
Abstract
Introduction
During recent years, the increased risk of cardiovascular disease (CVD) and atherosclerosis in systemic lupus erythematosus (SLE) have been much discussed. In SLE a combination of traditional and non-traditional risk factors contribute to the increased risk of CVD. 1 Traditional risk factors include hypertension, renal disease and dyslipidaemia, while the role of smoking varies between studies. Interestingly, accelerated atherosclerosis have been reported in SLE, more as increased prevalence of atherosclerotic plaques than as a generally increased intima-media thickness (IMT), which appears to be unchanged.2,3
Relatively little is known about associations between rheumatic disease and diet. In rheumatoid arthritis (RA) a gluten-free vegan diet could improve the situation.4,5 Also, Mediterranean diet has been reported to be beneficial.6,7 Further, omega-3 fatty acids (FAs) are in general believed to be anti-inflammatory, and studies indicate that substitution with such compounds may ameliorate rheumatic disease.8,9 On the other hand, omega-6 FAs have pro-inflammatory properties. 10
In SLE the knowledge is still scarce about the impact of diet on the disease. The aims of the present study were therefore to investigate the dietary habits in relation to FAs in subcutaneous adipose tissue (AT), disease activity and atherosclerosis.
Patients and methods
Study group
Altogether, the 114 patients with SLE included in the SLEVIC (SLE vascular impact cohort) study 11 were recruited. They fulfilled the 1982 revised criteria of the American College of Rheumatology (ACR) for SLE 12 and were younger than 70 years. Of the 114 patients, 42 were treated with glucocorticoids at the time of the study. Further, the 122 age- and sex-matched controls (recruited randomly from the same catchment area), also recruited to the SLEVIC study, agreed to participate. The study was approved by the Karolinska Institutet research ethics committee and is in accordance with the Helsinki Declaration. All subjects gave informed consent before entering the study.
Assessments
The investigation included written questionnaires, an interview and physical examination by a rheumatologist, laboratory measurements, subcutaneous abdominal fat cell aspiration and ultrasound examination of the carotid arteries.
Disease activity and damage
SLE activity was determined by the Systemic Lupus Activity Measure (SLAM), which is a global score assessing overall disease activity occurring in the month preceding the assessment with a score ranging from 0 to 84, 13 and also with Systemic Lupus Erythematosus Disease Activity Index (SLEDAI). 14 SLEDAI includes the manifestations most commonly contributing to disease activity and are scored based on the presence or absence within 10 days of the evaluation.
Organ damage was determined with Systemic Lupus International Collaborating Clinics (SLICC) damage index. 15 This index includes cumulative damage in 12 organ systems since the onset of SLE, with a score ranging from 0 to 47.
Dietary assessment
A self-administered, semi-quantitative food frequency questionnaire (FFQ) was used. 16 In that the participants were asked to report their frequency of use of 88 food items and beverages over the past year. The nutrient calculations were carried out using nutrient composition values from the Swedish National Food Administration data. 17 The intake of nutrients was computed by multiplying the frequency of consumption of each food item by the nutrient content of the specified portions. Dietary intake is described as the percentage of total intake. According to the Swedish National Food Administration the proportions (energy percentage, E%) of carbohydrate, protein and fat should be 55–65 E%, 10–15 E% and 25–35 E%, respectively, for normally active individuals. For less active individuals the recommendations are 55 E%, 16 E% and 28 E%, respectively. 18
Assays
Venous blood samples were collected between 07:30 and 10:00 after an overnight fast. The biochemical variables were determined by standard laboratory methods. They included, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), blood lipids and lipoproteins.
Subcutaneous abdominal fat cells were aspirated with a needle attached to a vacuum tube and stored at −70 C until analysed for FAs. The FA composition of subcutaneous AT was analysed by gas liquid chromatography as described previously. 19 The amounts of FAs were given as the relative percentage of the sum of the FAs analysed.
Carotid B-mode ultrasonography
The right and left carotid arteries were examined with a duplex scanner (Sequoia, Siemens Acuson, Mountain View, CA, USA) using a 6 MHz linear array transducer. The intima-media thickness (IMT) was defined as the distance between the leading edge of the lumen-intima echo and the leading edge of the media-adventitia echo in the far wall. The examinations were digitally stored for subsequent analyses by a computer system 20 with automated tracing of echo interfaces and measurements of distances between the wall echoes within a 10 mm long section of common carotid artery (CCA) in late diastole, defined by a simultaneous electrocardiographic recording. The mean values of the IMT within the 10 mm long section were calculated. When a plaque was observed in the region of the CCA measurements, the IMT was not measured.
