
Abstract
This study assessed temporal trends in characteristics and outcome of the intensive care unit (ICU) patients with systemic lupus erythematosus (SLE). We analyzed 2870 SLE patients (≥15 years) with first-time ICU admission between 1999 and 2008. Patient data were retrieved from the Taiwan National Health Insurance Research Database. Median age of the patients increased from 38.5 to 44.0 years during the study period. Most patients were women (overall 85.5%); the proportion varied insignificantly over time. Median duration from SLE diagnosis to ICU admission (disease duration) increased by four years. The proportion of patients with disease duration of more than three years increased from 42.6% to 61.4%, whereas the proportion of patients with a primary rheumatic diagnosis decreased from 41.7% to 25.1%. The incidence of infection increased from 39.1% to 47.2%. The incidence of organ dysfunction increased from 64.1% to 69.2%, especially in neurological, cardiovascular, and respiratory systems. Conversely, the incidence of renal dysfunction decreased from 36.2% to 28.8%. Meanwhile, there were decreasing uses of hemodialysis (from 37.3% to 28.7%) and vasopressors (from 58.3% to 47.9%). Hospital mortality also decreased from 42.6% to 31.2% during the 10 years. After the patient and hospital characteristics were adjusted, patients admitted in 2007 and 2008 were 50% less likely to die than those admitted in 1999 and 2000 (adjusted odds ratio 0.5, 95% confidence interval 0.38–0.67). This study demonstrates a temporal improvement of the short-term survival of the ICU patients with SLE in Taiwan despite changing characteristics and increasing severity of the acute critical illnesses.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease of unknown cause, featuring episodic flares and thrombophilic and immuno-compromised states,1–3 which can predispose patients to multi-organ damage and serious infection requiring intensive care. 4 The five-year survival rate of SLE patients has increased from 50% in the 1950s to over 90% in the 2000s. 5 The improved survival is achieved at the costs of immunosuppression and accrual of organ damage, which has led to changing morbidity and mortality of these patients.6,7 Whether similar trends are also present in critically ill SLE patients remains poorly understood. In the last two decades, more than a dozen studies have investigated the characteristics and outcome of critically ill patients with SLE8–12 or with systemic rheumatic diseases that included SLE.13–20 The short-term mortality rates in these studies varied widely, ranging from 20% to 53%.13–20 These studies are limited by experiences from a single or a few institutions and by the inclusion of only a few patients, which is prone to selection bias.
In the present study, we retrieved inpatient data of adult SLE patients having an intensive care unit (ICU) stay from a national administrative database, 21 used in several studies on SLE22–29 and some critical illnesses.30–32 We aimed to investigate temporal trends in characteristics and outcome of these patients over a 10-year period. We hypothesized that there is a temporal improvement in the outcome of ICU patients with SLE.
Methods
Database
Data in this retrospective population-based cross-sectional study were retrieved from a national administrative database. In Taiwan, a compulsory and universal National Health Insurance (NHI) program has been implemented by the government since 1995. There are two major ethnic groups in Taiwan, namely Han Chinese (98%) and Taiwanese aborigines (2%). During the study period, the per capita income in Taiwan increased from US$13,609 (USD) in 1999 to US$17,399 in 2008. Patients in this study were drawn from the National Health Insurance Research Database (NHIRD), 21 released for research purposes by the National Health Research Institute (NHRI), Taipei, Taiwan. The NHIRD provides information on inpatient and outpatient claims of nearly all the population (>22 million) and has been used in relevant studies on SLE22–29 and some critical illnesses.30–32 The NHIRD information includes encrypted patient identification numbers, sex, birthday, dates of admission and discharge, medical institutions providing the services, the ICD-9-CM (International Classification of Diseases, Ninth Revision, Clinical Modification) diagnosis codes (up to five) and procedure codes (up to five), outcome at hospital discharge (recovered, died or transferred), and hospital charges.
Ethics statement
The review board of the Medical Research Committee in Chi Mei Medical Center approved the study (grant No. CMFHR10081) and waived the need for formal ethical approval and written informed consent from the participants due to the use of a reimbursement database. Researchers using the database must sign an agreement based on the Computer-Processed Personal Data Protection Law and related regulations of the Bureau of NHI and the NHRI.
