
Abstract
Psoriasis is an autoimmune inflammatory disease that has recently been treated with a novel treatment, ustekinumab, a human monoclonal antibody that targets the Th17 pathway. Discoid lupus is a subset of chronic cutaneous lupus erythematosus. Recent studies have suggested the Th17 pathway may be involved in cutaneous lupus. We present a case of a 41-year-old man with both severe psoriasis and hypertrophic discoid lupus treated with ustekinumab. After three doses of 45 mg subcutaneous injections at day 1, week 4, and week 16, his psoriasis plaques cleared and his hypertrophic discoid lupus plaques showed moderate improvement. Following a fourth dose of 90 mg his lupus plaques showed marked improvement. Ustekinumab may be a promising therapy for this and other forms of cutaneous lupus.
Background
Psoriasis is an immune-mediated disease of skin and joints characterized by thickened epidermal layers resulting from excessive keratinocyte cell proliferation. 1 The disease is orchestrated by proinflammatory CD4-positive helper T cells that produce interferon gamma and interleukin-17. 2 Interferon gamma produces TNF-alpha which has been targeted in the treatment of psoriasis. While TNF-alpha inhibitors have been a mainstay of treatment of psoriasis, there are cases of moderate to severe psoriasis that do not respond and TNF-alpha inhibitors have been associated with exacerbation of cutaneous lupus erythematosus. 3 Ustekinumab is a human monoclonal antibody that targets the p40 subunit of interleukin-12 and interleukin-23(IL-23). 4 Neutralization of these cytokines leads to rapid and sustained improvement in moderate–severe plaque psoriasis. 4
Discoid lupus erythematosus is a subset of chronic cutaneous lupus that is characterized by verrucous and hyperkeratotic plaques with indurated borders. Like psoriasis, CD4-positive helper T cells of the Th1 subset have been implicated in the pathophysiology of cutaneous lupus. However, unlike psoriasis, TNF-alpha inhibitors are not generally recommended as an effective treatment for cutaneous lupus and may cause or exacerbate the disease. 3 Recent studies have found Th17 cells to be involved in both systemic lupus erythematosus with cutaneous involvement as well as cutaneous lupus,5,6 A recent case report showed successful treatment of a case of subacute cutaneous lupus erythematosus with ustekinumab. 7 Coexistence of lupus erythematosus and psoriasis is rare, occuring in 0.69% of patients with psoriasis and 1.1% of patients with lupus erythematosus. However, when they occur concomitantly, discoid lupus can be the lupus subtype in as many as 80% of the cases.8,9
We present the case of a 41-year-old man with severe psoriasis and hypertrophic discoid lupus. He was originally treated with methotrexate, hydroxychloroquine, cyclosporine, and various topical steroids with a mild response of his psoriasis and no response of his discoid lupus. Subsequent treatment with ustekinumab completely cleared his psoriatic plaques and his discoid lupus eventually showed marked improvement.
Clinical case
A 41-year-old gentleman presented with a history of occasional joint pain, swollen fingers, and two different types of cutaneous lesions found on his bilateral arms, legs, face and scalp. Some of these lesions improved with sun exposure while some worsened. He had previously received diagnoses of both psoriasis and cutaneous lupus. Providers attempted multiple trials of methotrexate, cyclosporine, azathioprine, intralesional steroids, and UVB light therapy. His psoriasis plaques partially responded to the methotrexate and UVB light therapy. On physical exam, he had erythematous scaly plaques on his forearms, shins, and thighs, clinically consistent with psoriasis. He also had hyperkeratotic hypopigmented plaques on his back, legs, elbows and lateral forearms. Skin biopsies from these lesions indicated an interface dermatitis with basement membrane thickening and dermal mucin deposition. He was given the diagnoses of severe psoriasis and hypertrophic discoid lupus. Labs at his initial presentation showed an ANA titer of 1:1280 with a speckled pattern. He had no other clinical features of systemic lupus.
He was initially started on methotrexate 20 mg weekly and clobetasol 0.05% ointment three times weekly. Over the course of four years his psoriasis waxed and waned on 20 mg of methotrexate weekly and varying amounts of topical steroids. The cutaneous lupus lesions had minimal to no response. The methotrexate was discontinued once he began experiencing gastrointestinal side effects. He was started on cyclosporine 350 mg daily as well as hydroxychloroquine 200 mg daily. His discoid lupus did not respond to this treatment but he did have a mild decrease in the severity of his psoriatic plaques. Over the next four months with a taper of his cyclosporine his psoriasis and discoid lupus plaques acutely worsened.