Carotid plaque was defined as a localized IMT of >1 mm and at least a 100 per cent increase in thickness compared with adjacent wall segments. Plaque was screened for in the common, internal and external carotid arteries. Plaque occurrence was scored as the absence of plaque, the presence of unilateral plaque and the presence of bilateral plaque.
The differences between repeated measurements of IMT, by using the automated analysing system, were 4.9 per cent (coefficient of variation), with an IMT of 0.44–1.02 mm. The ultrasonographic methods used have been described in detail previously.21,22
Statistics
The results were dichotomized or determined as continuous variables as indicated. We calculated percentiles based on distributions in the whole study group. Age, gender and geography were matched by the design of the study. Data are presented as means (with 95% confidence intervals, CI) or medians (with interquartile ranges, IQRs) depending on their distribution. Comparisons between groups were made with the Mann–Whitney U test, median test or Student’s t test. To evaluate the association between intake of FAs in the diet and their relative content in AT Spearman rank correlation analysis was used. Spearman rank correlation analysis was also used to evaluate the associations between measurements of the SLE disease and atherosclerosis. P-values <0.05 were considered significant. The statistical analysis program STATISTICA 9 (Stat Soft Scandinavia AB, Uppsala, Sweden) was used for statistical analysis.
Results
Demographic and disease characteristics among SLE patients and controls 11
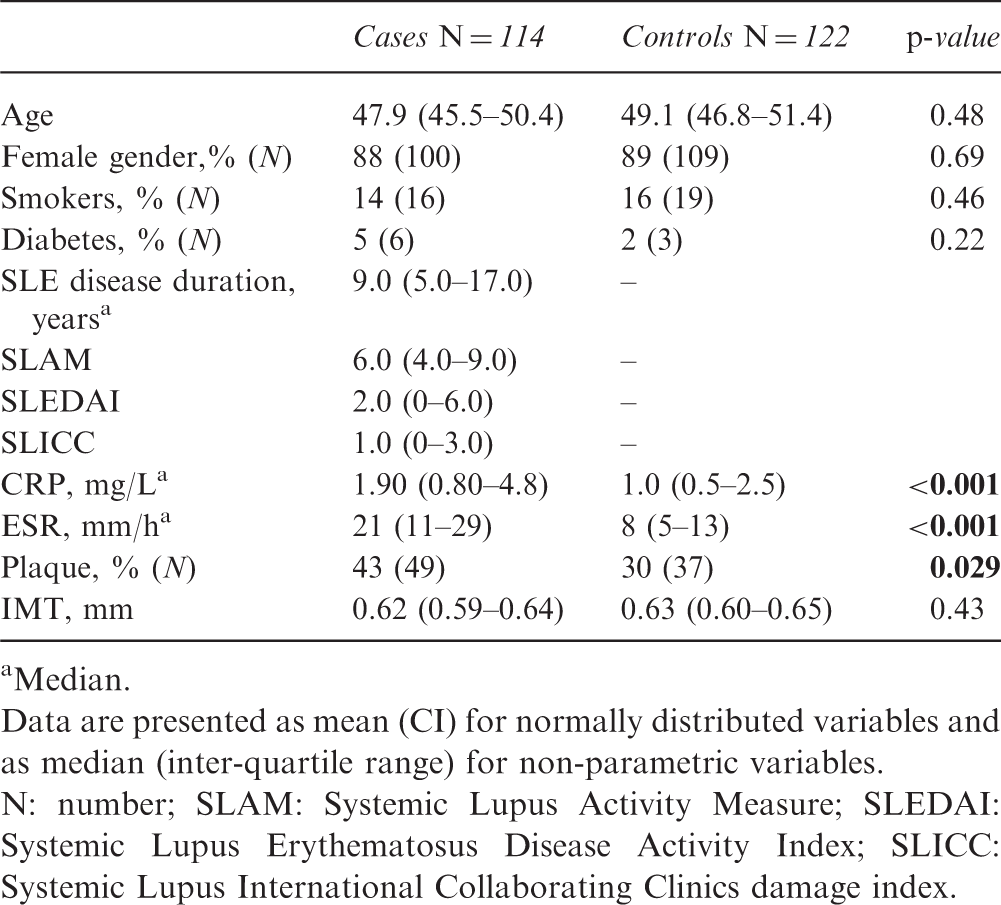
Median.