Study sample and definitions
SLE was defined by ICD-9-CM code 710.0. Patients with SLE were initially identified from a catastrophic illness registry, which includes selected major injuries or illnesses (including rheumatic diseases) and is published by the Department of Health, Executive Yuan. To register as SLE, the diagnosis must be made by board-certified rheumatologists and the application is further reviewed and approved by the Bureau of NHI, which ensures the accuracy and reliability of the diagnosis. 27 The study period spanned from 1999 through 2008 (both inclusive). We then linked patients with SLE in the registry to inpatient claims data and identified 14,668 patients with hospitalization; among them, 2994 (20.4%) had at least one ICU admission during the study period. After excluding patients less than 15 years old, the rest (n = 2870) were enrolled in the analysis. To ensure the independence of observations, only the first ICU admission during the study period was analyzed. The definitions of infection, acute organ dysfunction and hospital mortality were described previously. 32
Measurements
Measurements of the study subjects included age, sex, year of admission, hospital levels (medical center [>500 beds], regional [250–500 beds] and district hospitals [20–249 beds]), disease duration (measured by the time period from SLE diagnosis to the first ICU admission), major surgical condition (defined by the use of spinal, epidural or general anesthesia), Charlson Comorbidity Index,33,34 selected comorbid conditions, principal diagnoses, infection, acute organ dysfunction, corticosteroid and immunosuppressive therapy for SLE, uses of life-support measures (including hemodialysis, vasopressors, and mechanical ventilation [MV]), lengths of ICU and hospital stay, and hospital mortality. Hospitals are periodically accredited by the Taiwan Joint Commission on Hospital Accreditation and Quality Improvement (authorized by the government) and classified into the three levels, representing different hospital sizes and service capabilities. The Charlson index, adapted for use with ICD-9-CM coded administrative databases, is a weighted summary measure of clinically important concomitant diseases including rheumatic disease.33,34 For the purpose of this study, rheumatic disease or SLE was excluded from the Charlson index.
Statistics
Continuous variables are presented as median (interquartile range) owing to a skewed distribution; discrete ones as counts or percentages. To investigate temporal trends, analysis of variance was performed for linearity of scaled variables, and linear-by-linear association chi-square analysis was performed for categorical data. To assess the effect of calendar year on hospital mortality, we performed univariable and multivariable logistic regression models with generalized estimating equations methods, 35 which was used to account for hospital clustering effect 36 and was done by specifying an exchangeable structure of a working correlation matrix. Covariates in the model included age (<65 vs. ≥65 years), sex, disease duration (<1, 1–3, >3 years), non-SLE comorbidity (y/n), major surgical condition (y/n), rheumatic vs. non-rheumatic principal diagnosis, infection (y/n), acute organ dysfunction (y/n), and hospital level. As we simultaneously included a number of covariates in the multivariable regression model, a potential numerical problem concerned collinearity between covariates, rendering estimated regression coefficients invalid. We assessed this potential problem by examining the estimated slope coefficients and standard errors of the mean, and found no indication of collinearity. Model performance was assessed using c-statistics. Data analyses were performed using SPSS for Windows, version 17.0 (SPSS Inc., Illinois, US). Statistical significance was set at p < .05 (two-tailed).
