
Abstract
Colitis in patients with systemic lupus erythematosus (SLE) is quite rare. It can be caused by intestinal vasculitis, mesenteric vascular thrombosis, concomitant inflammatory bowel disease or infectious colitis. It is important to make an accurate and early diagnosis as the treatments for each condition differ and a delayed diagnosis can result in life-threatening complications. However, non-specific gastrointestinal symptoms make a timely diagnosis challenging. Amoebic colitis is a rare condition in patients with SLE. Here we present a case of fulminant amoebic colitis in a patient with SLE which was initially misdiagnosed as ischemic colitis due to intestinal vasculitis. Her colitis was complicated with multiple intestinal perforations, disseminated intravascular coagulation and acute respiratory distress syndrome; but in the end, the patient was successfully treated with metronidazole and paromomycin.
Introduction
Gastrointestinal manifestations are common and appear in variable forms in patients with systemic lupus erythematosus (SLE). 1 Among them, large bowel involvement is relatively rare. It can be either SLE-related (e.g. ischemic colitis due to intestinal vasculitis, mesenteric vascular thrombosis) or non-SLE related (e.g. concomitant inflammatory bowel disease, infectious colitis). Therefore, for proper management, it is important to distinguish the infectious colitis from those conditions that are treated with corticosteroids. Some of them may present as ‘acute abdomen’ such as intestinal perforation. In these cases, surgical treatment should not be delayed, or life-threatening complications could occur.
Amoebic colitis is a rare condition in patients with SLE. However, a delayed diagnosis can result in fulminant amoebic colitis associated with a high rate of intestinal perforation and mortality. Here we report a case of fulminant amoebic colitis in a patient with SLE that was initially misdiagnosed as ischemic colitis due to intestinal vasculitis.
Case report
A 47-year-old woman presented at the emergency department in August of 2010 with approximately 500 cc of hematochezia and abdominal pain which had developed on that day. She had been diagnosed with SLE in 1998 and was taking 5 mg of prednisolone, 100 mg of hydroxychloroquine and a calcium supplement tablet. She had been hospitalized with hemolytic anemia two weeks before the visit and was given 100 mg of methylprednisolone per day for six days and then was discharged and told to take 50 mg of oral prednisolone per day.
On examination, her blood pressure was 127/73 mmHg. Pulse rate, respiratory rate and body temperature were normal. Her abdomen was soft and flat with normal bowel sounds and tenderness was present at the periumbilical area but without any guarding or rebound tenderness.
The initial laboratory findings revealed a white blood cell count of 21,030/µl (neutrophils: 82%), a hemoglobin level of 10.7 g/dl, a platelet count of 374,000/µl, an erythrocyte sedimentation rate (ESR) of 11 mm/h and a C-reactive protein (CRP) level of 5 mg/dl (reference range, 0.01–0.47). The serum anti-nuclear antibody (ANA) level was 1:1600 with a speckled pattern, the serum C3/C4 level was 70/11.8, the anti-dsDNA level was 10.18 IU/ml (reference range, <7), the IgG anticardiolipin antibody level was 4.7U/ml (reference range, <10), the anti β2 glycoprotein I antibody level was 2.6 U/ml (reference range, <7), the lupus anticoagulant ratio was 1.1 (reference range, <1.3). Renal function and liver function tests were all within reference ranges. Stool microscopy revealed no parasitic ova and stool cultures revealed no pathogen.
Plain radiography of the abdomen showed no particular abnormality. On the computed tomography (CT) scan of the abdomen, edematous wall thickening along the cecum, ascending colon and proximal transverse colon was observed, suggesting non-specific colitis (Figure 1).