Data are presented as mean (CI) for normally distributed variables and as median (inter-quartile range) for non-parametric variables.
N: number; SLAM: Systemic Lupus Activity Measure; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SLICC: Systemic Lupus International Collaborating Clinics damage index.
Dietary intake and fatty acid profiles in adipose tissue
Dietary intake among the SLE cases and controls
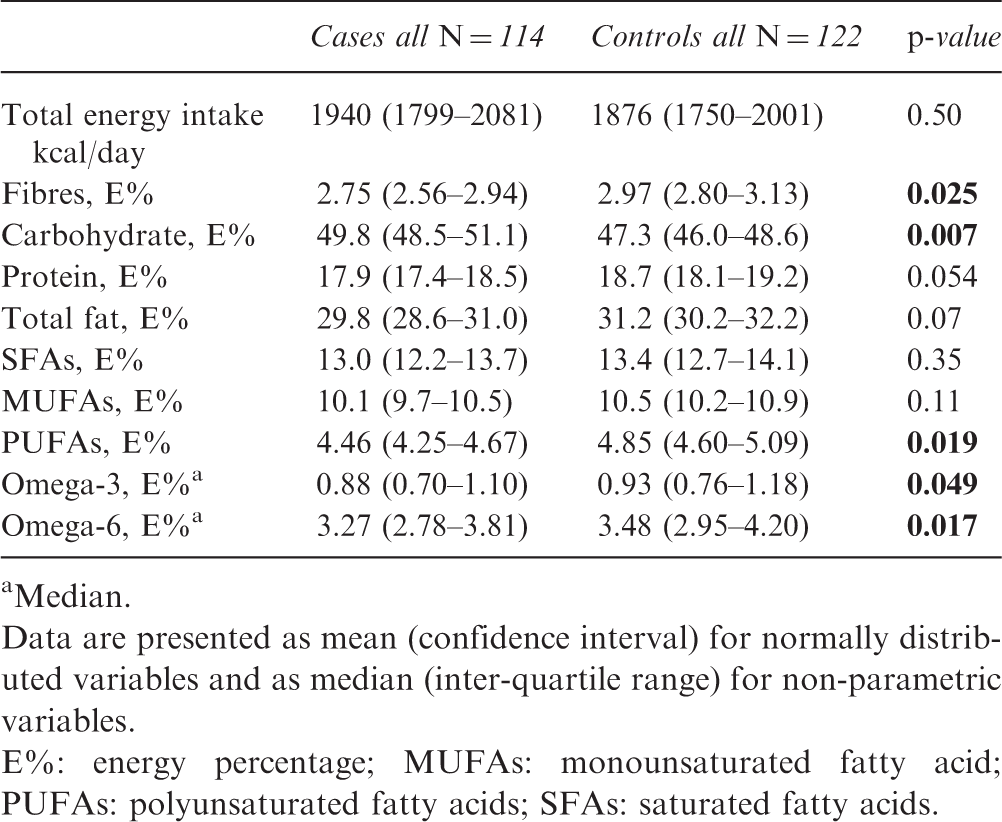
Median.
Data are presented as mean (confidence interval) for normally distributed variables and as median (inter-quartile range) for non-parametric variables.
E%: energy percentage; MUFAs: monounsaturated fatty acid; PUFAs: polyunsaturated fatty acids; SFAs: saturated fatty acids.
There were no significant differences in total energy intake between patients and controls and the total intake was comparable with the Swedish Food Recommendations. 18 However, as to the diet composition the patients with SLE reported significantly higher intake of carbohydrate, with significant lower fibre intake, and significantly lower intake of poly-unsaturated fatty acids (PUFAs), that is, omega-3 and omega-6, than the controls.
The reported dietary intake, by both patients and controls, of the omega-3 essential FAs, eicosapentaenoic acid (EPA, 20:5 n3) and docosahexaenoic-acid (DHA, 22:6 n3) correlated significantly with that in AT, r = 0.35, p ≤ 0.001 and r = 0.40, p ≤ 0.001, respectively. The dietary linoleic acid (FA 18:2 n6) correlated significantly with that in AT (r = 0.18, p = 0.010). However, dietary arachidonic acid (FA 20:4 n6) did not correlate at all. This is probably a reflection of the role this FA has in the inflammatory process. These results verify the reliability of the long-term FA intake according to the FFQ.
