
Abstract

Introduction
The most well-described neonatal autoimmune disease is neonatal lupus.
In higher organisms such as humans and other mammals, the development of the immune system begins as early as the first trimester. The goal of the immune system is to protect the host against danger. Danger to the host may take the form of infectious agents or may originate from the organism itself, as in the case of tumor cells. Other dangers include environmental agents such as toxins and even physical threats. The innate immune system can recognize danger-associated molecular patterns (DAMPS) and pathogen-associated molecular patterns (PAMPS), 1 but it is the adaptive immune system, with its diverse repertoire of antibodies and T cell recognition capabilities that allows for greater response amplification and specificity to defend against foreign invaders.
In order to develop such an effective system, the organism must strike a balance, as the development of a ‘better’ immune system is accompanied by a greater possibility that the immune system may inadvertently be directed against normal host tissues. In the fetus and neonate, both quantitative and functional defects in immune response exist not only because of the immaturity of the developing immune system, but also because of the expression of inhibitory receptors in neonatal immune cells 2 that leads to an overall suppression of the immune response. This is by design, as these conditions are necessary to mediate the development of tolerance to self-antigens, which is a very crucial process in preventing autoimmune disease. During this process, the effectiveness of this developing system against self-antigens is impaired, possibly providing an explanation as to why primary neonatal autoimmune disease is so rare.
In neonatal lupus, it is the transfer of maternal antibodies directed against the fetus or neonate that is most closely associated with clinical manifestations of the disease. The clinical syndrome most severely affects the heart, leading to varying degrees of heart block that may be fatal to the fetus or neonate. Though the transfer of these antibodies is mediated by an active transfer process involving the neonatal Fc receptor, the overall pathogenesis in neonatal autoimmunity has historically been considered to involve only passive immunity.
Autoantigensin neonatal autoimmune diseases
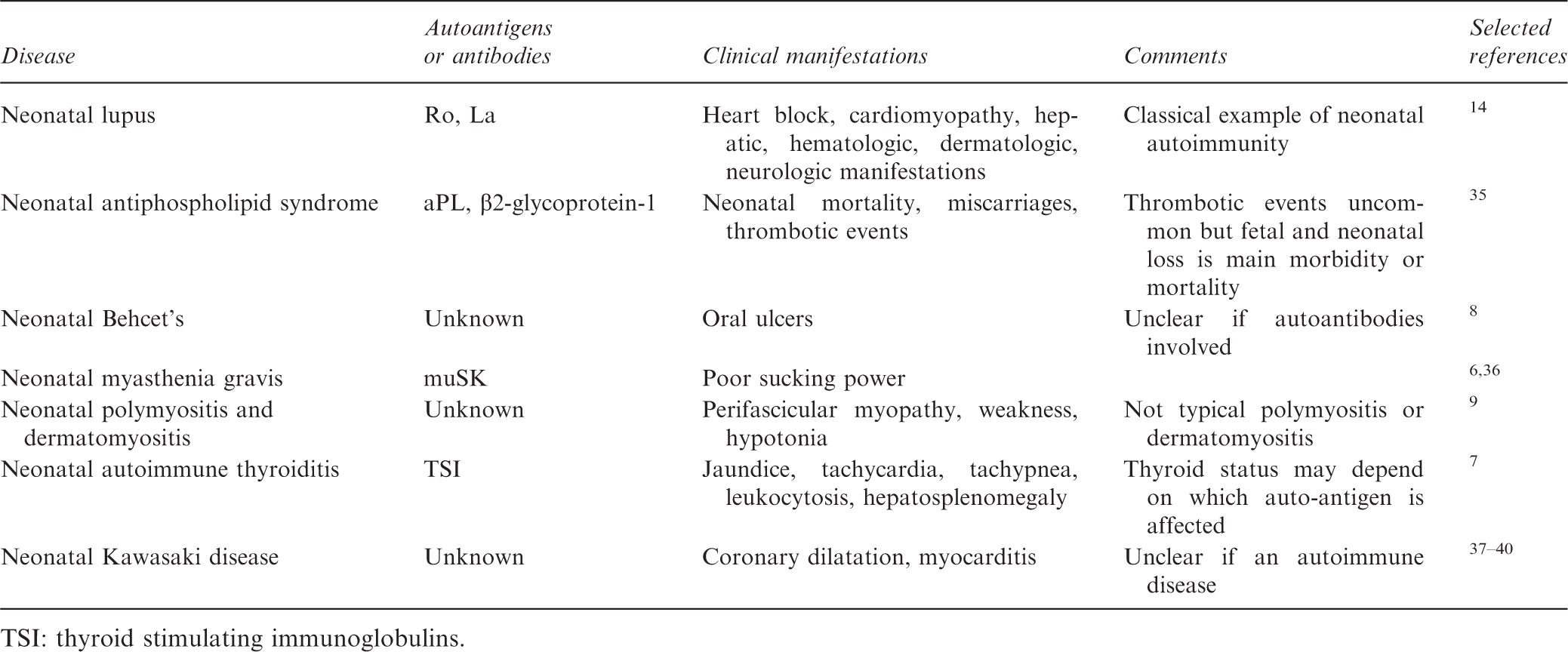
TSI: thyroid stimulating immunoglobulins.
Epidemiology of neonatal autoimmune diseases
