
Abstract
Infections are an important cause of morbidity and mortality in juvenile systemic lupus erythematosus (JSLE). Among them, invasive aspergillosis (IA), which is usually related to immunosuppressed patients, has been rarely reported in JSLE. From 1983 to 2011, 5604 patients were followed at our institution and 283 (5%) met the American College of Rheumatology (ACR) classification criteria for SLE. Six (2.1%) of our JSLE patients had IA. One of them was previously reported and five will be described herein. Four of them were female. The median age at JSLE diagnosis was 12 years (8–16) and the median interval between diagnosis of JSLE and IA was 6 months (1–38). All had pulmonary involvement and three of them had systemic involvement. The median Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) was 19 (7–22). Diagnosis of IA was performed by isolation of Aspergillus spp., two in bronchoalveolar lavage culture and by way of autopsy in the others. All of them were treated with corticosteroids and/or immunosuppressive drugs at IA diagnosis (azathioprine and/or intravenous cyclophosphamide). They all required treatment in the pediatric intensive care unit with mechanical ventilation and antifungal therapy (fluconazole, amphotericin B, itraconazole and/or voriconazole); nonetheless, none of them survived. In conclusion, this was the first report that evaluated the prevalence of IA in a large population of JSLE patients from a tertiary pediatric hospital, and clearly showed the severity of the outcome, especially in patients with active disease and treated with immunosuppressive agents. This study reinforces the importance of early diagnosis and treatment with certain antifungals, especially in critically ill patients.
Introduction
Infections are an important cause of morbidity and mortality in juvenile systemic lupus erythematosus (JSLE) patients.1,2 The majority of infections are caused by virus and bacteria, and less frequently by opportunistic agents such as fungi. 2
