
Abstract
Kidney biopsy is essential for the diagnosis and management of lupus nephritis. The risk of bleeding complication, however, is not defined in the systemic lupus erythematosus population. A retrospective cohort study was conducted to determine predictors of major and minor complications among patients with systemic lupus erythematosus undergoing percutaneous ultrasound-guided kidney biopsy. Major complications included bleeding necessitating intervention, hypotension requiring vasopressors or higher level of care or death. Minor complications included moderate or large (≥ 4 cm in largest diameter) perinephric hematoma, gross hematuria or voiding difficulties. All patients were observed for at least 23 h post-procedure. The overall incidence of bleeding was 10.5% (2.7% major, 7.8% minor). Adjusted logistic regression showed that for every 10,000 cells/mm3 decrease in platelet count, risk for major and any complication increased by 27% (odds ratio 1.27; 95% confidence intervals 1.06–1.51; p = 0.01) and 8% (odds ratio 1.08; 95% confidence intervals 1.02–1.15; p = 0.01), respectively. Patients with a platelet count <150,000 cells/mm3 were 30 times more likely to experience a major complication (p = 0.002). Other candidate predictors, including steroid exposure, kidney function, hematocrit and histopathology, were not significant. Kidney biopsies are well tolerated in patients with systemic lupus erythematosus. However, patients with pre-biopsy platelet counts <150,000 cells/mm3 are at markedly increased risk for a major bleeding complication.
Introduction
Systemic lupus erythematosus (SLE) commonly presents with kidney involvement and is associated with increased morbidity and mortality. 1 While the clinical course may vary from patient to patient, 10–60% of patients with lupus nephritis may eventually go on to develop end-stage kidney disease. 2 A delay in treatment may result in progressive renal failure whereas inappropriate use of immunosuppressive and cytotoxic agents can cause great harm to the patient. Timely diagnosis and proper treatment are therefore critical in patients with lupus nephritis. 3
The kidney biopsy is the single most important diagnostic tool in the management of lupus nephritis. While clinical and laboratory data such as hematuria, proteinuria, cellular casts, or rise in serum creatinine may suggest renal involvement, the underlying histopathology cannot be determined unless a biopsy of the kidney is performed. 4 Of the six possible classes of lupus nephritis, as defined by the International Society of Nephrology and Renal Pathology Society (ISN/RPS), patients with proliferative forms of disease (III or IV) generally warrant more aggressive therapies. 3 Moreover, activity and chronicity indices, also determined by kidney biopsy, provide a semi-quantitative assessment of disease activity that can be used to guide treatment. 4 For these reasons, a kidney biopsy should be pursued when possible.
Biopsying the kidney, however, is an invasive procedure and associated with several potential risks. Bleeding, the most serious of these complications, may require blood transfusion, arterial embolization under fluoroscopy or even nephrectomy. Other risks include patient discomfort, infection, unintentional injury to other organs or death. Percutaneous approaches, under ultrasound or computed tomography guidance, are most commonly used today. Alternative approaches include transjugular, laparoscopic, transurethral, and open surgical biopsies, but these techniques carry with them their own set of risks. 5
Fortunately, the advent of real-time ultrasound guidance has markedly improved the ability to obtain adequate tissue without compromising patient safety. Previous studies have investigated predictors and timing of complications in the general population.6,7 Nevertheless, there remains a paucity of data on such risks in the SLE population. Patients with SLE often have concurrent hematologic abnormalities, including anemia and thrombocytopenia. Furthermore, a subset of these patients may also have anti-phospholipid antibody syndrome necessitating peri-procedural anti-coagulation therapy. Such hematological disorders could theoretically increase the risk for post-biopsy complication.8,9 We aimed to better define the incidence and predictors of major and minor complications in patients with SLE undergoing renal biopsy to facilitate physicians in determining those patients most appropriate for such a procedure.