Abdomen computed tomography showed the non-specific colitis from the mid transverse colon to the rectum.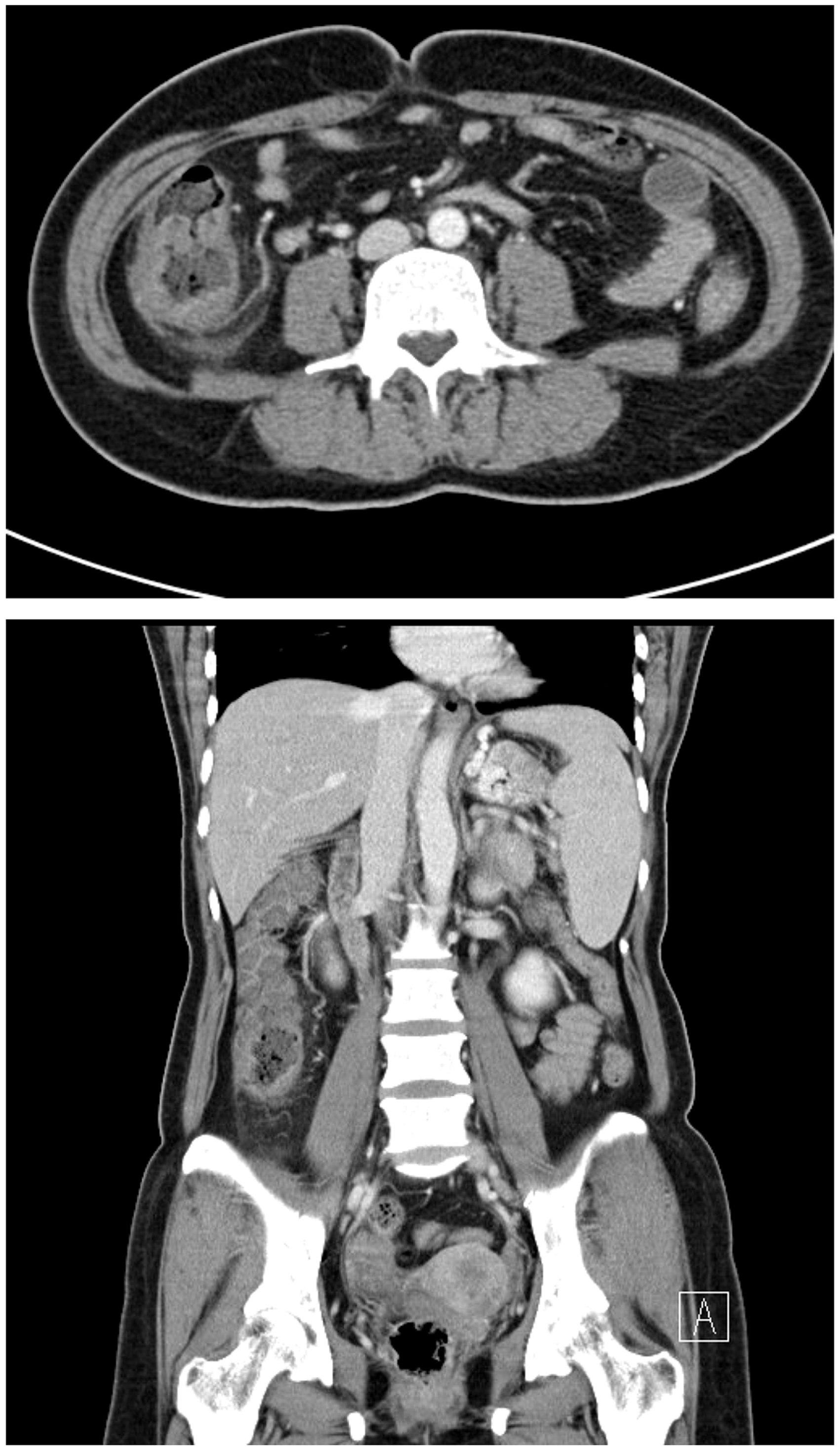
A provisional diagnosis of intestinal vasculitis was made and the patient was initially given 62.5 mg of methylprednisolone. Despite the treatment, abdominal pain and hematochezia persisted. On physical examination, tenderness on periumbilical area persisted, but the abdomen was soft and without rebound tenderness. Colonoscopy was performed on the fifth day of admission and it showed multiple ulcers with exudates and edematous mucosa from mid-transverse colon to rectum (Figure 2). Antibiotics (cefobactam 2 g t.i.d) were added to treat a possible infectious colitis. The biopsy result was consistent with active colitis with ulceration and there was no evidence of cytomegalovirus (CMV) or tuberculosis infection. Angiography of the mesenteric vessels was performed but showed only increased vascularity at the ascending colon and proximal transverse colon area without any vascular stenosis or leakage.