Invasive aspergillosis (IA) is a fungal infection caused by Aspergillus spp., usually related to primary immunodeficiencies, transplantation or to the use of immunosuppressive drugs. 3 It affects mainly the pulmonary tract, but can involve any organ or system. 4 Association between IA and SLE was seldom described in adults 4 – 7 and to our knowledge only two cases were reported in JSLE,1,8 including one from our pediatric rheumatology group. 1
Therefore, from January 1983 to June 2011, 5604 patients were followed at the Pediatric Rheumatology Unit from Instituto da Criança da Faculdade de Medicina da Universidade de São Paulo and 283 (5%) of them met the American College of Rheumatology (ACR) 9 classification criteria for SLE. Six (2.1%) of our JSLE patients had IA, and they were the only cases from the total population (n = 5604; 0.1%) followed at our Pediatric Rheumatology Unit with this invasive fungal disease. One of them was previously reported 1 and five will be described herein. This study was approved by the Local Ethics Committee of our University Hospital.
Demographic data, clinical features, laboratory findings, disease activity/damage, treatment regimens and outcome in juvenile systemic lupus erythematosus (JSLE) patients at invasive aspergillosis (IA) diagnosis
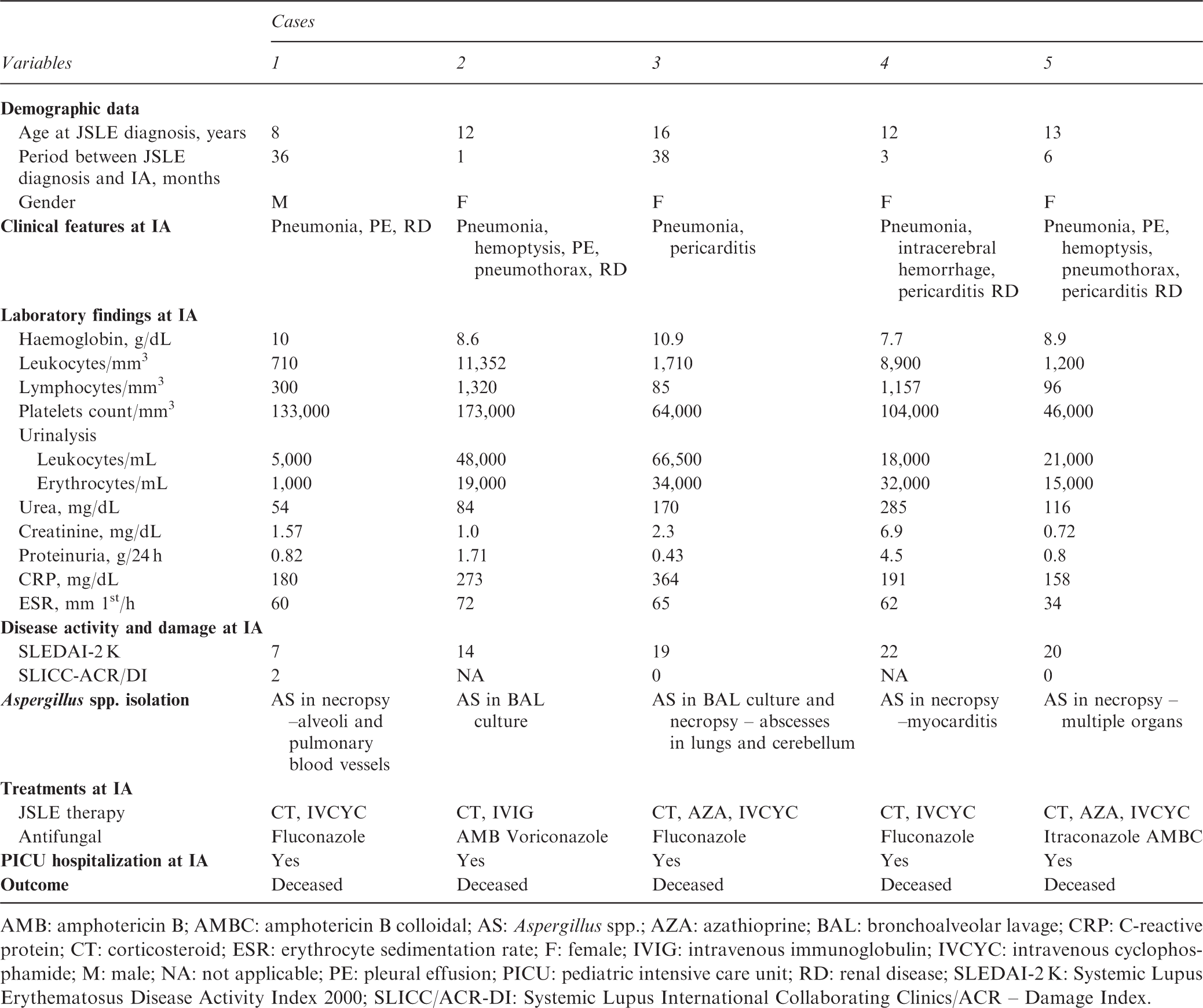
AMB: amphotericin B; AMBC: amphotericin B colloidal; AS: Aspergillus spp.; AZA: azathioprine; BAL: bronchoalveolar lavage; CRP: C-reactive protein; CT: corticosteroid; ESR: erythrocyte sedimentation rate; F: female; IVIG: intravenous immunoglobulin; IVCYC: intravenous cyclophosphamide; M: male; NA: not applicable; PE: pleural effusion; PICU: pediatric intensive care unit; RD: renal disease; SLEDAI-2 K: Systemic Lupus Erythematosus Disease Activity Index 2000; SLICC/ACR-DI: Systemic Lupus International Collaborating Clinics/ACR – Damage Index.