Materials and methods
Study population
A retrospective cohort study of 219 consecutive individuals aged 18 years or older with a clinical diagnosis of SLE, as determined by a rheumatologist, who underwent a percutaneous kidney biopsy from March 1993 to December 2007 at a single tertiary care academic center was conducted. For those patients who had multiple biopsies during this time period, only the first biopsy was included in the analysis. As per standard practice at our institution, patients were required to have a systolic blood pressure ≤160 mmHg, diastolic blood pressure ≤100 mmHg, platelet count ≥50,000 cells/mm3, international normalized ratio <1.3 s and partial thromboplastin time <42.1 s before proceeding with biopsy. For each patient, blood pressures were checked just prior to biopsy and, if elevated, pharmacologic therapies were given to ensure a measurement of ≤160/100 mmHg at the time of biopsy. The blood pressures used in this analysis, however, were obtained from the most proximal clinic visit, as these were often the only records available. For those patients who did not initially meet the above laboratory criteria, transfusion therapies could be provided. Patients on aspirin or clopidogrel were instructed to discontinue these drugs for 5 days prior to the date of biopsy; desmopressin (DDAVP) was not used prior to nor following any biopsy. All patients who underwent a renal biopsy were included in the analysis. The study was approved by the Johns Hopkins University School of Medicine Institutional Review Board.
Prior to each kidney biopsy, informed written consent was obtained. Biopsies were performed by attending nephrologists or by nephrology fellows directly supervised by attending nephrologists. All biopsies were performed using a semi-automated 18-gauge needle with real-time ultrasound visualization provided by experienced radiology technicians; those performed after December 2001 also used a needle-guide device attached to the ultrasound probe. Two to three cores of tissue were generally obtained per biopsy, as our institution does not have pathology technicians available to ensure sample adequacy during each biopsy. To evaluate for any signs of complications, all patients were monitored for a minimum of 23 h (bed rest for at least 6 h) post-procedure with frequent vital sign checks, repeat hematocrit measurements and follow-up imaging if clinically indicated.
Outcomes
The primary outcome was any bleeding complication, further categorized as major or minor, associated with the biopsy. Consistent with previous studies, major complications were defined as bleeding requiring packed red blood cell transfusion, interventional radiology or surgery; hemodynamic instability requiring transfer to a higher level of care or need for vasopressors; or death. Minor complications were defined as the development of a perinephric hematoma that was ‘moderate’ or ‘large’ by description or ≥ 4 cm in largest diameter; difficulty voiding necessitating urinary catheter placement; or gross hematuria. Only those patients with signs or symptoms concerning for bleeding underwent post-procedure imaging.
Candidate predictors
Information on potential predictors of interest was abstracted from patient electronic medical records. Sociodemographic variables included age at the time of biopsy, gender and race. Clinical variables included pre-biopsy blood pressure (systolic, diastolic and mean arterial), history of diabetes and/or hypertension, concurrent diagnosis of anti-phospholipid antibody syndrome, prednisone use and ISN/RPS class of kidney involvement. Laboratory variables included pre-biopsy hematocrit, platelet count, blood urea nitrogen, serum creatinine, albumin, erythrocyte sedimentation rate and the presence of nephrotic range proteinuria (>3.5 g/day). Glomerular filtration rate (GFR) was estimated using the four-variable Modification of Diet in Renal Disease (MDRD) equation.10,11
Statistical analyses
Data were analyzed using STATA statistical software (Version 11, 2009; College Station, TX). The most recent laboratory values and blood pressure parameters available prior to biopsy were used in the analysis. Baseline characteristics comparing patients with any bleeding complication to those without complication were conducted using Student’s t-test and Wilcoxon rank-sum test for continuous variables and Fisher’s exact test for binary and categorical variables. For each outcome (any, major or minor complication), simple logistic regression analysis was performed with each candidate predictor and the Wald test was used to identify potentially important predictors of bleeding. Multiple logistic regressions were then conducted with likelihood ratio testing and Akaike’s information criteria to determine the best model for each outcome of interest. Of note, systolic blood pressure and pre-biopsy hematocrit were included in all multivariable analyses, as these variables were determined a priori to be clinically relevant. As more than half of the biopsies were performed by a single attending physician, attending status was included in all three final models to control for potential confounding. Effect modification was evaluated by inclusion of interaction terms. Sensitivity analyses included the use of exact logistic regression, particularly for the outcome of major complications, which had only six events. While computationally intensive, exact logistic regression does not rely on asymptotic assumptions, thereby allowing for more accurate inferences when sample sizes are small. 12 Further analyses were conducted treating pre-biopsy platelet count as a binary rather than continuous variable with the purpose of determining a cut-off that could be applied to clinical practice.
