
Abstract
Antiprothrombin (aPT) antibodies may be detected by an enzyme-linked immunosorbent assay (ELISA) using a purified antigen or a phosphatidylserine/prothrombin complex (aPS/PT). IgG/IgM antibodies directed against aPS/PT were assessed in 158 patients with primary antiphospholipid syndrome (PAPS). They were detected in 80/158 (50.6%) PAPS patients; IgG alone was positive in 12 (7.6%), IgM alone in 36 (22.8%), and both IgG and IgM isotypes in 32 (20.2%) PAPS patients. IgG and IgM aPS/PT were significantly associated with both vascular thrombosis and pregnancy morbidity. IgG aPS/PT was significantly associated with venous thrombosis (p = 0.023), whilst IgG and IgM aPS/PT were associated with arterial thrombosis (p < 0.001 and p < 0.001, respectively). Logistic regression analysis showed that IgM and IgG aPS/PT were independent risk factors for thrombosis (odds ratio (OR) 3.5 [95% confidence interval (CI) 1.6–7.9] and OR 4.1 [95% CI 1.4–11.7], respectively) and IgM aPS/PT was an independent risk factor for arterial thrombosis (OR 2.7 [95% CI 1.1–6.7]). In conclusion, these findings indicate that aPS/PT are clinically relevant in PAPS.
Keywords
Introduction
Antiprothrombin (aPT) antibodies may be detected by an enzyme-linked immunosorbent assay (ELISA) coating a purified antigen onto irradiated plates 1 or by using phosphatidylserine/prothrombin complex (aPS/PT) as antigen. 2 Several studies investigating aPS/PT have focused mainly on patients with systemic lupus erythematosus (SLE) and/or secondary antiphospholipid syndrome (APS). 2 – 4
In this study, IgG/IgM antibodies directed against PS/PT were assessed in a large cohort of patients with primary APS (PAPS).
Patients and methods
Plasma and serum samples were collected from 158 PAPS patients attending the Rheumatology Unit of Padua University. All of the subjects fulfilled the international consensus statement classification criteria for APS. 5 Fifty-six of these (35.4%) had a history of pregnancy morbidity alone including fetal loss, premature birth and early miscarriages (pregnancy morbidity group), and 102 (64.6%) had a history of previous thrombosis with (n = 19) or without (n = 83) pregnancy morbidity (thrombosis group). Fifty-one (50 %) had arterial thrombosis, 27 (26.5%) venous thrombosis and 24 (23.5%) both. One hundred healthy blood donors, age and sex matched with the study population, and 114 patients with autoimmune diseases were included as the control group.
IgG/IgM aPS/PT were detected using commercial ELISA kits provided by INOVA Diagnostics Inc (San Diego, California, USA). In accordance with the manufacturer’s instructions, the IgG/IgM aPS/PT cut-off values were > 30 U/mL for both isotypes. However, our cut-off was arbitrarily set at ≥40 U/mL to increase the specificity of the assay.
IgG/IgM anticardiolipin (aCL) and IgG/IgM antiβ2glycoprotein I (antiβ2GPI) antibodies were measured using an in-house ELISA, as described elsewhere.6,7 Lupus anticoagulant (LA) was detected according to internationally recognized recommendations. 8
Statistical analysis was performed using Pearson’s Chi-square, Fisher’s and Mann-Whitney tests. The multivariate analysis was performed using binary logistic regression.
Results
Prevalence of IgG/IgM aPS/PT and conventional aPL in PAPS patients
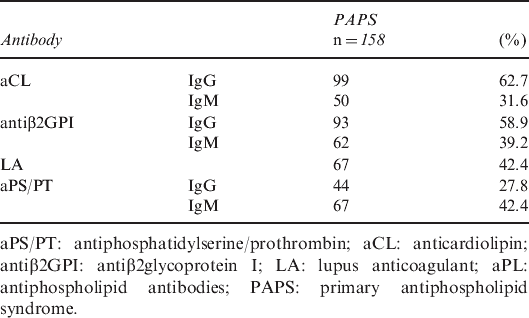
aPS/PT: antiphosphatidylserine/prothrombin; aCL: anticardiolipin; antiβ2GPI: antiβ2glycoprotein I; LA: lupus anticoagulant; aPL: antiphospholipid antibodies; PAPS: primary antiphospholipid syndrome.
The relationship of IgG/IgM aPS/PT antibodies with clinical features of PAPS

aPS/PT: antiphosphatidylserine/prothrombin; PAPS: primary antiphospholipid syndrome; CI: confidence interval; *Male patients have been excluded in the statistical comparison with pregnancy morbidity.
The prevalence of IgG and IgM aPS/PT in the different subsets of PAPS are reported in Table 3 and Figure 1.
