
Abstract
Introduction
Systemic lupus erythematosus (SLE) is an immune-mediated connective tissue disorder with strong gender and ethnic biases. Most affected women are of childbearing age and pregnancy is a frequent event.1,2
Pregnancies in women with SLE are high-risk due to increased rates of maternal and fetal complications. Initial reports of pregnancy in SLE suggested poor outcomes, 3 but recent data show dramatic improvements in live birth rates.4,5 Pregnancy in SLE must be considered from three perspectives: the effect of pregnancy on disease activity/progression; effects of disease/treatments on the fetus; and the health of the mother during pregnancy and after delivery.
The literature related to fetal and maternal outcomes in SLE pregnancies is growing. However, a wide variety of study designs and definitions of lupus and complications are used. Reviews focus on end points related to fetal outcome and maternal complications. A recent meta-analysis, covering 2751 pregnancies in women with SLE and lupus nephritis (LN), identified high maternal complication rates and an overall maternal mortality rate of 1%. 6 The causes of these deaths were not discussed, and to date there has not been a formal analysis addressing the issue of maternal death in women with SLE, and in particular, LN. One review of pregnancy outcomes in patients with LN raised concerns that sepsis, not disease activity, may be the leading cause of maternal mortality. 2 The most recent Centre for Maternal and Child Enquiries Report (2006–2008) notes that although maternal mortality has declined in the United Kingdom, maternal mortality rates attributable to sepsis have risen. 7 This highlights the challenges of diagnosing and treating sepsis during pregnancy, even in an immune competent population.
In this study, we perform a review of the literature for maternal deaths in women with LN to: (1) identify the main causes of death and (2) discuss possible reasons for these causes, and approaches aimed at improving patient care and outcomes.
Methods
We performed an extensive electronic literature search from 1962 to 2009 using online databases (PubMed, Embase, Lilacs, Cochrane Controlled Trials Register, Medline, and Science Citation Index). The abstracts and full text for all papers identified using the keywords ‘SLE’, ‘lupus nephritis’, and ‘pregnancy outcome’ were reviewed. Studies were included if they reported pregnancies in patients with LN with at least one reported death. As most papers were case series, quality scores were not applied, but validation criteria were applied as follows.
Definitions
The presence of SLE was defined by the American College of Rheumatology diagnostic criteria appropriate to the age of the article. 8 Maternal mortality was defined as that occurring during pregnancy, or during the early post-partum period, defined as the 6 weeks (42 days) following pregnancy termination/delivery. The presence of LN was defined by histology, where available, and graded by either the Comerford and Cohen classification 9 and, more recently, the 1995 World Health Organization classification. 10 Where histology was not reported, terms such as ‘inactive renal disease’ and ‘quiescent nephritis’ were accepted as representing sufficient diagnostic certainty on the authors’ part, to record these patients as having LN in remission. Active nephritis was defined as proteinuria >500 mg/day, with >5 red cells per high power field (or other evidence of an active sediment). An elevated creatinine was not necessary to define active nephritis. Most patients presenting with de novo LN during pregnancy did not have a histological diagnosis. Renal disease flares were defined by elevations in urinary protein levels above 300 mg/day (physiological proteinuria of pregnancy) with autoantibody status and complement levels used to distinguish disease flares from preeclampsia.
Information on the number of pregnancies and proportions of patients with LN diagnosed prior to/during pregnancy was extracted and tabulated. Where LN was diagnosed prior to pregnancy, the cases were separated into active or inactive at conception.
Results
One hundred and thirty-six papers were identified from the initial database searches. Of the 136 papers, 63 were excluded, leaving 73 original papers for analysis; 59 papers did not report maternal mortality, leaving 14 papers with potentially relevant information.
11
–
24
Of these, it was unclear in one of the articles if the death occurred in a LN patient – this was also excluded
22
(see Figure 1).