Results
Baseline characteristics
Baseline characteristics of patients with and without bleeding complication
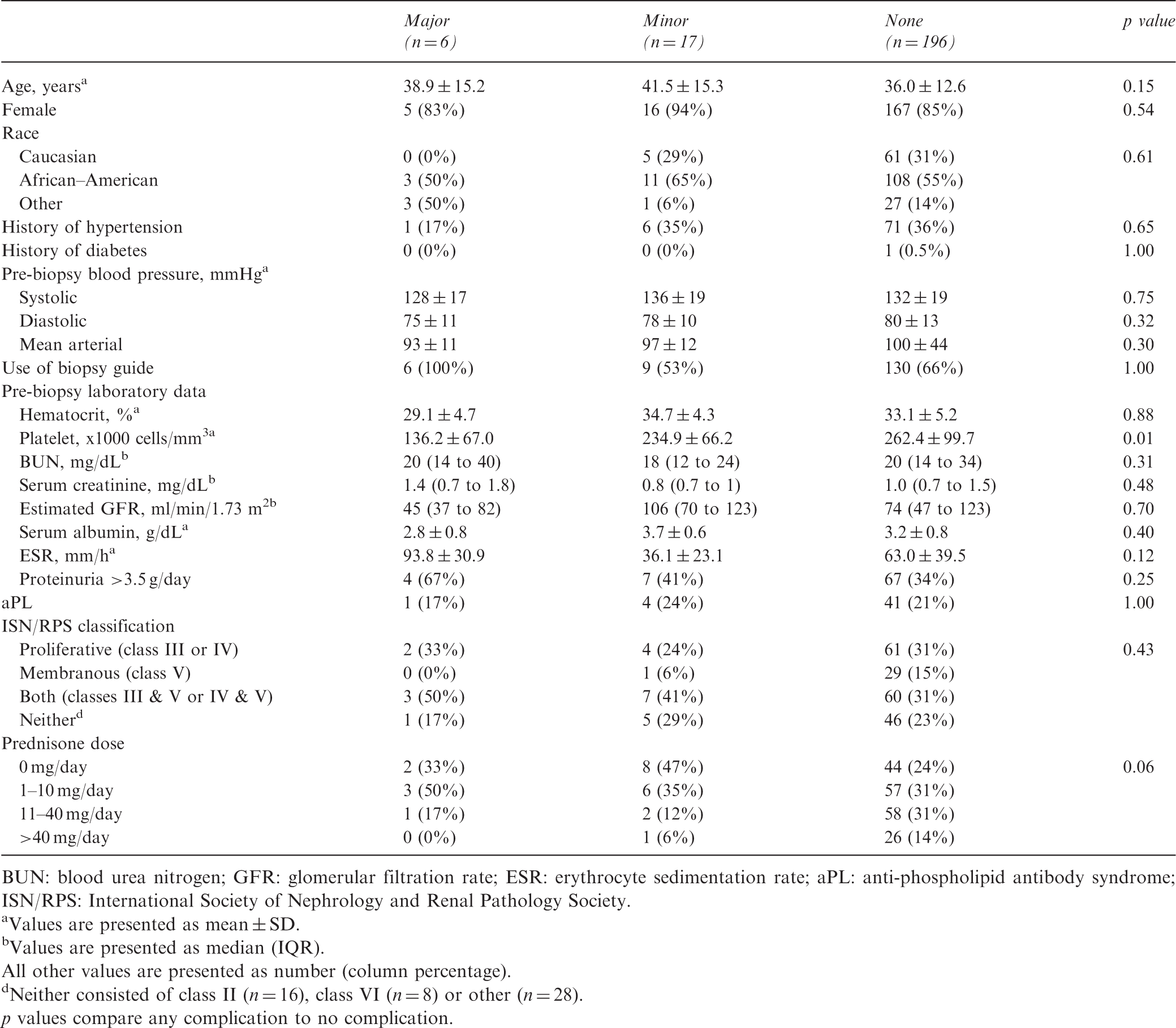
BUN: blood urea nitrogen; GFR: glomerular filtration rate; ESR: erythrocyte sedimentation rate; aPL: anti-phospholipid antibody syndrome; ISN/RPS: International Society of Nephrology and Renal Pathology Society.