The patients’ dietary intake of carbohydrates E% correlated significantly and positively with linoleic acid (18:2 n6) in AT (r = 0.38, p < 0.001). This was also verified when subdividing the intake into tertiles. Thus the patients with SLE who had the highest intake of carbohydrate, that is the third tertile, had significantly higher levels of 18:2 n6 in their AT, than those with the lowest intake, that is, the first tertile, of carbohydrate (p = 0.011).
Dietary intake and adipose fatty acids: associations with SLE disease
Dietary intake of carbohydrates E%, fibres E%, saturated fatty acids and total monounsaturated fatty acids did not significantly correlate with SLAM, SLEDAI or SLICC (data not shown). On the other hand dietary intake of the omega-6 fatty acid linoleic acid (18:2 n6) correlated positively with SLAM (r = 0.21, p = 0.028), but not with SLEDAI and SLICC.
Spearman correlation coefficients between relative (percentage of total fat) FA content in adipose tissue and the SLE disease
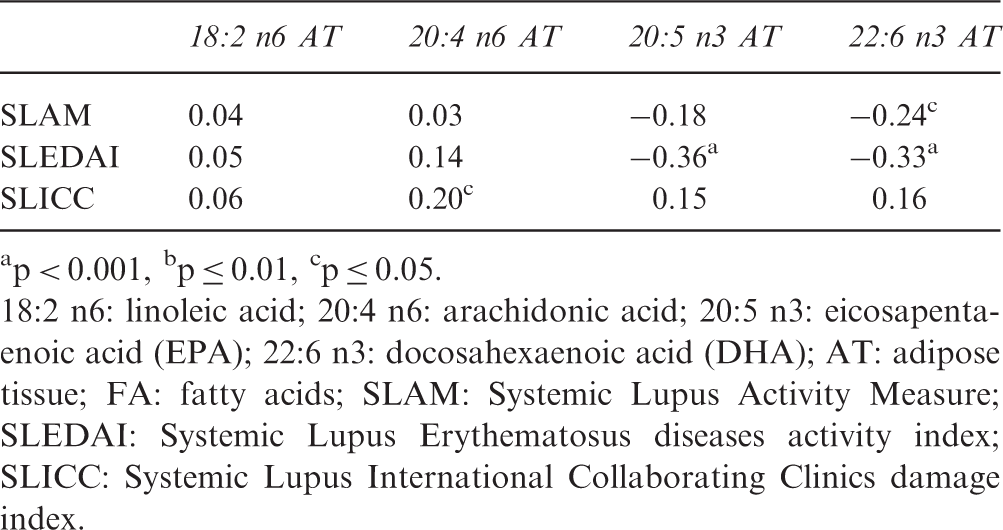
p < 0.001, bp ≤ 0.01, cp ≤ 0.05.
18:2 n6: linoleic acid; 20:4 n6: arachidonic acid; 20:5 n3: eicosapentaenoic acid (EPA); 22:6 n3: docosahexaenoic acid (DHA); AT: adipose tissue; FA: fatty acids; SLAM: Systemic Lupus Activity Measure; SLEDAI: Systemic Lupus Erythematosus diseases activity index; SLICC: Systemic Lupus International Collaborating Clinics damage index.
Carbohydrate intake and AT fatty acids: associations with serum lipids among patients with SLE
Dietary intake of carbohydrate E%, correlated significantly and negatively with serum HDL (r = −0.28, p = 0.003) as well as with apoA1 (r = −0.27, p = 0.005) whereas fibre E% did not significantly correlate with these serum lipids. Concerning the FAs in AT, both DHA and EPA correlated positively with serum apoA1, r = 0.29, p = 0.004 and r = 0.22, p = 0.029, respectively. Linoleic acid (18:2 n6) correlated negatively with apoA1, r = −0.21, p = 0.037. No significant correlations were found between dietary intake of carbohydrate E%, omega-3 and omega-6 or AT omega-3 and omega-6 and triglycerides.