Results
Demographics and clinical characteristics
Characteristics of the intensive care unit (ICU) patients with systemic lupus erythematosus (SLE) by subperiod
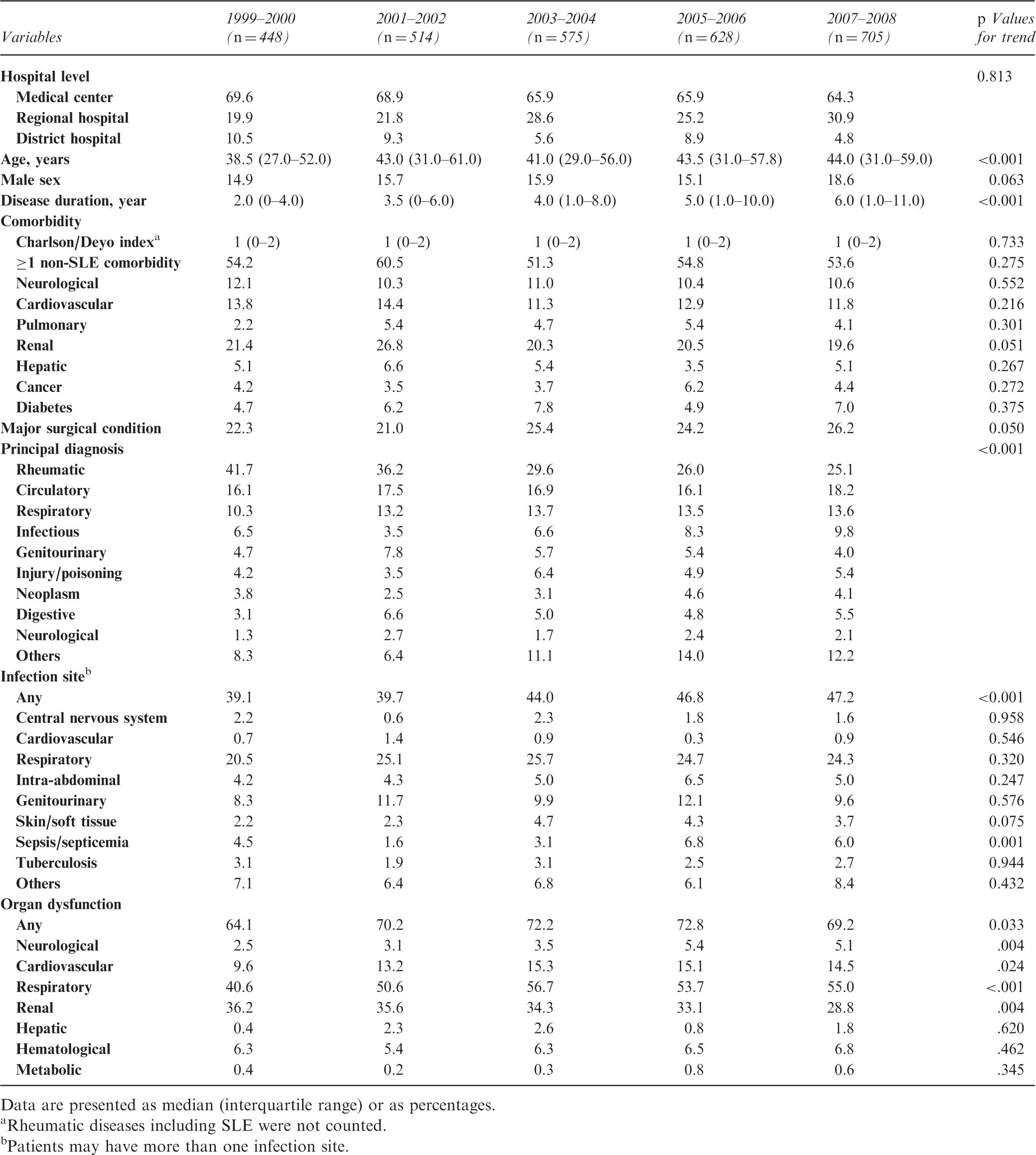
Data are presented as median (interquartile range) or as percentages.
Rheumatic diseases including SLE were not counted.
Patients may have more than one infection site.
Comorbidity other than SLE was common (overall 54.7%); the percentage varied insignificantly over time. The most common comorbid conditions were renal (overall 21.5%), cardiovascular (12.7%) and neurological diseases (10.8%). Approximately one-fourth of the patients had a major surgical condition; and the percentage slightly increased in recent years. The proportion of patients with a principal diagnosis of rheumatic disease (mainly SLE) fell significantly from 41.7% to 25.1%. Nevertheless, the most common principal diagnosis was still rheumatic disease, which was followed by circulatory and respiratory diagnoses. The incidence of infection increased gradually from 39.1% to 47.2%; however, the increase was significant only in sepsis/septicemia when individual infection sites were examined separately. The severity of patient conditions was increasing, as reflected by the high and increasing incidence of organ dysfunction, which increased from 64.1% in 1999 and 2000 to 69.2% in 2007 and 2008. The increase of organ dysfunction was mainly seen in neurological (from 2.5% to 5.1%), cardiovascular (from 9.6% to 14.5%), and respiratory systems (from 40.6% to 55.0%). Conversely, the incidence of renal dysfunction decreased from 36.2% to 28.8% during the same period.