Values are presented as mean ± SD.
Values are presented as median (IQR).
All other values are presented as number (column percentage).
Neither consisted of class II (n = 16), class VI (n = 8) or other (n = 28).
p values compare any complication to no complication.
Clinical outcome
Crude and adjusted odds ratios (ORs) for biopsy complication
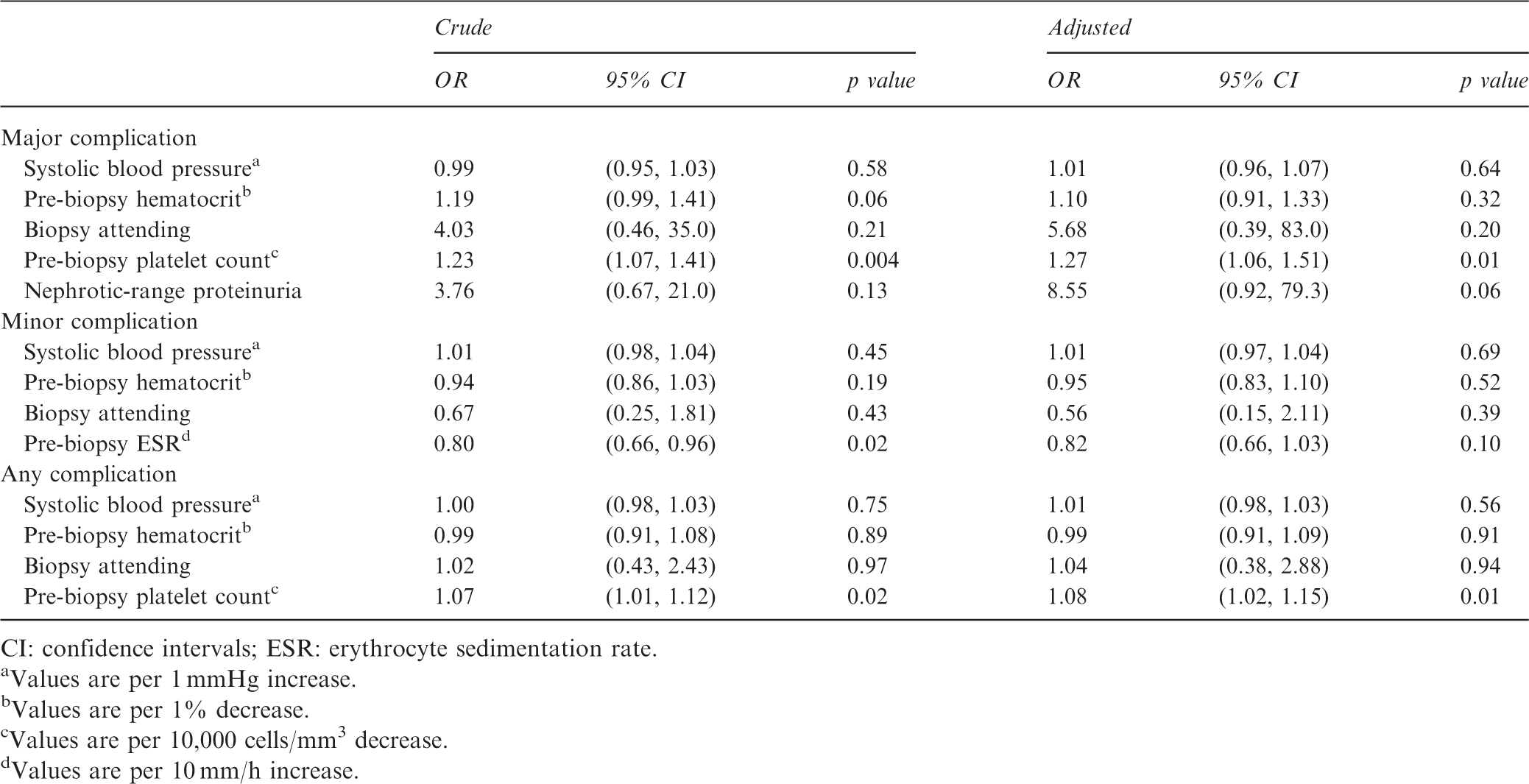
CI: confidence intervals; ESR: erythrocyte sedimentation rate.