A recent review from Italy retrospectively studied 136 pregnancies in 107 lupus patients with an average age of 29 years. Of these, 50% had anti-Ro and anti-La antibodies, and 29% had antiphospholipid antibodies. There were 125 live births and one neonatal death. Eight miscarriages and three artificial terminations accounted for the remaining 11 pregnancies. Prematurity (25%) and fetal growth restriction (14%) were significant morbidities. Interestingly, in their series there were no patients with neonatal lupus or congenital heart block. 10 A United States study in 2011 evaluated 325 neonates born to mothers with anti-Ro antibodies who had cardiac manifestations of neonatal lupus. 11 The mortality rate was 17.5% with about a third of these dying in utero. In patients with structural defects including dilated cardiomyopathy or endocardial fibroelastosis, the mortality rate was four times higher. Ultimately, 70% of patients with congenital heart block needed cardiac pacing. Most studies have demonstrated that the incidence of heart block in neonates born to mothers with positive antibodies is only about 2%,12,13 but this rate increases dramatically if the mother has a history of having a previous child with either heart block 14 or cutaneous manifestations.15,16
Clinical manifestations of neonatal autoimmunity
Skin manifestations include telangiectasias or annular or polycyclic erythematous plaques. These usually appear a few days or weeks after birth and resolve spontaneously.17,18 Hepatic manifestations range from transient, mild elevations of transaminases to fulminant liver failure.19,20 Hematologic manifestations include thrombocytopenia which occurs in 10% of patients who present with other manifestations of neonatal lupus. 21 In rare cases, neutropenia may also be present. 22
The cardiac manifestations constitute the major reason for fetal and neonatal mortality and morbidity. The degree of heart block may be variable, ranging from first degree heart block to complete atrioventricular (AV) block. 23 In almost all infants with higher degrees of AV block, the cardiac arrhythmia is progressive. If the diagnosis is made in utero, there is a 43% mortality rate, compared with a 6% rate among those infants with heart block diagnosed in the neonatal period. Hydrops is a potential complication of advanced heart block in neonatal lupus. 24
Pathogenesis of neonatal lupus
The degree to which these antibodies are pathogenic is still a matter of debate. If antibodies were the sole culprit, then all babies born to mothers with these antibodies would be affected. Furthermore, if these antibodies were pathologic, then how does one explain the lack of cardiac arrhythmias in the mother herself? These considerations would suggest that there are other factors which regulate the clinical expression of neonatal lupus.