Case 1
An eight-year-old boy was admitted to our University Hospital with a one-year history of fever and recurrent tender erythematous nodules due to lupus panniculitis. The skin biopsy from the upper back region showed septal and lobular panniculitis, with lymphocytes in fat lobules, hyaline fat necrosis and without vasculitis. Direct immunofluorescence study of lesional skin was negative to IgG, IgM, IgA and C3. He was treated with prednisone 2 mg/kg/day, chloroquine diphosphate 5 mg/kg/day, cyclosporine 3 mg/kg/day and sunscreen protection, with improvement of clinical manifestations. At 11 years old, he had severe generalized skin vasculitis (diffuse tender erythematous nodules and peripheral gangrene in fingers) and pericarditis. Laboratory tests showed: white blood cell count 1900/mm3 (54% neutrophils, 39% lymphocytes, 6% monocytes and 1% eosinophils), platelets 108,000/mm3, proteinuria 0.7 g/24 h, antinuclear antibodies (ANA) 1:160 (fine speckled pattern), anti-Ro 1:40 IU/mL and the diagnosis of JSLE was confirmed according to the ACR criteria. 9 The Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) 10 score was 15. He was treated with three pulses of intravenous methylprednisolone (30 mg/kg/day) and monthly intravenous cyclophosphamide – IVCYC (750 mg/m2/dose). Four months later, he developed fever, cough, tachypnea, tachycardia and diffuse vasculitis. At that time, he was being treated with prednisone (1 mg/kg/day) and IVCYC (750 mg/m2/dose). Echocardiography showed pulmonary hypertension and left ventricular hypertrophy with diastolic dysfunction. Chest computed tomography found an infiltrate in the top of the right lung and bilateral pleural effusion, and vancomycin and cefepime were initiated. After six days of hospitalization in the pediatric intensive care unit (PICU), he had abdominal pain in conjunction with fever, respiratory insufficiency and oliguria. Laboratory findings at IA diagnosis are shown in Table 1. Chest radiography revealed infiltration in both lungs and antimicrobial agents were changed to meropenem, linezolid and fluconazole. After two days, he presented severe respiratory insufficiency due to pulmonary hemorrhage and died. The necropsy revealed numerous hyphae of Aspergillus spp. permeating both alveoli and pulmonary blood vessels.
Case 2
A 12-year-old girl was hospitalized in our University Hospital with a three-month history of recurrent fever associated with malaise, cutaneous vasculitis (tender nodules in the fingers), malar rash, photosensitivity, arthritis, myositis and pericarditis. Laboratory tests showed: hemoglobin 10 g/L, hematocrit 29.6%, white blood cell count 6100/mm3 (69% neutrophils, 24% lymphocytes, 6% monocytes and 1% eosinophils), platelets 101,000/mm3, urea 76 mg/dL (normal 10–42), creatinine 2.09 mg/dL (normal 0.6–0.9), C3 0.41 mg/dL (normal 0.5–1.8), C4 0.27 mg/dL (normal 0.1–0.4), urinalysis (14,400 leukocytes/mL and 15,000 erythrocytes/mL), erythrocyte sedimentation rate (ESR) 24 mm/1st hour, C-reactive protein (CRP) 243 mg/dL (normal < 5) and echocardiogram showed pericardial effusion. Immunological tests showed ANA 1:320 (fine speckled pattern), positive anti-double-stranded DNA (anti-dsDNA) and IgG anticardiolipin antibodies (15 GPL). The diagnosis of JSLE was confirmed according to the ACR criteria, 9 her SLEDAI-2K 10 was 26 and pulse therapy with methylprednisolone 1 g/day for three days was started. After three days of hospitalization, she presented septic shock and underwent invasive mechanical ventilation, dialysis and antibiotic treatment (ceftriaxone and vancomycin). On the fourth day in the PICU, ceftriaxone was changed for meropenem, associated with gancyclovir and amphotericin B, and she also received 2 g/kg of intravenous immunoglobulin (IVIG). Twenty days later, she presented fever, cough, hemoptysis and respiratory failure. Chest radiograph showed pulmonary infiltrate, pleural effusion and pneumothorax in the right side. The chest computed tomography scan revealed a pulmonary mass in the bottom of the right lung and Aspergillus spp. was isolated in bronchoalveolar lavage (BAL) culture. Voriconazole was promptly administered. However, on the thirteenth day despite this new antifungal therapy, she died of septic shock.