Flow chart of study selection.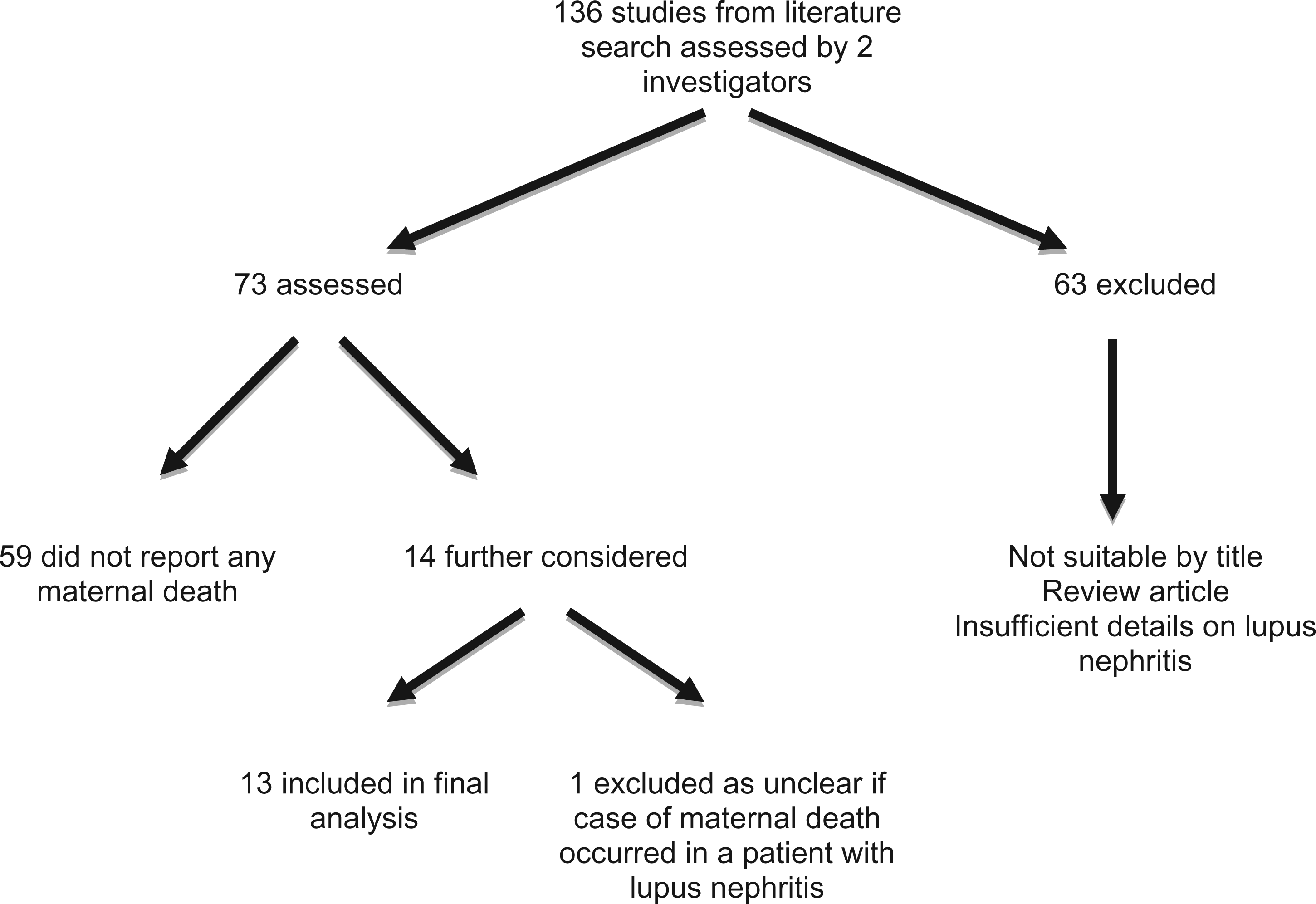
These 13 studies reported 19 deaths in patients with LN. A death occurred 18 months post-partum due to pancreatitis 15 and was excluded from the analysis, leaving 18 reported deaths in the immediate peri-partum period. A death due to Bacillus cereus sepsis was reported in 2 articles, leaving 17 unique cases.16,18 The extent of information pertaining to immunosuppression/histological classes varied among studies, but causes of death were reported for all cases, but one.