Occurrence of plaque
As reported earlier these patients with SLE had an increased occurrence of plaque in the carotid arteries compared with the controls, 42.98 per cent (n = 49) versus 30.32 per cent (n = 37), p = 0.029, whereas carotid intima measures (IMT) were similar. 11
Both patients and controls with plaque were older than those without (p < 0.001). The patients with plaque had a longer disease duration and were more damaged, according to SLICC (p = 0.038) than those without plaque. The total intake of glucocorticoid medications was not associated with atherosclerotic plaques. 11
Relationship between dietary intake, AT fatty acid profile, serum lipids and occurrence of plaque among the patients with SLE
Spearman correlation coefficients between fatty acids in adipose tissue and plaque occurrence among patients with SLE (N = 114)
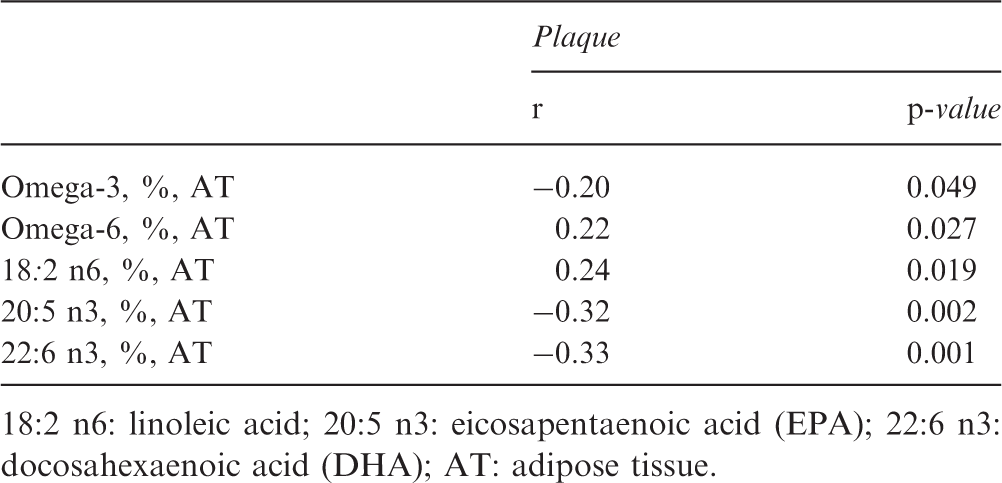
18:2 n6: linoleic acid; 20:5 n3: eicosapentaenoic acid (EPA); 22:6 n3: docosahexaenoic acid (DHA); AT: adipose tissue.
The significant positive correlation between dietary intake of carbohydrate E% and AT omega-6, mentioned above, differed in potency dependant on plaque presence or not. Thus, in patients with plaque the coefficient was r = 0.45, p < 0.001, whereas a weaker correlation was found among those without plaque (r = 0.29, p = 0.05).
Discussion
We report here that patients with SLE consume less PUFAs and fibres and more carbohydrates, as compared with age- and sex-matched healthy controls, and that the dietary intake of essential FAs was well reflected in AT FA content. An important finding was that among the patients the AT content of omega-3 was negatively associated with disease activity and plaque presence and positively with serum apoA1. The AT omega-6 FA was positively associated with SLE damage and plaque presence but negatively with serum apoA1. Furthermore, among the patients, the dietary intake of carbohydrates was not associated with disease activity or severity, but was positively correlated with AT omega-6 and negatively with serum HDL and apoA1.
The reliability of the long-term FA intake according to the FFQ was verified by the significant correlations found between the PUFAs ingested and those in AT in subcutaneous fat from the abdominal region. PUFAs in AT are largely exogenous and hence valid markers to assess dietary intake.23,24
Lifestyle factors in SLE have not been much studied, and to the best of our knowledge, this is the first time dietary factors are studied in more detail in SLE. Even though it is recognized that in the general population diet may play a major role in disease, especially CVD, it has been difficult to demonstrate exactly how with the same certainty as in controlled double-blinded studies on medications. Recently, the role of different macro-nutrients in the diet as risk factors for atherosclerosis and CVD has been debated and re-evaluated. While diet recommendations typically include decreases in fat and especially saturated fat, 25 it has been difficult to demonstrate their efficacy in controlled studies. In the largest intervention study, Women’s Health Initiative (WHI), reduced total fat intake and increased intakes of vegetables, fruits and grains did not significantly reduce the risk of CVD in postmenopausal women and achieved only modest effects on CVD risk factors including blood lipids. 26
Among the present patients with SLE the intake of PUFAs was significantly decreased compared with controls, while there were no differences in monounsaturated and saturated fat. Studies on SLE and intake of omega-3 are scarce but in a study from 2004, supplementation with omega-3 fish oils was found to reduce symptomatic disease activity. 27 Such a benefit of omega-3 is supported by the present finding that AT omega-3 was negatively associated with disease activity.