The prevalence of IgG and IgM aPS/PT was significantly higher in the thrombosis/pregnancy morbidity group than in the thrombosis group (p < 0.001 for both isotypes) and higher in the thrombosis group than in the group with pregnancy morbidity (p < 0.001 for both isotypes). aPS/PT: antiphosphatidylserine/prothrombin. Comparison of IgG/IgM aPS/PT prevalence in the different clinical subsets of PAPS aPS/PT: antiphosphatidylserine/prothrombin; PAPS: primary antiphospholipid syndrome; CI: confidence interval.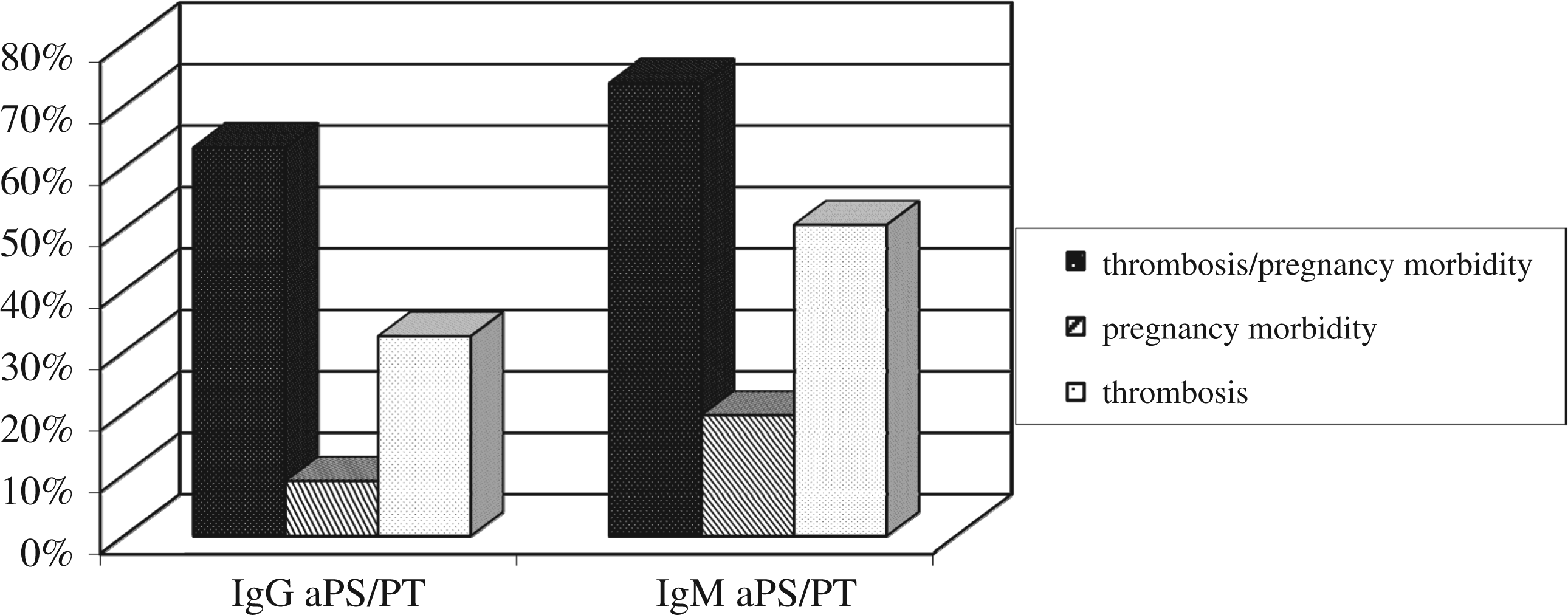

The mean titres of IgG and IgM aPS/PT were significantly higher in the thrombosis group than in the group with pregnancy morbidity (62.1 U/mL vs 13.2 U/mL, p < 0.001 and 78.2 U/mL vs 27.8 U/mL, p < 0.001, respectively). When all the patients with arterial (n = 75) and venous (n = 51) thrombosis were analysed separately, IgG aPS/PT antibodies were found to be significantly associated with venous thrombosis (p = 0.023), while IgG and IgM aPS/PT antibodies were significantly associated with arterial thrombosis (p < 0.001 for both).
Logistic regression analysis showed that IgM and IgG aPS/PT were independent risk factors for the presence of thrombosis (OR 3.5 [95% CI 1.6–7.9] and OR 4.1 [95% CI 1.4–11.7], respectively). IgM aPS/PT was an independent risk factor for arterial thrombosis (OR 2.7 [95% CI 1.1–6.7]). Moreover, IgG/IgM aPS/PT were independent risk factors for the presence of LA (OR 6.0 [95% CI 2.7–13.4] and OR 6.3 [95% CI 2.4–16.7], respectively).
Discussion
In this study we assessed IgG/IgM aPS/PT in a large, homogenous cohort of PAPS patients. Taking into account the logistic regression results, high titres of IgG/IgM aPS/PT are independent risk factors for the presence of LA and for thrombosis. Moreover, high titres of IgM aPS/PT antibodies could be considered a marker for arterial thrombosis in PAPS patients.
In our recent paper, 9 aPT directed to a purified antigen did not show a significant prevalence in thrombotic versus obstetric PAPS patients, thus, we could affirm that aPS/PT antibodies have a higher clinical relevance when their ability to distinguish thrombosis from obstetric morbidity is evaluated.
Further laboratory and clinical studies are certainly warranted to better define the clinical utility of antiprothrombin antibodies.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.