Values are per 1 mmHg increase.
Values are per 1% decrease.
Values are per 10,000 cells/mm3 decrease.
Values are per 10 mm/h increase.
Description of individuals with biopsy-related major complications
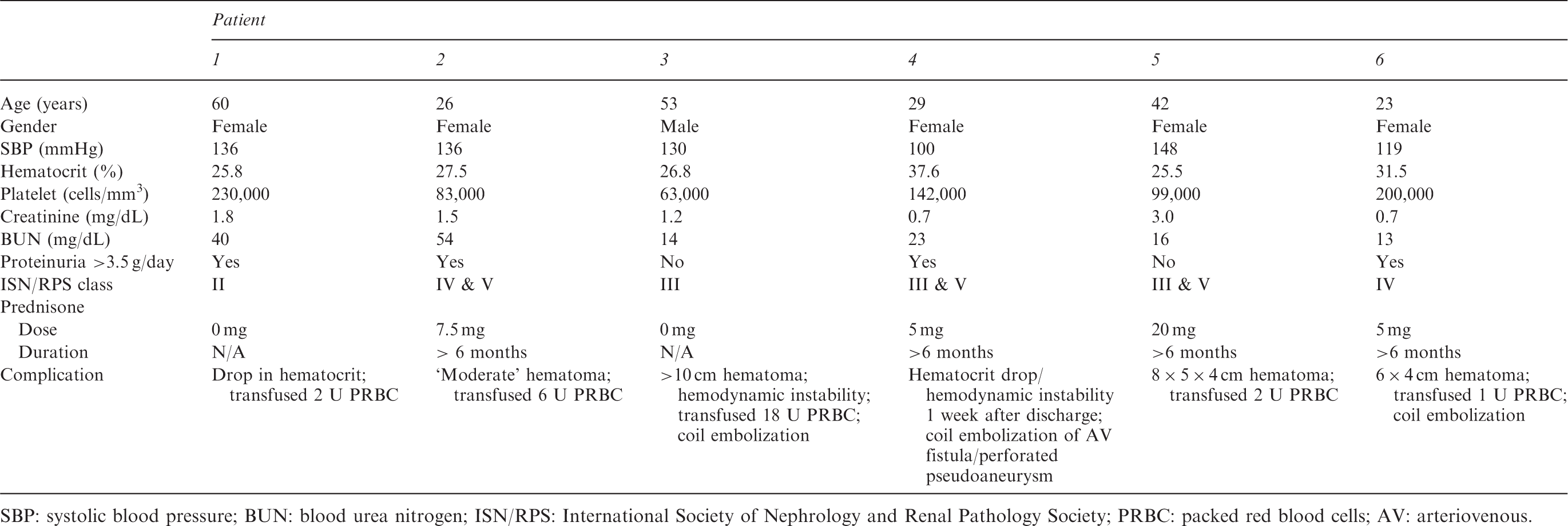
SBP: systolic blood pressure; BUN: blood urea nitrogen; ISN/RPS: International Society of Nephrology and Renal Pathology Society; PRBC: packed red blood cells; AV: arteriovenous.
