients with SLE was influenced by coping capacities to deal with health-stressors measured by the Sense of Coherence scale, an effect unique to SLE when compared with other chronic rheumatic diseases. 28 Coping mechanisms have been suggested in another HRQOL study where end-stage renal disease patients with SLE did not have significantly lower SF-36 scores compared with SLE patients with preserved renal function. 24
The vitality domain in cases had the highest score of any in our study (65.3). The questions contributing to this domain focused on fatigue. Fatigue is among the most prevalent and debilitating symptom for SLE patients, with reported prevalence from 50% to 85.7%.1,29 Interestingly, our cases scored significantly better than the general population and to African Americans in another SLE cohort in the vitality domain.
5
Cultural religious influences unique to the Gullah
The domain scoring lowest for both cases and controls was social functioning, with controls having lower scores (35.9) than cases (41.3). The questions contributing to this domain asked how often physical or emotional health has ‘interfered with normal social activities’ during the past four weeks. The strong effect among controls was unexpected, though might suggest a large caregiver burden in our population. While not widely explored in the rheumatology literature, the negative impact on caregivers for those with chronic disease and the need to address their well-being is well established.31,32 Anecdotally, the majority of our controls were parents or children of cases who played a large caregiver role.
Consistent with previous studies in SLE and other chronic diseases, disability was a strong predictor ofPCS, with lower scores among those reporting disability. The interpretation of this finding is confounded by the fact that only cases were disabled, thus it is difficult to determine to what extent the case status was contributing to a lower PCS versus the disability. We performed a subset analysis of subjects without disability and found that case status, hypertension, and a history of clinical depression were associated with significant differences in PCS. Those with SLE had a PCS that was 4.8 points lower than those without SLE.
Curiously, a history of clinically diagnosed depression did not correlate with MCS overall or three of its subscales, but was associated with the role emotional subscale. It is possible that depression was not current or was well managed at the time the respondents took the SF-36. However, a history of depression was also significantly associated with a nine-point increase in PCS. Of note, cases that were diagnosed with depression were also receiving medical attention for the condition. A small randomized study showed that cognitive-behavioral therapy in SLE patients improves not only MCS and its components, but also physical components of HRQOL. 33 Thus, the increase in PCS may be attributed to the treatment of the depression, not the depression itself.
Our study had a number of limitations. Because of our unique population, we had low numbers of participants. Nonetheless, we not only were able to detect significant differences in HRQOL that had been shown in other populations,4,5 but we also identified new factors contributing to HRQOL, signaling that our study sample was sufficiently large for our main analyses. In addition, the use of related controls, as opposed to other methods of selection, may have reduced the number included. However, it ensured that we had cases and controls with similar genetics and environments. Our population was restricted to African American Gullah females with SLE and their female relatives, and so our results from this specific population may not be generalizable to the broader population. As is common with survey-driven studies, we had a fair amount of missing data. Using multiple imputations to account for missing values, however, our conclusions did not change, suggesting that the missingness in our dataset had a minimal impact. There is also the potential for a number of selection biases to impact our findings, such as by education and disease damage. However, of the survey respondents, there was a broad distribution of years of education (Table 1) and disease damage (Table 2), so it is unlikely that our results are biased by these two factors.
One could argue that SF-36 has its limitations in describing HRQOL in SLE. Our finding of MCS scores above the general population in cases despite a significant rate of depression warranted concern. While the SF-36 has been validated in SLE, 3 other disease-specific measures have been developed including the LupusQol-US© 34 and the LUPUS-PRO 35 that may be more sensitive to detect SLE’s impact on HRQOL, although findings are not consistent. 36 These were not used as they had not been validated in the literature at the start of ourstudy and also could not be used in related controls. Further, our goal was to use the SF-36 domain scores to identify areas of intervention to improve HRQOL. Not only did we fail to observe any associations with disease-specific measures, but it is also unclear whether these domains translate into a clinically meaningful construct that could be targeted. Domain and summary scales of the SF-36 were all significantly higher than expected so that only a limited number of domains could be identified to target interventions. Our unexpected finding of fairly high SF-36 scores also sheds light on the consideration that interventions designed to improve HRQOL in SLE should not only be age, gender, and race specific but also culturally and regionally specific.
In this cohort of African American Gullah females, we saw that the physical, but not mental, component of HRQOL was impaired in cases versus related controls. These differences were largely attributable to disability and other comorbid conditions. We did not identify any disease-specific variable that was strongly associated with HRQOL. Rather, the pattern of elevated scores relative to the general population and other SLE cohorts may indicate a set of coping skills unique to the Gullah population.
Footnotes
Funding
This work was supported by the National Center for Research Resources, National Institutes of Health (MUSC’s CTSA grant UL1 RR029882).
Conflict of interest statement
None declared.