Perhaps the most intriguing of all of the many speculative theories involves the role of apoptosis. 25 Apoptosis has been shown to play a role in the development of classical lupus and drug-induced lupus. The process is a necessary mechanism to maintain homeostasis of the immune system. Apoptosis controls the clearance of nuclear material and may play a role in the prevention of classical autoimmunity by limiting the exposure of reactive T cells to antigenic nuclear material. However, in the case of neonatal autoimmune diseases, it has been shown by cellular staining experiments that Ro and La antigens are normally intra-nuclear in non-apoptotic cells, 26 but when apoptosis ensues, these antigens slowly migrate from the nucleus through the cytoplasm to the cell surface. In the human, antibodies begin to cross the placenta at about 12 or 13 weeks of gestation, with acceleration of this process at about 22 weeks. It has been hypothesized that it is a combination of the timing of exposure of expression of Ro and La on the cell surface during normal apoptosis, coupled with the crossing of antibodies across the placenta that may induce conditions favorable to antigen-antibody cross-linking that may lead to the development of pathology.
In addition, the possibility that there may be neonatal cardiac antigens with cross-reactivity to anti-Ro and anti-La antibodies has not been ruled out. One group has identified the autoantibody binding site of autoantibodies to be a part of the alpha (1D) L-type calcium channel, providing a mechanism for tissue injury leading to heart block. 27 The role of genetics in the pathology of neonatal lupus has not yet been studied adequately. Like most autoimmune disease, both genetic and epigenetic factors may accompany environmental triggers leading to manifestations of the disease. HLA studies in neonatal autoimmunity have demonstrated an association between DR3/DR2 with maternal anti-Ro and anti-La antibodies, but this does not translate to a clinical association of neonatal lupus. 28 A higher incidence of HLA-Cw3 has been suggested in neonates with lupus. 29 A genetic risk variant at loci 6p21 has been found to be associated with neonatal lupus and it was demonstrated that the risk alleles were inherited by the mothers of children with neonatal lupus from their maternal grandparents. 30