Case 3
A 16-year-old girl was diagnosed with JSLE 9 based on arthritis, serositis (pleuritis and pericarditis), proteinuria 1 g/24 h, ANA 1:160 (dense fine speckled pattern) and positive anti-dsDNA. Other laboratory tests revealed hemoglobin 8.9 g/L, hematocrit 28%, white blood cell count 3600/mm3 (66% neutrophils, 27% lymphocytes, 1% eosinophils and 6% monocytes), platelets 183,000/mm3, abnormal urinalysis (13,000 leukocytes/mL, 28,000 erythrocytes/mL), urea 40 mg/dL, creatinine 0.6 mg/dL, C3 0.3 mg/dL and C4 0.05 mg/dL. ESR was 60 mm/1st hour and CRP 7.8 mg/dL. The SLEDAI-2K 10 was 24 and prednisone 2 mg/kg/day was started. Over the following two years, she had recurrent pericarditis and frequent migraine, which was treated with analgesic and opioids, besides the introduction of azathioprine 2 mg/kg/day and prednisone 1 mg/kg/day. At 19 years old, she had cutaneous vasculitis and migraine refractory to opioids, when IVCYC (500 mg/m2/month) was administered. Two months later, she was hospitalized due to persistent migraine (nonresponsive to narcotic analgesia), fever, pericarditis and myocarditis, confirmed by echocardiogram. At that time, her medications were prednisone 1 mg/kg/day and azathioprine 2 mg/kg/day. She also received dobutamine, antibiotics (oxacillin, cefepime and amikacin) and methylprednisolone 1 g/day for three days. However, she developed cardiogenic and septic shock, requiring epinephrine, mechanical ventilation and pericardial drainage. Main laboratory tests are shown in Table 1. The pericardial effusion culture isolated Staphylococcus aureus. One week later, she developed pneumonia and fluconazole was also empirically introduced. Seven days later, she had renal insufficiency and died. The culture of BAL isolated Aspergillus spp. only after her death. Autopsy showed fungal abscesses in the lungs and cerebellum due to Aspergillus spp.
Case 4
At the age of 12 years and two months, a female teenager presented diffuse cutaneous bullous lesions, pericarditis, anasarca, arterial hypertension and renal failure within a period of six months. Laboratory findings showed: hemoglobin 9.3 g/L, hematocrit 26%, white blood cell count 6800/mm3 (95% neutrophils, 4% lymphocytes and 1% monocytes), platelets 134,000/mm3, proteinuria (4 g/24 h), abnormal urinalysis (13,000 leukocytes/mL, 28,000 erythrocytes/mL), urea 125 mg/dL, creatinine 7.6 mg/dL, C3 0.5 mg/dL and C4 0.2 mg/dL, ESR 63 mm/1st hour, CRP 5.9 mg/dL and positive ANA 1:320 (speckled pattern), anti-Sm, anti-RNP and anti-Ro antibodies. At 12 years and eight months, JSLE 9 was diagnosed and her SLEDAI-2K 10 was 14. Treatment during hospitalization consisted of methylprednisolone pulse therapy for three days 1 g/day and IVCYC (750–1000 mg/m2/month), requiring peritoneal dialysis and then hemodialysis. At 12 years old and 10 months, she had severe headache, left hemiparesis and pneumonia. Laboratory findings are shown in Table 1. The brain computed tomography scan revealed an 8 cm parenchymal hematoma in the right cerebral hemisphere. Decompressive craniotomy, methylprednisolone pulse therapy for five consecutive days 1 g/day, antibiotics (teicoplanin and ceftazidime) and fluconazol were administered. However, she went into a coma and died after 15 days. Necropsy revealed myocarditis by Aspergillus spp. in the posterior wall of the left ventricle, parenchymal hematoma in the right cerebral hemisphere and pneumonia without fungi isolation.