Treatment, resource use and outcome
Treatment and resource use of the intensive care unit (ICU) patients with systemic lupus erythematosus by subperiod
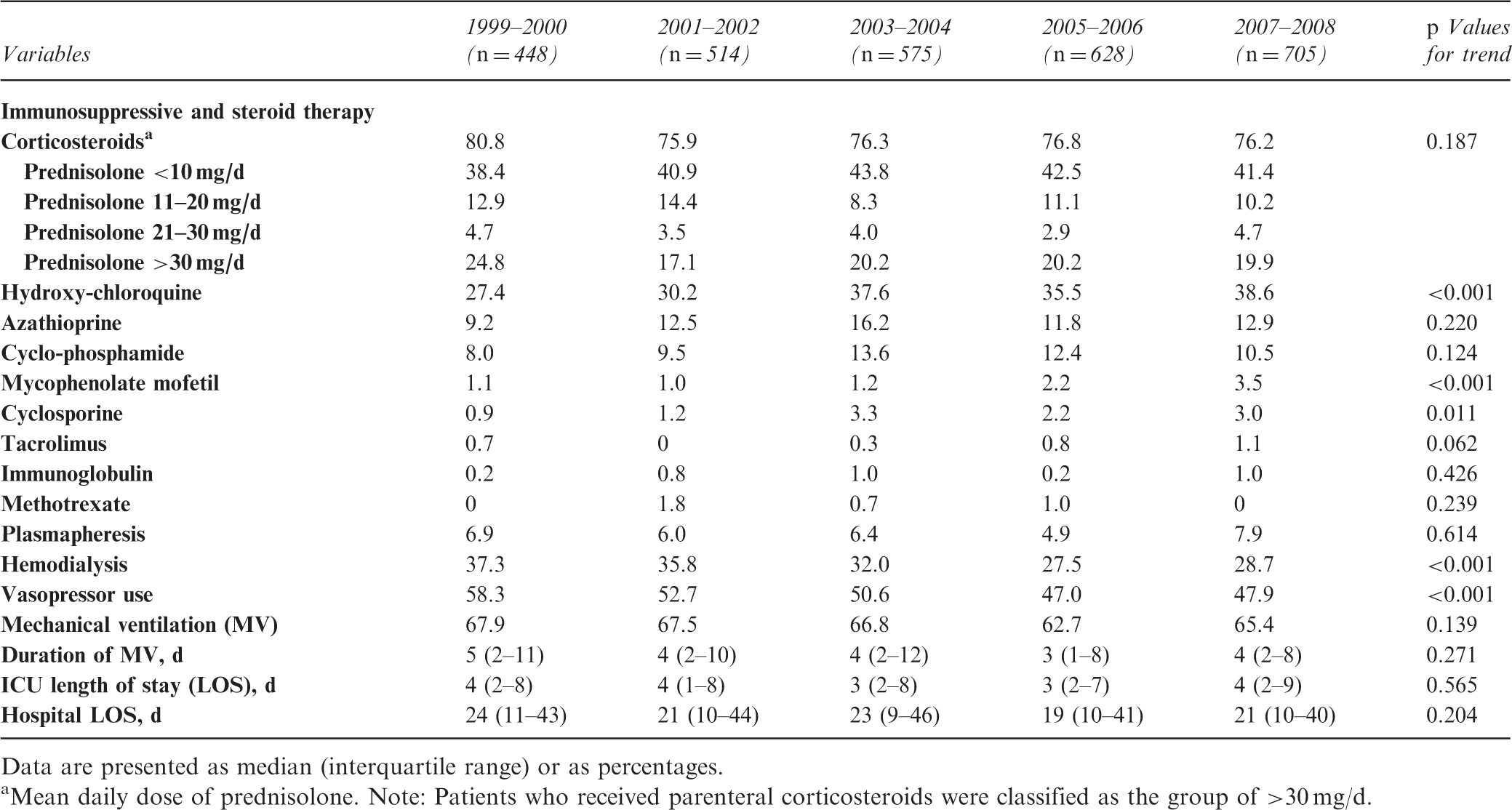
Data are presented as median (interquartile range) or as percentages.
Mean daily dose of prednisolone. Note: Patients who received parenteral corticosteroids were classified as the group of >30 mg/d.