Colonoscopy showed multiple discrete ulcers.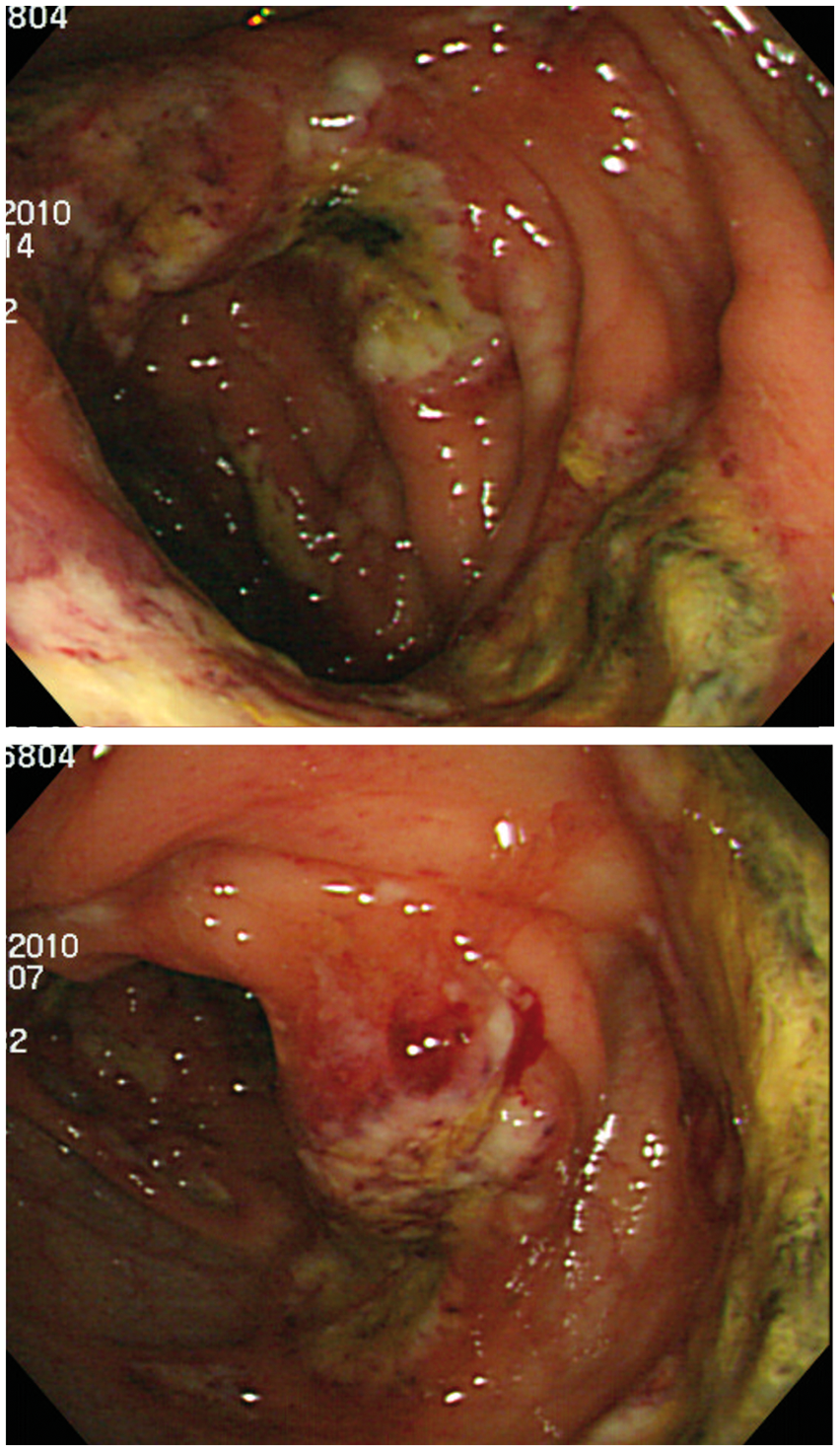
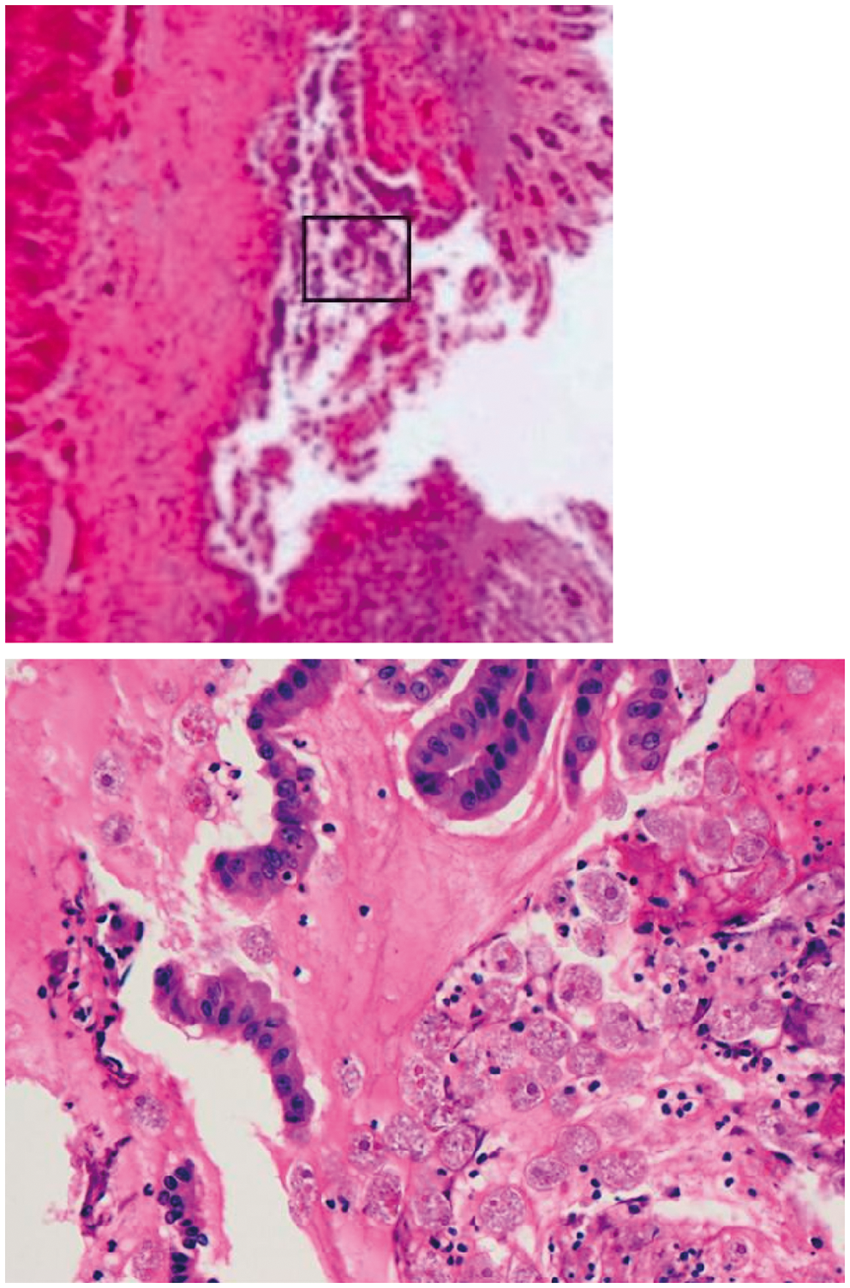
On the 18th day, the patient complained of worsened abdominal pain and the chest radiograph showed peritoneal free air. An emergency laparotomy was performed. Near total necrosis of the ascending colon with abscess formation was observed. Multiple perforations were found along the transverse colon, sigmoid colon and rectum (Figure 3). Total colectomy with end ileostomy was done. Tissue pathology showed Entamoeba trophozoites on PAS stains (Figure 4). The diagnosis of fulminant amoebic colitis was made and metronidazole treatment followed by paromomycin was started. Broad-spectrum antibiotics were added as well.