Details of cases of maternal death included in analysis
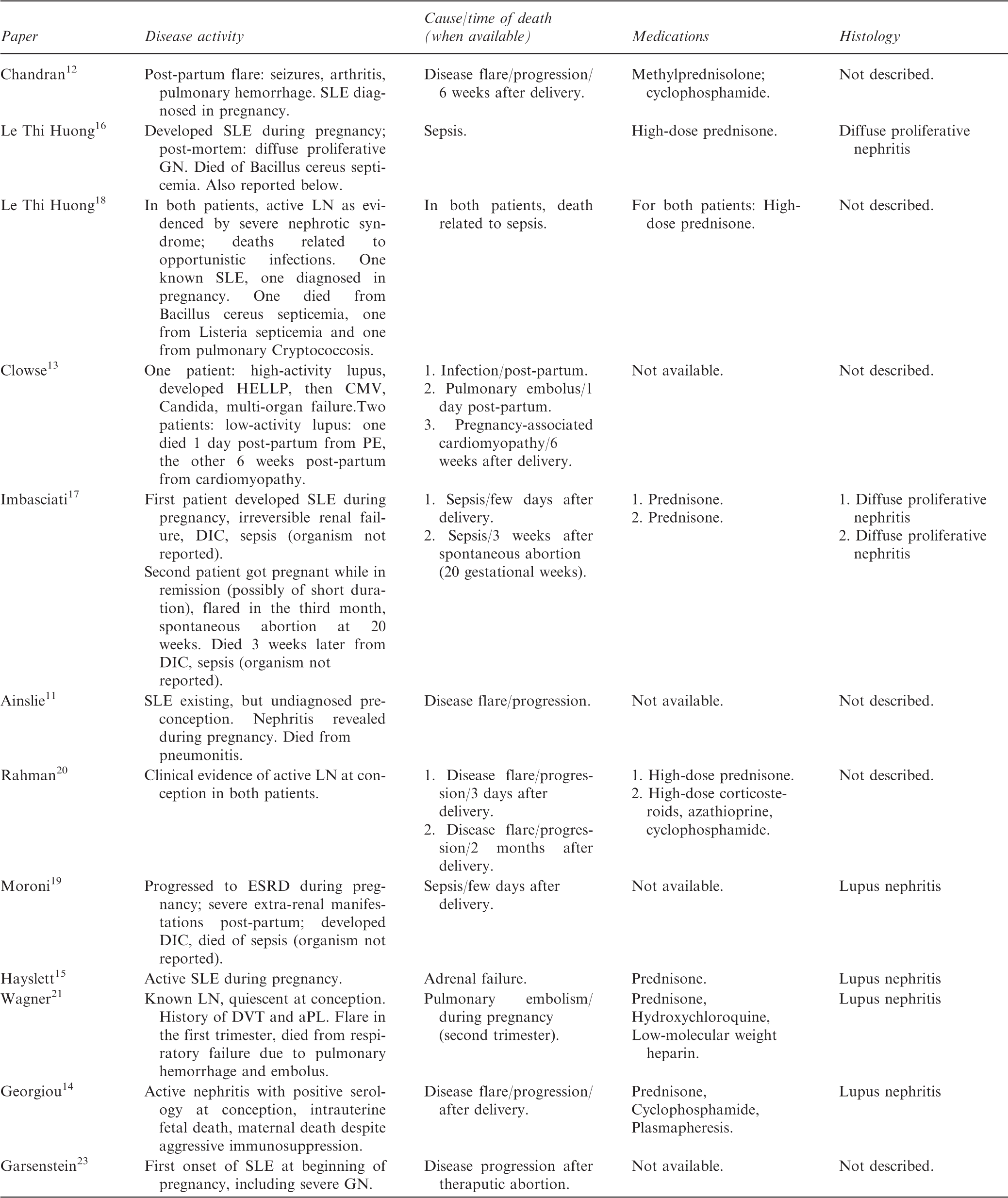

GN: glomerulonephritis; DIC: disseminated intravascular coagulation; ESRD: end stage renal disease; PE: pulmonary embolus; aPL: anti-phospholipid antibody.