Predictors of hospital mortality in the intensive care unit patients with systemic lupus erythematosus (SLE)
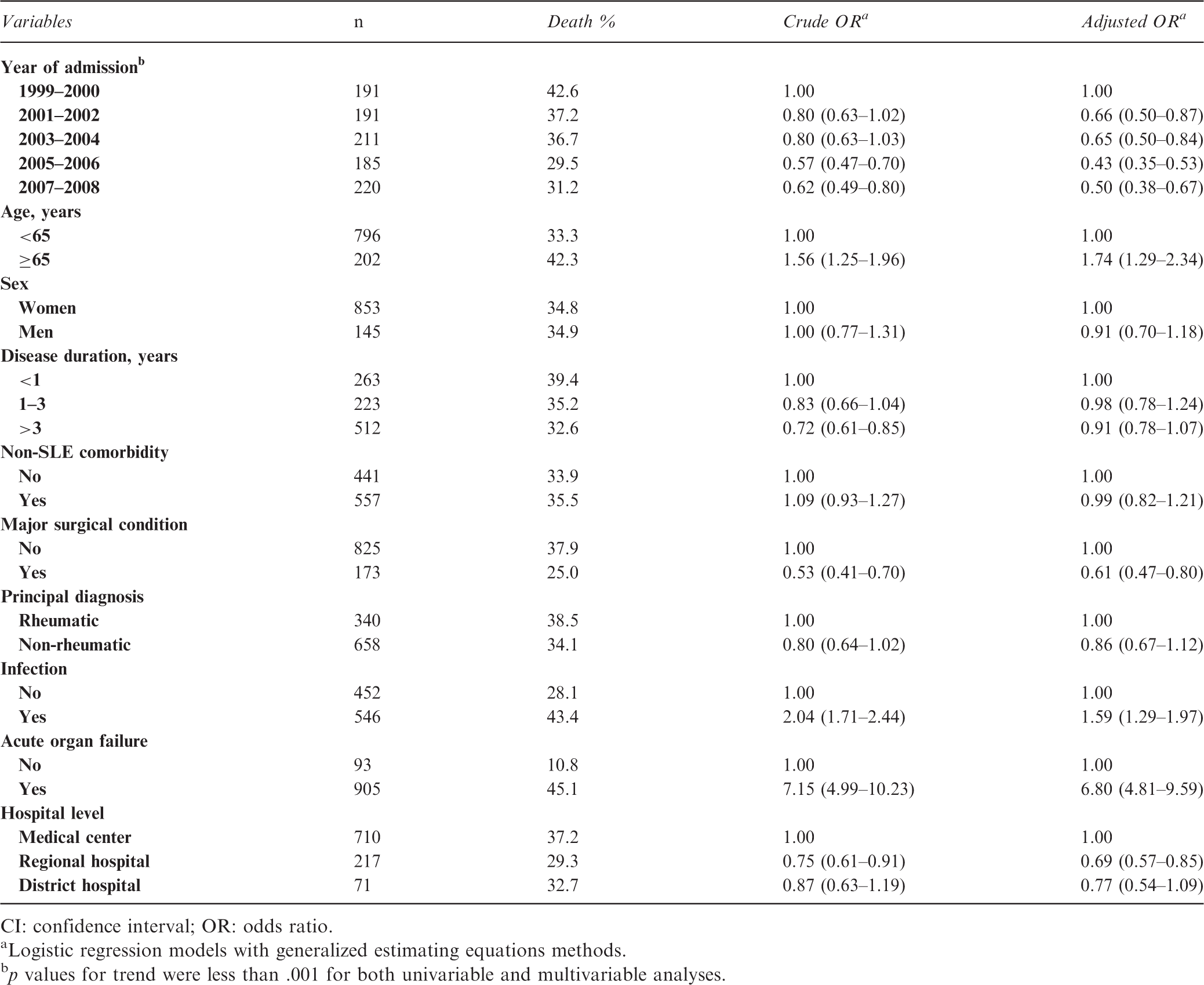
CI: confidence interval; OR: odds ratio.
Logistic regression models with generalized estimating equations methods.
p values for trend were less than .001 for both univariable and multivariable analyses.
Discussion
In this study, we found that ICU patients with SLE in Taiwan were getting older, were increasingly admitted later after SLE diagnosis and more commonly for non-rheumatic disease, and had more overall incidence of infection and organ dysfunction over the recent 10 years. Conversely, the incidence of renal dysfunction and the percentages of patients receiving hemodialysis and vasopressors decreased over time. More importantly, the risk of death was halved during the study period when changes in the patient and hospital characteristics were adjusted.