Case 5
A 13-year-old girl had a two-month history of alopecia, malar rash, diffuse cutaneous vasculitis (palpable purpura and necrotic lesions), generalized seizures, macroscopic hematuria, Raynaud phenomenon and arthritis. Laboratory tests showed: hemoglobin 9.8 g/L, hematocrit 33%, white blood cell count 3600/mm3 (81% neutrophils, 18% lymphocytes and 1% monocytes), platelets 265,000/mm3, proteinuria (0.82 g/24 h), abnormal urinalysis (25,000 leukocytes/mL, 400,000 erythrocytes/mL and granular casts), urea 58 mg/dL, creatinine 0.8 mg/dL, C3 0.67 mg/dL, C4 0.20 mg/dL, ESR 50 mm/1st hour, CRP 81.1 mg/dL and positive ANA 1:320 (homogeneous pattern), anti-dsDNA and anti-P antibodies. Renal biopsy showed mesangial lupus nephritis. The diagnosis of JSLE was confirmed according to the ACR criteria 9 and her SLEDAI-2K 10 was 24. Prednisone 2 mg/kg/day, IVCYC (500 mg/m2/month) and subsequently azathioprine 2 mg/kg/day were administered. Six months after JSLE diagnosis, she was hospitalized with a two-week history of anasarca associated with malar rash, macroscopic hematuria, cough, progressive dyspnea and two days of fever. At that time, she was receiving prednisone 0.5 mg/kg/day, azathioprine 2 mg/kg/day and IVCYC (500 mg/m2/month), and ceftriaxone and furosemide were initiated, evolving with partial resolution of anasarca. On the sixth day of hospitalization, she still had cough and purulent sputum, and one week later she developed dyspnea and pain in the right hemithorax. Anasarca was still unresolved and chest x-ray showed an infiltrate in the bottom of the right lung and ipsilateral pleural effusion. Antibiotic treatment was changed to cefepime and vancomycin, and itraconazole was started. However, five days later she developed hemoptysis and respiratory failure, being intubated and transferred to the PICU. The main laboratory findings are described in Table 1. Thoracic radiography revealed a diffuse infiltrate involving both the entire right side and most of the left side of the chest, and echocardiography showed a pericardial effusion. Itraconazole was changed to colloidal amphotericin B. However, thirteen days later she presented with respiratory failure and massive hemoptysis through the endotracheal tube. A new chest radiograph revealed bilateral pneumothorax, which was promptly drained, and a cystic image in the right lung base. The thoracic computed tomography scan found a cavity in the right lung. Blood culture was performed and was negative for microorganisms. The following week she had another pulmonary hemorrhage and died. Autopsy showed clusters of septate hyphae, spores and conidia of Aspergillus spp. in necrotic areas of cavities in the lungs, as well as necrosis and fungal proliferation in the brain, cerebellum, heart, esophagus, stomach, liver, pancreas, small intestine, colon, kidneys and dermis.
Discussion
This was the first report that evaluated the prevalence of IA in a large population of JSLE patients from a tertiary Pediatric Hospital, and clearly showed a very severe outcome, especially in patients with active disease treated with immunosuppressive agents. To our knowledge, only two cases1,8 of this association have been reported so far, including one previously published by our Pediatric Rheumatology Service. 1
Aspergillus spp. is a ubiquitous fungus acquired by airborne spores inhalation. There are three major forms of aspergillosis: allergic, chronic (saprophytic) and IA. 12 The allergic subtype typically affects asthma patients and the saprophytic subtype generally constitutes milder forms of the disease. Importantly, IA has emerged as a cause of life-threatening infection in immunocompromised patients with human immunodeficiency virus (HIV), prolonged neutropenia, primary immunodeficiencies, solid organ or hematopoietic stem cell transplantation and treated with immunosuppressive agents.3,12 Of note, this severe infection was also reported in pediatric and adult lupus patients,1,4– 8 generally after disease diagnosis, as observed herein.
The respiratory tract is the most common site of IA,1,4,5,7,8 and most patients present fever, dyspnea, cough and hemoptysis, as observed in our patients. In patients with pulmonary complications, such as pulmonary hemorrhage and unexplained or unresolved infiltrations after broad-spectrum antibiotic therapy, a high degree of suspicion is necessary for prompt recognition of pulmonary aspergillosis. 13 Other organs and systems may be affected, such as kidney, heart and brain. 4 Indeed, three of our cases had Aspergillus spp. in extra-pulmonary sites. In one of them, this infectious agent was demonstrated solely in the myocardial tissue, which was uncommonly described in previous reports. 12
IA diagnosis is challenging due to non-specific signs and symptoms, since multisystemic involvement of this opportunistic infection may mimic JSLE manifestations,5,7 as evidenced in this report. Indeed, in our patients this severe infection was associated with disease activity, which probably contributed to the delay of IA diagnosis.