Confounding effects of sepsis and opportunistic infections
In cases of mortality due to infection, there were insufficient data to comment on laboratory parameters, including white cell count, at the time of infection. The infectious agent was not always identified, but in the four cases where it was reported, three patients died with infection due to opportunistic intracellular organisms. Listeria, Bacillus cereus, Cryptococcus, Cytomegalovirus (CMV), and Candida, were all implicated agents (multiple organisms were identified in some patients). During pregnancy, all 11 patients for whom details of immunosuppression were reported received corticosteroids, with 5 of these patients described as receiving high dose steroids. Of these five patients, three died of active disease and two of opportunistic infections. In the third patient, who died of opportunistic infection, details of immunosuppression were not reported. Azathioprine and hydroxychloroquine were given to one patient each, and cyclophosphamide was administered to three patients immediately after pregnancy termination (Table 1). Information regarding the drug dosing and duration of treatment was mostly incomplete.
Other causes
Disparate pathologies were implicated in the remaining cases. Steroid withdrawal was implicated in one case. Theoretically, this may have worsened disease control, although no data were reported to support this hypothesis. PE was reported as the cause of death in two patients, one with antiphospholipid syndrome (APS), as confirmed by the presence of antiphospholipid antibodies (aPL) and a history of deep vein thrombosis. One patient developed pregnancy-associated cardiomyopathy and died 6 weeks post-partum.
Cases with intra-partum onset of lupus nephritis
A total of 6 studies reported patients presenting with de novo lupus nephritis during pregnancy, with 26 pregnancies in this group. 11 –13,16– 18 Three deaths were identified, two due to infection and one due to disease flare.
Discussion
Our study demonstrates that all maternal deaths in patients with SLE and LN occurred in those with active disease. In all cases where immunosuppression was documented, steroid therapy had been used. The major cause of maternal death was infection, with three of four deaths reported due to infection with opportunistic organisms. The second most common cause of maternal death was disease activity. The presented evidence supports current recommendations that the disease should be quiescent on stable therapy for a substantial period (often defined as ≥ six months) prior to conception. 25 This may decrease complication rates due to disease activity, and may lessen the use of aggressive immunosuppressive therapy, thus lowering rates of opportunistic infections and related deaths. When LN presents de novo in pregnancy, a logical presumption is that disease activity would have the greatest bearing on outcome. Our review emphasizes that even in this setting, infection contributes to adverse maternal outcomes.
Additional cases of maternal mortality were retrieved during the literature search, but did not meet the criteria for inclusion as defined above. For example, in a study of 134 patients with SLE and their 191 pregnancies, ‘nephritis’ was listed as the cause of death in 5 of 12 reported deaths. However, the information regarding the disease activity and severity, as well as the exact timing of death was incomplete, thus not allowing for detailed analyses of these events. Of note, in this series, only 1 patient died during her pregnancy, while 11 died during the post-abortal or post-pregnancy period. 26 Another report included three cases of maternal death that occurred at 13, 20, and 28 weeks post-partum, in association with SLE activity. 23 Taken together, the published evidence suggests that the risk for maternal mortality is particularly high in the post-partum period, and that SLE exacerbations occurring weeks after delivery may contribute to maternal mortality, thus justifying close monitoring of these patients.