Other pathogenic mechanisms may involve a depletion or immaturity of regulatory T cells in the neonate. 31 This allows an autoimmune process to go unchecked, but cannot by itself explain why this preferentially leads to cardiac effects. Maternal microchimerism, whereby maternal cells cross the placenta and co-habitate with fetal cells for many years, has been suggested as a possible cellular mediated mechanism that may contribute to the pathogenesis of neonatal lupus, but this is speculative and not well defined. 32 This mechanism would be analogous to a graft versus host disease process whereby maternal cells may attack fetal or neonatal cardiac tissue.
It is not known which of these mechanisms may actually be responsible for the clinical phenotype of neonatal immunity. One or more of these mechanisms may contribute to disease, or there may be some as yet undiscovered pathway that may prove to be more important in the development of neonatal lupus. Like other diseases, we are finding that multiple genetic and environmental factors frequently contribute to actual clinical illness. Figure 1 illustrates the possible pathophysiologic pathways that may contribute to the development of neonatal lupus.
Potential factors in the pathogenesis of neonatal lupus.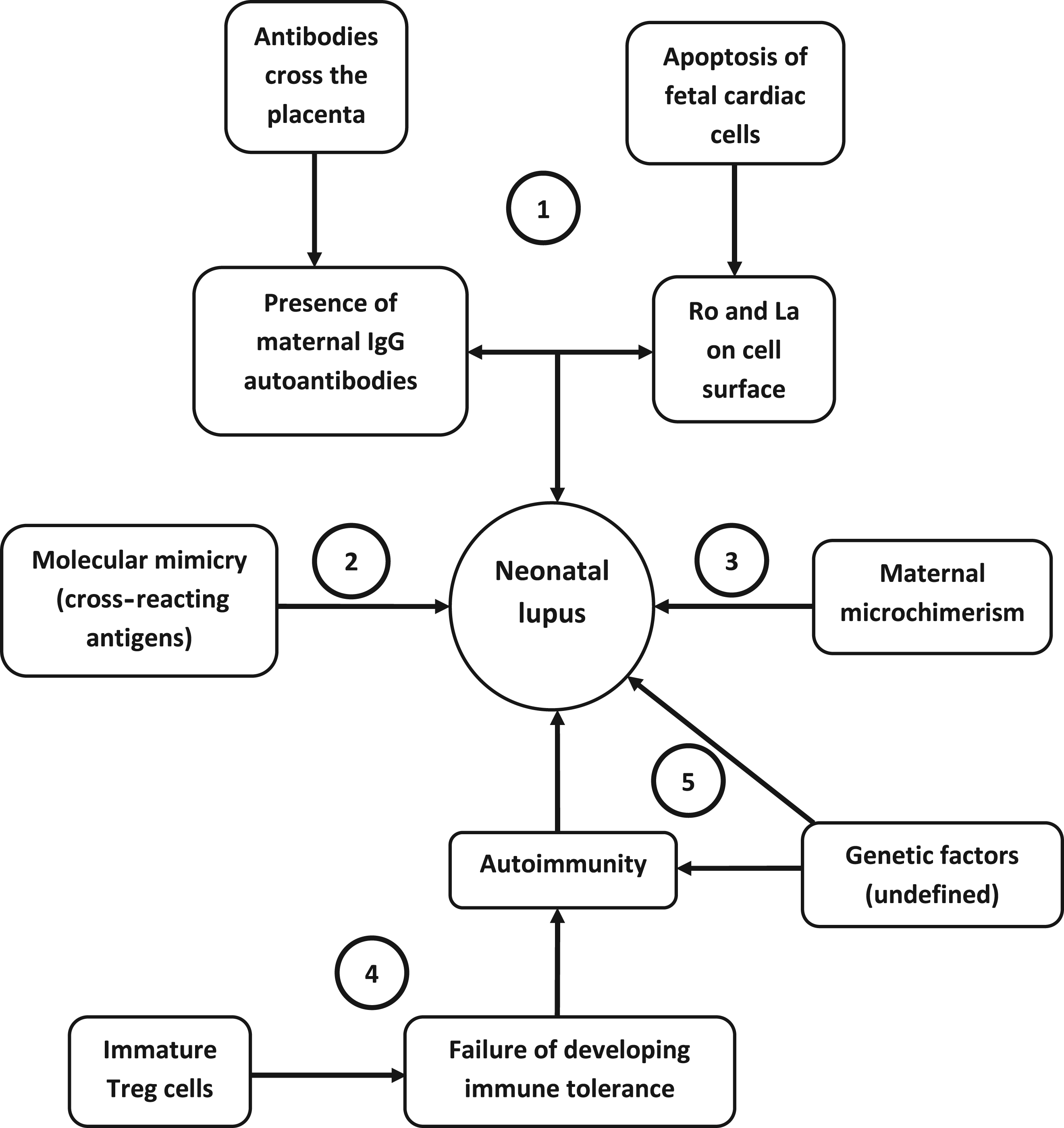
The prognosis and treatment of neonatal autoimmune diseases
The treatment of neonatal autoimmune disease is generally supportive. Treatment of the mother with corticosteroids during pregnancy has yielded poor results. 33 Intravenous gamma globulin has been used to prevent the development of congenital heart block in susceptible neonates with no adverse effects but with undetermined efficacy. Hydroxychloroquine given to anti-Ro positive mothers appeared to reduce the risk of cardiac manifestations of neonatal lupus in a case control study of 275 pregnancies. 34
Supportive management remains the mainstay of treatment, but studies have shown that most patients with second degree heart block or worse develop progressive disease and almost all of these patients ultimately require cardiac pacing. 11 Patient and family education and counseling is an important part of the management of pregnancy in mothers who possess anti-Ro and anti-La antibodies.
Summary
Neonatal autoimmune disease, at first glance, may appear to be mediated by autoantibodies. But manifestations of the illness require pathogenic events that extend beyond an antigen–antibody complex formation, and may involve a multitude of factors, including apoptosis, microchimerism, molecular mimicry, T cells, and the overall immunodeficient state of the fetus or neonate. Understanding of these factors may provide information leading to improved outcomes in the treatment and management of neonatal autoimmune diseases.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author has no conflict of interest to declare.