The impact of dietary omega-3, especially EPA (20:5n-3) and DHA (22:6 n-3) on rheumatoid inflammation has been investigated in many studies. Several randomized controlled studies have shown that supplementation with fish oil in addition to ordinary pharmacological treatment results in beneficial effects on RA symptoms, such as decreased number of tender and swollen joints as well as an NSAID-sparing effect.8,9
With regard to inflammation it is often considered that it is the PUFAs omega-3 and omega-6 that are most important, these often acting to oppose one another’s actions, which could explain the opposite correlations found here for AT omega-3 and omega-6 with disease activity and plaque occurrence. Cells involved in the inflammatory response are typically rich in the omega-6 FA, arachidonic acid (a metabolite of linoleic acid) which is a precursor to inflammatory eicosanoids. 28 Eicosanoids produced from arachidonic acid include various prostaglandins, thromboxanes and leucotrienes. These have well-established roles in regulation of inflammation, immunity and platelet aggregation. 29 It is possible that these mechanisms have an impact on the development of atherosclerosis. Interesting to note is that there are data suggesting that atherosclerotic plaques can incorporate the omega-3 FA EPA, and that a higher content of EPA in carotid plaques is associated with a reduced number of foam cells and T cells, less inflammation and increased stability. 30 Further, AT content of EPA and DHA, has been shown to be significantly lower in subjects suffering a primary non-fatal MI than in healthy controls. 31
The above mentioned reports on the beneficial effect of omega-3 FAs are supported by the present findings that AT omega-3 were positively associated with serum apoA1 and negatively with plaque presence. Convincing evidence from extensive research over the past three decades points out the potential beneficial effects of omega-3 in primary prevention, CHD, post-MI and atherosclerosis. 32
Another finding in the present study is that intake of fibre was lower and intake of carbohydrates higher, among patients with SLE as compared with the controls. The role of fibre intake in human disease is less debated than other macro nutrients, and many studies indicate that fibre intake is negatively associated with human disease. 33 Recommendations regarding carbohydrates depend on factors including glycaemic index (GI) and there is thus a consensus that fast carbohydrates are negative. A caveat in the present study is that the design does not allow for detailed analysis of type of carbohydrates involved. It is, however, interesting to note that low carbohydrate intake was associated with high HDL and apoA1, while high carbohydrate intake had opposite associations. This could be a reflection of the low fibre content in the diet. HDL may be an important factor in SLE, due to its anti-inflammatory and anti-atherogenic properties.1,2,34,35
Interestingly, carbohydrate intake has recently been implicated as a risk factor for CVD, especially refined carbohydrates which promote a swift increase in blood glucose, with ensuing insulin increases. 36 In line with this, diabetics in the WHI study experienced an adverse glycaemic effect of the low-fat diet 37 and an opinion appearing to be on the rise is that dietary efforts to improve the CVD risk should emphasize limitation of refined carbohydrate intake and a reduction in excess adiposity. 36
The limitations of the current study should be acknowledged. The cross-sectional design of our study limits the ability to ascribe causal relationships to the associations detected. Cross-sectional studies only provide a ‘snapshot’ of the outcome and the characteristics associated with it at a specific point in time.
Taken together, our findings indicate that the dietary patterns among the patients with SLE are different from a population-based control group, with lower intake of PUFAs, decreased intake of fibres and increased intake of carbohydrates. This diet may in different ways, directly or indirectly, contribute to increased inflammatory activity, disease damage, unfavourable lipid profile in serum and atherosclerosis.
Footnotes
Acknowledgements
We are grateful to the registered nurses Margareta Wörnert, Mona Westvall and Eva Waldheim for collecting clinical data and administration of patients and to Niclas Håkansson for statistical help.
Author contributions
J Frostegård and AC Elkan had the main responsibility for drafting the article, all authors were involved in revising it critically for important intellectual content, and all authors approved the final version to be published. J Frostegård and AC Elkan had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
This study was supported by the Swedish Research Council, The regional agreement on medical training and clinical research (ALF) between Stockholm county council and the Karolinska Institutet, the King Gustav V 80 years foundation, The Swedish Rheumatism Association, CIDaT, Vinnova and the 6th Framework Program of the European Union, Priority 1: Life sciences, genomics and biotechnology for health (grant LSHM-CT-2006-037227 CVDIMMUNE) with JF as coordinator.
Conflict of interest
The authors have no conflicts of interest to declare.