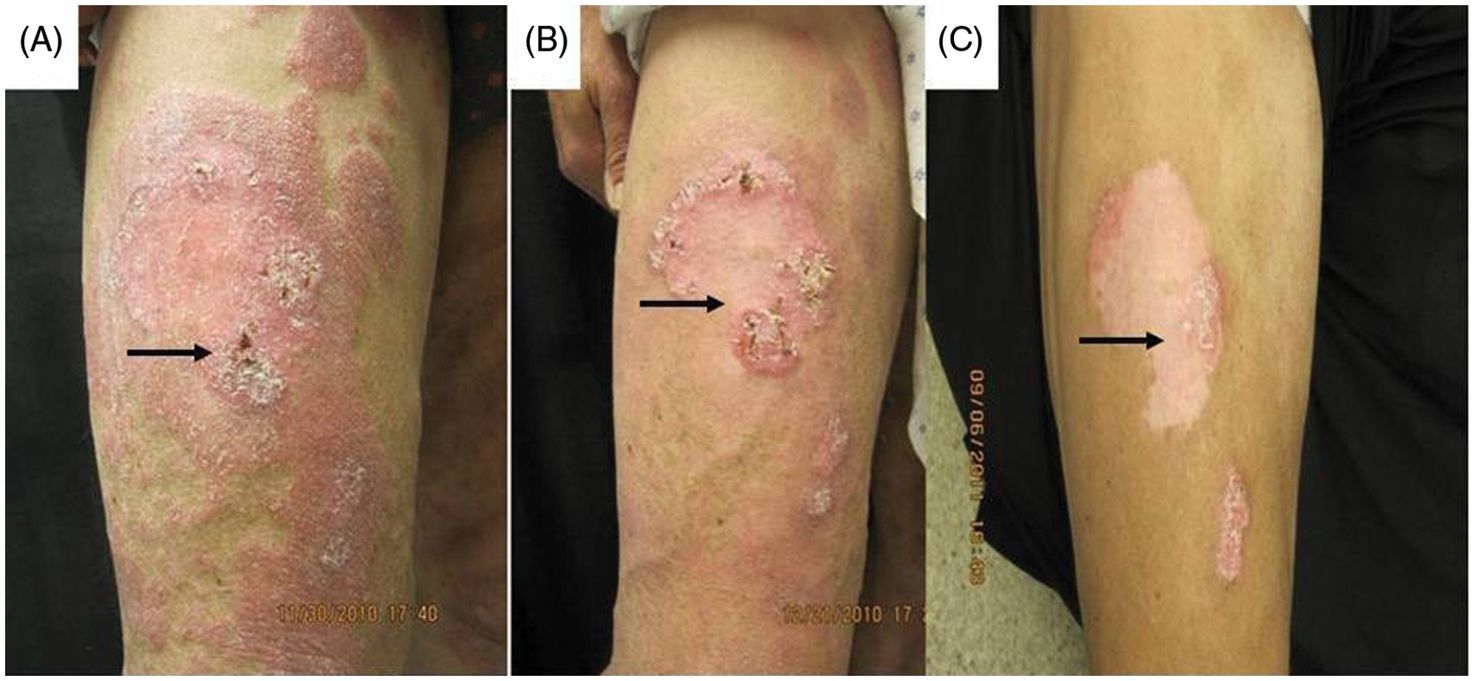
Approximately six years after his initial presentation, ustekinumab 45 mg injections were administered initially, four weeks later, then subsequently every twelve weeks (Figures 1a, 2a). The patient weighed 70.5 kg. Hydroxychloroquine was discontinued. Cyclosporine was tapered off over three months. Dramatic improvement in his psoriatic plaques was noticed within two months and his discoid lupus lesions became slightly less indurated with fewer scales (Figures 1b, 2b). His psoriasis remained clear at his follow-up appointments over the next five months and his discoid lupus plaques began to show modest improvement. He was then given a 90 mg injection of ustekinumab in an attempt to clear his residual cutaneous lupus activity. When he presented six weeks later his discoid lupus plaques showed marked improvement with less induration and keratosis and moderate regression of the margins of his lupus plaques (Figures 1c, 2c). He did not experience any clinical or laboratory evidence of systemic lupus during treatment.