Several lines of evidence support the complex interactions between disease activity and infections. These interactions may be modified by immunosuppressive drugs and, in pregnant patients, may be further potentiated by hormonal/immunological changes. During pregnancy, the maternal immune system adapts to allow for the growth of a semi-allogeneic fetus. Significant immunological changes ensue,27,28 including inhibited cytokine production by type-1 helper cells (Th1), and enhanced cytokine production by type-2 helper cells (Th2) (related to the cellular and humoral immune systems, respectively). It has been suggested that up-regulation of Th2 cytokines in pregnancy may increase the risk for Th2-mediated diseases, such as SLE. However, the role of pregnancy in causing SLE flares remains controversial. Similar to pregnancy, SLE is an immune-compromising condition, with reports of increased vulnerability to infectious agents. 29 The sum of the hormonal and immunological changes in pregnant patients with SLE may play an important role in elevating the risk of a disease flare, and creating an environment predisposed to overwhelming infection. The challenge of balancing immunosuppression, given the altered metabolism of some agents during pregnancy, highlights the importance of planned pregnancies for this patient group.
Immunosuppression during pregnancy
Most patients received steroids, azathioprine, and hydroxychloroquine during pregnancy, which, with respect to fetal well-being, are considered to be relatively safe. 30 However, induction regimens for treatment of autoimmune disease and use of steroids are associated with high relative risks for major infections. 31 These medications may have heightened the risk of infection in these women. These medications also induce lymphopenia, which may be further potentiated in pregnancy when, relative to the total white blood cell count, the lymphocyte count drops and begins to rise only after delivery. 32 The importance of a mean nadir lymphocyte count as a predictor of major infection has been shown in non-pregnant patients with SLE and ANCA vasculitis managed with regimens that do not cause severe neutropenia. 33 Thus, immunosuppressive therapy may have contributed to the high rate of infections in this patient cohort. In particular, it is of note that the infectious deaths in patients who were reported as receiving high dose steroids were all due to opportunistic infections.
Not all immunosuppressive agents result in the same risk of infection in SLE patients. Steroids are reported to significantly increase infection risk, while anti-malarial agents have the opposite effect. 25 In addition, these data identified LN treated with immunosuppressive therapy as a significant risk factor for serious infections. In this cohort, most patients had either clinical or biopsy-proven evidence of LN.
Opportunistic infections
In this cohort, Candida, Listeria, Bacillus cereus, Cryptococcus and CMV were implicated agents. Most of these pathogens are predominantly intracellular organisms. While this is likely a reflection of the degree of immunosuppression, inhibited Th1 T-cell responses may have had a contributory effect. 28
Atypical infections, such as CMV and Cryptococcus, are challenging to diagnose and treat.34,35 Cryptococcus most commonly affects the central nervous system, with steroid therapy being a major risk factor for its development. 35 Other invasive fungal infections, including organisms such as Candida and Aspergillus, appear to be more common in patients with nephritis. 36 Given the atypical nature of these infections, it is imperative that they are considered, along with atypical sites for localization. Uncommon presentations of rare infective agents should also be considered. Bacillus cereus (noted as a cause of death in this review) is normally associated with indwelling lines and neutropenia, but has been reported in a SLE patient with neither of these risk factors. 37
Disease activity
Our data suggest that the combination of disease flare and infection may be more common than generally recognized. Elevated SLEDAI scores correlate with more frequent infections, and worse outcomes.36,38 Hypocomplementemia, which commonly accompanies SLE flares, is a predictor for infection, independent of immunosuppressive therapies. 38 Conversely, infection may influence disease activity, with studies showing that some infectious agents (notably CMV) can precipitate SLE flares.39,40 Disease activity scores, such as SLEDAI-2K, have a role in predicting a heightened risk of flare during pregnancy. 41 Pregnancy-specific scores, such as the Lupus Activity Index in Pregnancy, 42 are validated for their abilities to predict flares, 43 but are used for research purposes, not in clinical practice.
Histological subclass
A previous meta-analysis of SLE pregnancy outcomes did not find a statistically significant link between histological class and adverse pregnancy outcomes due to limited data availability. 6 In this review, not all cases reported histological subclass, nor were there sufficient cases to establish a comparator group. As such, it is not possible to comment on the potential relationship between the histological class of LN and maternal mortality outcomes. Importantly, renal biopsy is rarely performed close to or during pregnancy. This avenue may merit further investigation, as histological subtype and disease activity may be important confounding variables for mortality.