Gross specimen of the resected colon. Trophozoites of Entamoeba histolytica were seen on resected colon.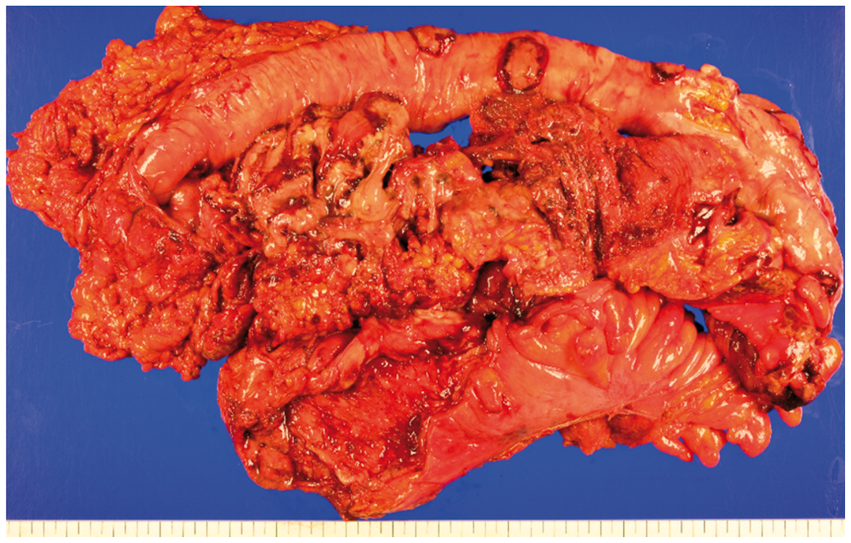
After the surgery, the patient’s condition was complicated with acute respiratory distress syndrome (ARDS) and disseminated intravascular coagulation (DIC). The patient was intubated for mechanical ventilation and received care in the intensive care unit (ICU). Her condition improved after a month, and she was discharged on 8 October 2010. She underwent ileostomy reversal surgery a month later.
Discussion
Gastrointestinal manifestations are common in patients with SLE and any area of the gastrointestinal tract may be involved. It may present as esophageal disease, mesenteric vasculitis, inflammatory bowel disease, pancreatitis, liver disease and peritonitis. 1 Lee et al. reported that 22% of patients with SLE experienced acute abdominal pain. The most common cause was lupus enteritis (intestinal vasculitis), accounting for up to 45% of the cases. 2 Lupus enteritis is caused by small vessel vasculitis of the bowel wall and mostly involves the jejunum and the ileum. 3 In contrast, ischemic colitis due to vasculitis is quite rare, developing in only 0.2% of patients. 4
Intestinal vasculitis has been reported to be associated with SLE activity. 5 Predisposing factors include the presence of concomitant vasculitis elsewhere, recent colonoscopy or barium enema, thrombocytopenia and high circulating rheumatoid factor. 6 Although several diagnostic tools are used, none of them achieves a pathognomic finding. CT scan of the abdomen may reveal ischemic bowel changes such as wall thickening, target signs, vascular engorgement or dilatation of bowel segments. Colonoscopy may demonstrate hemorrhages, edema and multiple discrete ulcers with exudates. Endoscopic biopsy specimens may reveal small vessel wall thickening with lymphocyte infiltration and hemorrhage. 5 However, all of the above signs can also be found in the cases of secondary vasculitis or infection. Therefore, the diagnosis of intestinal vasculitis should be made after thorough review of the clinical, laboratory and radiological findings. Corticosteroids are the treatment of choice, and in the steroid-resistant cases, combination therapy with cyclophosphamide 4 or rituximab 6 were reported to be successful.
Our patient presented with relatively low disease activity, had no history of thrombosis and her antiphospholipid antibodies were all negative. The affected site was the colon and just before admission she had received steroid pulse therapy due to hemolytic anemia. Therefore, we thought that there was a high possibility of infectious colitis and checked for a common bacterial infection or an opportunistic infection such as CMV and tuberculosis. However, a stool culture grew no pathologic bacteria, and there was no evidence of either CMV or mycobacterial infection. However, after a retrospective review, we think that because this patient had a greater possibility of developing infectious colitis than intestinal vasculitis we should have checked more thoroughly, including doing an assessment for less likely pathogens such as parasites.