Response to ustekinumab in left arm. At initiation of treatment (a), 8 weeks later (b), 6 weeks after 90 mg injection (c). Arrows indicate discoid lupus plaques. Response to ustekinumab in right thigh. At initiation of treatment (a), 4weeks later (b), 6 weeks after 90 mg injection (c). Arrows indicate discoid lupus plaques.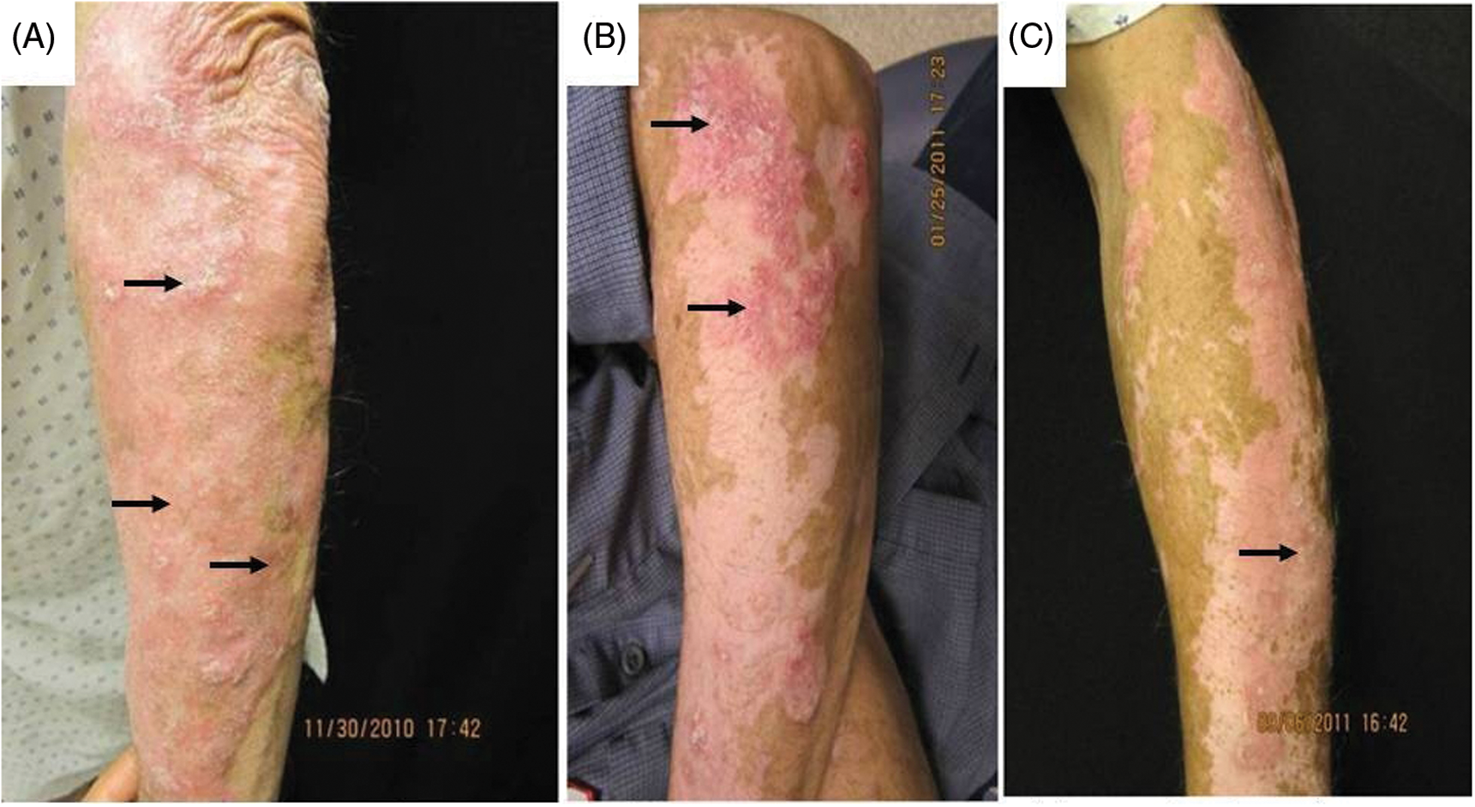
Discussion
In recent years the Th17 pathway has been shown to be involved in many autoimmune diseases, including psoriasis. 10 It is powered by a unique set of interleukins including IL-23. IL-23 expression has been shown to be higher in the epidermis of psoriatic skin and IL-23 messenger RNA is elevated in lesional skin samples of patients with psoriasis. 11 Produced from activated macrophages and dendritic cells, it stimulates the proliferation of Th17 helper T cells. Th17 cytokines stimulate keratinocyte proliferation 12 allowing for epidermal cell expansion in psoriasis. Ustekinumab allows for rapid neutralization of proinflammatory cytokines 4 and has become a promising treatment for moderate to severe psoriasis.
Recent studies have investigated the presence of Th17 in many autoimmune diseases including subacute cutaneous lupus erythematosus and SLE.5,6 Given the potential role of Th17 in cutaneous lupus, there has been speculation as to the potential role of ustekinumab as a treatment of cutaneous lupus erythematosus. To date, there has been one published case of cutaneous lupus that responded to ustekinumab. 7
Hypertrophic discoid lupus erythematosus is a distinct subset of lupus erythematosus originally described by Behcet in 1940. 13 Our knowledge regarding the treatment of hypertrophic discoid lupus is based mainly on case studies and experience; no randomized control trials exist that define the best treatment modalities. Common therapies include sun protection, topical and intralesional corticosteroids, systemic antimalarials, and other immunosuppressive agents. Our case illustrates that hypertrophic discoid lupus is often difficult to manage and particularly resistant to treatment. 14 To our knowledge, our report presents the first reported case of ustekinumab used concomitantly on a patient with both psoriasis and cutaneous lupus erythematosus and represents the second reported case of cutaneous lupus responding to ustekinumab. Like TNF-alpha inhibitors, there was considerable concern for the possibility of ustekinumab triggering symptoms of systemic lupus, but this was not observed. It is notable, however, that the 45 mg injections of ustekinumab were sufficient to show complete clearance of the patient’s psoriatic skin lesions while the hypertrophic discoid lupus lesions required a 90 mg injection before they showed notable improvement.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.