In contrast to major complications, pre-biopsy platelet count was not associated with minor complication risk. Higher ESR, however, was associated with a decreased risk for minor complication (crude OR 0.80; 95% CI 0.66–0.96; p = 0.02), but this association did not reach statistical significance after adjustment for systolic blood pressure, pre-biopsy hematocrit and biopsy attending (adjusted OR 0.82; 95% CI 0.66–1.03; p = 0.10).
None of the remaining candidate predictors was associated with bleeding complications. Of note, lower eGFR and/or higher blood urea nitrogen level were not associated with greater risk for any, major or minor complication. This finding was surprising, as patients with decreased renal function leading to uremia are often considered as having dysfunctional platelets. Moreover, patients who were on prednisone, a medication known to impair wound healing, at the time of biopsy were not more likely to bleed compared to patients not taking prednisone. Finally, underlying ISN/RPS class of lupus nephritis appeared to have no impact on risk of bleeding. When using likelihood ratio testing, none of these variables made it into the final models for each of the three outcomes, thus providing further support that they were not predictive of post-biopsy bleeding.
Sensitivity analysis
Exact logistic regression provided similar findings as those obtained by ordinary logistic regression. When pre-biopsy platelet count was coded as a binary rather than continuous variable, the best platelet count cut-off for use in clinical practice was 150,000 cells/mm3. More specifically, patients with platelet counts < 150,000 cells/mm 3 had a 30-fold higher odds of having a major complication compared to patients with a platelet count ≥150,000 cells/mm3, although the 95% CI was wide (95% CI, 3.40–259.83; p = 0.002). Similarly, patients with platelet counts <150,000 count/mm3 were four times more likely to experience any bleeding complication compared to patients with higher platelet counts (95% CI, 1.16–12.45; p = 0.03).
Discussion
This study contributes to our understanding of the safety of percutaneous kidney biopsy in patients with SLE. Our data suggest that the incidence of major complications in this population is relatively low at 2.7%, although minor complications are not uncommon. Moreover, our analysis provides support that pre-biopsy platelet count is a key predictor of bleeding following kidney biopsy. To the best of our knowledge, this is the first study to estimate the incidence of bleeding complication following kidney biopsy in patients with SLE.
We observed that the overall odds for any complication increased by 8% for every 10,000 platelet count/mm 3 decrease and that pre-biopsy platelet count was particularly predictive of a major bleeding complication with a 27% increase in odds for every 10,000 platelet count/mm3 decrease. Moreover, individuals with platelet counts <150,000 cells/mm3 were 30 times more likely to develop biopsy-related major complications and four times more likely to have any biopsy-related bleeding complications. While most clinicians avoid invasive procedures at platelet counts <50,000–75,000 cells/mm3, our results show that the concern for bleeding should remain even at higher levels. In fact, three of the six patients who developed a major complication had a pre-biopsy platelet count >100,000 cells/mm3.