Amoebic colitis is caused by Entamoeba histolytica invading the colonic wall. Although its prevalence is decreasing in developed countries, it remains one of the major causes of morbidity and mortality in developing countries (preschool children in Bangladesh had a 2.2% frequency). 7 In Korea, the prevalence of protozoan cyst infection was reported as 2.99% in 2006. The prevalence of E. histolytica infection was 0.6%. 8 Patients with amoebic colitis usually present with abdominal pain, weight loss and watery or bloody diarrhea, similar to gastrointestinal manifestations of SLE or non-infectious colitis such as inflammatory bowel diseases. The best approach to diagnosis is the combination of a stool antigen assay (by ELISA) or a DNA assay (by PCR) with a serological antibody test. 9 The sensitivity and the specificity of stool antigen or DNA detection is high compared with the traditional microscopic examination of the stool. Although the current serologic test has certain disadvantages (it remains positive for years after infection and a delayed seroconversion (2–4 weeks) is common 10 ), its combination with stool antigen or DNA detection is reported to offer the best diagnostic yield. 9 The traditional method of microscopic examination of the stool is still widely used but it has low sensitivity (25–60%) and cannot discriminate pathogenic E. hystolityca from non-pathogenic Entamoeba dispar or Entamoeba moshkovskii.10,11 It also failed to demonstrate the erythrophagocytic trophozoite, the hallmark of the amoebiasis in our patient. Neither a stool antigen assay nor a serologic antibody test was performed in this case as both were unavailable in our hospital. When the colonic biopsy was reviewed after the surgery, trophozoites were not discovered.
Fulminant amoebic colitis refers to the condition complicated with massive necrosis of wide segments of the large bowel, which is rare (occurring in less than 0.5% of cases), and is associated with high mortality (more than 40% of cases). 12 It usually occurs in the setting of poor nutrition, overcrowded housing and poor hygiene and has been reported in patients who received a high dose of corticosteroid therapy. 13 Delayed diagnosis of amoebic colitis can lead to fulminant amoebic colitis as well.
Treatment of amoebic colitis includes metronidazole followed by paromomycin. 14 In the case of fulminant amoebic colitis, broad spectrum antibiotics should be added to treat intestinal bacteria that may spill into the peritoneum. 11
In this case, trophozoites were fortunately found on the resected colon specimen and our patient was eventually successfully treated with metronidazole and paromomycin. If we had suspected and checked more thoroughly for rare infectious causes such as amoebic colitis we could have prevented the patient from developing fulminant colitis with serious complications.
Some rare pathogen infections other than amoebiasis have been reported in patients with SLE who presented with abdominal pain. Cryptococcal lymphadenitis 15 and Strongyloides stercoralis hypersensitivity syndrome 16 were reported in patients with SLE. These conditions should also be considered in differential diagnosis when patients do not respond well to the proper treatment for the assumed diagnosis.
Conclusion
Colitis is an uncommon manifestation in patients with SLE. However, when it occurs, it is important to distinguish infectious colitis from those conditions that can be treated by high dose corticosteroids such as ischemic colitis due to intestinal vasculitis because both conditions can be fatal with delayed diagnosis. Our patient suffered from a fulminant amoebic colitis complicated with multiple colonic perforations, ARDS and DIC due to delayed diagnosis.
To our knowledge, there has been only one other case that reported fulminant amoebic colitis in a patient with SLE. 12 In that case, diagnosis was also delayed and the patient died from multiorgan failure. Both cases teach us that parasitic infection should be considered when there is a substantial possibility of infection in a colitis case in an SLE patient in order to reduce mortality and serious complications. Once the diagnosis of colitis is made in a patient with SLE, amoebic colitis should also be taken into account and be excluded by stool antigen or DNA detection and serologic antibody test.
Footnotes
Funding
This research was supported by a grant from the Catholic university of Korea.
Conflict of interest statement
The authors have no conflicts of interests to declare.