Maternal complications
Thrombo-embolic disease was the cause of death in two patients included in this review. Low molecular weight heparin therapy is used for patients with aPL or APS. 44 However not only lupus,45,46 but pregnancy as well, may contribute to a pro-thrombotic state (potentially due to endothelial activation), even in patients without aPL and/or renal disease at the point of conception. In addition, proteinuria may result in urinary loss of anti-thrombin III, further increasing thrombotic risk. Future studies are needed to provide guidance as to the optimal modalities and timing of anticoagulation in pregnant SLE patients.
Of note, there were no reported deaths related to preeclampsia/eclampsia. One death was associated with HELLP syndrome, believed to be a severe variant of preeclampsia associated with Hemolysis, Elevated Liver enzymes, and Low Platelets. While SLE does not increase the risk of this condition to the same extent as previous preeclampsia (OR 7.19) or primary APS (OR 9.72), it is a recognized risk factor. 47 Preeclampsia may also be associated with more severe histological classes of lupus nephritis. 48 Recent work suggests mutations in the genes coding for complement regulatory proteins may be associated with preeclampsia in SLE and/or aPL patients. 49 Eclampsia and preeclampsia should remain concerns, and differentiating preeclampsia from a disease flare is difficult, as both cause increasing proteinuria, rising blood pressure, and thrombocytopenia. 50 A LN flare is more likely when there is active urinary sediment, low complement levels, increased anti-DNA antibodies, and extra-renal lupus manifestations. Elevated uric acid levels make the diagnosis of preeclampsia more likely. 51
Finally, studies suggest that an abnormal second trimester Doppler flow wave in the maternal uterine artery help predict development of preeclampsia in this population, but this would not exclude the risk of flares. 51, 52
Conclusion
This review of pregnancies complicated by LN highlights the significant risk of maternal mortality in these patients. Most of the reported deaths occurred after delivery, likely reflecting a proactive approach in the management of patients with severe disease who, despite pregnancy termination, further progress and succumb to SLE- and LN-related complications. 23 In addition, pregnancy termination may allow for more aggressive immunosuppression which, in turn, may contribute to maternal deaths due to opportunistic infections. Importantly, all deaths occurred in patients with active disease, with infection and disease activity being the two major causes of maternal death. A major limitation of this study is the lack of a control group of pregnancies not resulting in death in patients with SLE or LN, which would allow for comparative analyses of risk factors for maternal death. Despite this limitation, our findings provide support for the current recommendations calling for avoidance of pregnancy until all manifestations of SLE are quiescent, with the patient on stable immunosuppression. This may decrease rates of complications, including maternal death, due to disease activity. Additionally, use of aggressive immunosuppression might be reduced, also lowering rates of opportunistic infections and maternal death. As a corollary, physicians must be vigilant when using immunosuppression in pregnancy and may consider focusing on lymphocyte count and T-cell subsets to guide therapy. The potential for a disease flare to lead to a severe infective episode must also be considered. Overall, a balanced (i.e. risk of infection versus treatment benefit) approach to immunosuppression is a vital tool in managing these patients.
Other approaches should be considered and there may be a role for preventive strategies. Insufficient data exist to comment on medical prophylaxis for viral/fungal infections, but this area merits further study. Pre-conception vaccination may be another consideration, as could measurements of antibody levels against encapsulated organisms. An inactivated Varicella zoster vaccine has been evaluated in patients undergoing autologous stem cell transplantation. This reduced herpes zoster episodes over the subsequent 12 months, 53 and remains an interesting avenue for future therapy, as does the development of a CMV vaccine.54,55 Routine infection control measures, such as avoidance of in-dwelling catheters, should be entertained. This review emphasizes the importance of pre-pregnancy counseling and the close monitoring of affected pregnancies. The paucity of literature on such serious outcomes suggests that a patient registry would be the most effective way to improve knowledge and outcomes.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
*
J Ritchie and A Smyth contributed equally as first authors