Thrombocytopenia is not uncommon in the SLE population. Studies have estimated that approximately 10–27% of patients with SLE have platelet counts of <100,000 cells/mm3.8,9 While many potential causes have been proposed, most cases of thrombocytopenia in patients with SLE are either immune-mediated or related to immunosuppressive medications used to treat lupus. 13 General recommendations are for symptomatic patients with a platelet count <50,000 cells/mm3 or asymptomatic patients with a platelet count <20,000 cells/mm3 to be initiated on glucocorticoid therapy. 14 Our findings suggest that those patients with SLE undergoing renal biopsy should have higher target platelet levels, especially in the peri-procedural period. We propose that the platelet count should be at least 100,000 cells/mm3 prior to renal biopsy in patients with SLE, but one could argue, based on current data, that a platelet count >150,000 cells/mm3 would be even more ideal. Response to treatment should be apparent within weeks; thus, a trial of steroids seems reasonable if delay in renal biopsy is possible. Our own practice at present is to transfuse platelets to >100,000 cells/mm 3 if urgent biopsy is needed.
The complication rates seen in this study are not considerably different from those that have previously been reported in non-lupus patients. In a general cohort of 471 patients who underwent ultrasound guided kidney biopsy in Italy, 34.1% experienced some form of bleeding complication (gross hematuria 0.4%, arteriovenous fistula 0.4%, hematoma 33.3%) with 1.2% experiencing major complications (blood transfusion, angiography or nephrectomy). Of note, all patients in that study underwent protocol imaging post-biopsy, perhaps accounting for the higher incidence of hematomas observed. Of the 157 patients who developed a hematoma, 90% were clinically silent, suggesting that post-biopsy hematomas are not uncommon and often go undetected. While there were no deaths, the one patient who did require a nephrectomy had SLE and class IV lupus nephritis. Female gender, younger age and a higher partial thromboplastin time were found to be associated with increased risk for bleeding. 7 In another study, Whittier et al. reported a biopsy complication rate of 13% (major 6.4%, minor 6.6%) and found that only a higher baseline serum creatinine was predictive of bleeding. Again, these results were among patients from the general population who required a kidney biopsy. 6 Finally, a recent study at our institution reported similar rates of bleeding complication among HIV-infected (overall 8.6%, major 3.3%, minor 5.4%) individuals compared to what we observed in this study. 15 The hematologic abnormalities often associated with SLE may partially explain the slight increase in risk of total complications that were observed in our patient population.
This study is not without limitations. First, the study population was derived from a tertiary care academic center with specialized care for SLE patients; therefore, our findings may not be generalizable to other institutions. For example, all biopsies in this study were performed by nephrologists, whereas other institutions may have the bulk of their renal biopsies conducted by radiologists. Moreover, institutions with real-time pathology technician assessment of sample adequacy may experience a lower incidence of bleeding complication, as the number of biopsy attempts per patient might be reduced. Second, the most recent blood pressure available in the patient’s medical record was used. In most cases this was from the most proximal clinic visit, which may have differed from the patient’s blood pressure at the time of biopsy. While such measurements were not standardized, they reflect usual clinical practice in which the decision to proceed with renal biopsy is usually made during a clinic visit. In addition, while all patients had a clinical diagnosis of SLE as determined by a rheumatologist, the retrospective nature of this study makes it difficult to confirm that each met the revised American College of Rheumatology criteria for SLE. We did show, however, that of the 219 patients who were biopsied, only 12.8% had no evidence of lupus nephritis on pathology. Another limitation of the study was the possibility of ascertainment bias, as not all patients underwent post-procedure imaging. Thus, some patients may have had small post-biopsy hematomas that were never detected because they did not have symptoms to warrant further evaluation. Finally, we had a small number of major complications. Exact logistic regression was used to account for this and yielded similar results.
In conclusion, our study shows that kidney biopsy is generally well tolerated in patients with SLE. Pre-biopsy platelet count, however, strongly predicts the risk for both major and any bleeding complication and patients with SLE referred for kidney biopsy should be counseled accordingly.
Footnotes
Funding
T.K.C. is supported by NIH-NIDDK grant 5T32DK007732. M.M.E. is supported by NIH-NIDDK grant 1K23DK081317.
Conflict of interest
None declared.