Definitions of invasive fungal disease have been recently revised and three levels of probability in immunocompromised patients were proposed: ‘proven’, ‘probable’ and ‘possible’. Proven IA demands isolation of Aspergillus spp. in tissue. Probable IA requires isolation of Aspergillus spp. in direct test (culture, cytology or microscopy) or indirect test (detection of antigen or cell-wall component). Possible IA needs a host factor (for example, neutropenia and immunosuppressive agents use) and a clinical criterion (for example, lower respiratory tract fungal disease) without mycological criteria. 14 In our JSLE population, proven IA was observed in four cases and probable IA in one case.
CRP is a classical marker of inflammation and values over 50 mg/dL are closely related to infections in SLE patients. 15 Interestingly, in Case 2 there were high levels of this early phase reactant both at lupus diagnosis and at IA diagnosis, suggesting that perhaps she had this infection at first evaluation and it was triggered by the immunosuppressive treatment. Chest computed tomography may help in the suspicion of a possible invasive fungal disease, especially in the presence of pulmonary mass or cavity, 14 as observed in two of our cases. The detection of galactomannan, a constituent of the cell wall of Aspergillus spp., in serum or in BAL assay, has been described as a valuable tool to diagnose IA.3,12,16 This test may be useful in critically ill patients, although there are several confounding factors.3,16 To our knowledge this test has not yet been performed in adult and pediatric lupus patients, and requires further studies in intensive care units. However, this tool might be taken into account in severe immunocompromised lupus patients. 16
The most important risk factors associated with invasive fungal disease in the lupus population are related to the disease itself (activity, lymphopenia, leucopenia and neutropenia) and treatments (corticosteroids and immunosuppressive drugs).1,2 Leucopenia, especially lymphopenia, and drugs were the main risk factors for this opportunistic infection in our JSLE patients.
Treatment of infected lupus patients with antifungal therapy should be promptly initiated, especially amphotericin B,1,4,5,8 itraconazole, 8 voriconazole 17 and equinocandin. 18 Voriconazole is the current treatment of choice for IA; 15 however, liposomal amphotericin B should be indicated in cases of drug intolerance or refractory disease.3,12 Equinocandin is also an alternative treatment. 18 One limitation of the present study was the retrospective design. According to the guidelines for aspergillosis by the Infectious Diseases Society of America, fluconazole is not the antifungal therapy for the treatment of IA. 12 We used this drug in the nineties as an empiric antifungal treatment but voriconazol has been the therapeutic option over the last decade.
Death associated with IA in adult lupus patients was described in 50%,5,7 generally in patients with active disease5,7 and treated with very high immunosuppressive agents (such as azathioprine 5 and/or IVCYC),5,6 as evidenced in our series. In the two pediatric cases reported in the literature with JSLE and IA, one of them died. 1 Therefore, it is important to highlight the need for suspicion of opportunistic infections from the first moment an immunocompromised patient suffers fever and lung disease.
IA may simulate sepsis, as shown in our cases, and this infection may be underestimated in the lupus population due to the fact that various rheumatologic services do not carry out necropsy systematically, as it was performed in four of our cases. 1 Additionally, it is important to investigate every fluid and/or tissue available to confirm IA diagnosis. 14
In conclusion, IA is a severe opportunistic infection that may mimic JSLE manifestations in patients with active disease receiving immunosuppressive agents. This study reinforces the importance of early diagnosis and antifungal therapy, especially in critically ill patients.
Footnotes
Acknowledgements
We thank colleagues in the Pediatric Infectology, Neurology and Intensive Care Units of our University Hospital.
Funding
This study was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo – FAPESP (grant #08/58238-4 to CAS), by Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPQ (302724/2011-7 to CAS) and Federico Foundation to CAS.
Conflict of interest
None declared