The characteristics of the ICU patients with SLE are expected to change over time because of an improving survival of SLE patients over the decades. The five-year survival rate of SLE patients increases from 50% in the 1950s to over 90% in the 2000s. 5 To the best of our knowledge, this is the first and largest population-based study that enrolled ICU patients with SLE and showed the temporal change of the patient characteristics and the short-term mortality over a long period of time. Unlike previous reports on ICU patients with SLE,8–20 our study is strengthened by its generalizability through an unbiased selection of all treated patients in Taiwan. Most of the previous studies are done earlier (spanned from 1978 to 2000), enroll fewer (usually less than 30) patients from single institutions, combine with other rheumatic diseases, or do not provide separate analyses of SLE.13–18,20 Nevertheless, these studies, taken together, can provide some useful information. For example, these reports reveal a trend of an increasing age of ICU patients with SLE over time (from average 27 years in earlier reports8–11 to 32 years in recent ones),12,19 which is consistent with our results. Furthermore, we found that patients were admitted to the ICU increasingly later after diagnosis of SLE and more commonly for non-rheumatic reasons. These findings likely reflect an improved treatment and survival of SLE patients over the years.5,37
The previous largest study on ICU patients with SLE is reported by Ñamendys-Silva and coworkers in 2009. 12 They investigated 104 SLE patients, with a mean age of 32 years and mean disease duration of 70 months, in a single ICU in Mexico from 1994 to 2004. 12 Among these patients, 96.2% were women, 61.5% had infection, 46.2% had acute renal dysfunction, 54.2% received hemodialysis, 67.3% received vasopressors/inotropics, and 74% received MV. 12 They found an overall ICU mortality rate of 32.7%; which was significantly lower in the later years than in the first few years (24.2% in 2000–2004 vs. 47.6% in 1994–1999). 12 The corresponding figures in our study were mean (median) age of 42 (44) years, mean (median) disease duration of 56 (50) months, women 85.5% (overall), infection 43.9%, acute renal dysfunction 33.2%, hemodialysis 31.7%, vasopressors 50.7%, MV 65.9%, and hospital mortality 34.8%, respectively. Among studies enrolling fewer ICU patients with SLE, the ICU mortality rates varied more widely.8–11,19 The variation in mortality among these studies is likely due to differences in time periods, patient populations, and study designs.
The occurrence of acute organ dysfunction is the strongest predictor of death in the ICU patients with SLE (aOR 6.80, see Table 3), which is not unexpected because organ dysfunction is usually an intermediate pathway leading to death. 32 Findings on the temporal change of organ dysfunction may also provide further evidence for the changing pattern of morbidity and mortality found in patients with SLE.6,7 Previous studies on all patients with SLE have shown that deaths due to active SLE, lupus nephritis, and infection are decreasing, whereas deaths due to thrombosis and circulatory diseases are increasing.6,7 The decreasing incidence of renal dysfunction and increasing incidence of cardiovascular dysfunction found in the present study agree with previous observations in all patients with SLE.6,7 However, the increasing incidence of infection and neurological dysfunction in our ICU patients with SLE somewhat differs from these previous observations.6,7 Moreover, we also found an increasing incidence of acute respiratory dysfunction in the ICU patients with SLE. Because only 20% of the Taiwanese patients with SLE had an ICU stay during the study period, the characteristics of these patients may significantly differ from those of without an ICU stay. Further research is needed to find these differences and factors that may be associated with ICU admission.
Treatment of SLE is changing, 37 as was also found in the ICU patients. The finding of increasing prescriptions of non-steroid medications, especially hydroxychloroquine (an antimalarial drug), for the ICU patients with SLE is consistent with a previous longitudinal study on patients with newly diagnosed SLE in Canada. 37 However, hydroxychloroquine was less frequently prescribed for patients in our study than for those in the Canadian Study (<40% vs. 46% in the 2000s). 37 One study has reported even more frequent use of hydroxychloroquine, especially in SLE patients managed by rheumatologists (88%). 38 The less frequent use of this medication in our study cohort may be due to different patient characteristics, physician specialties, and/or discontinuity of care during ICU stay. When patients are admitted to the ICU, discontinuity of care is likely to occur because both open and closed ICU systems exist in Taiwan. Hydroxychloroquine has been advocated as the cornerstone of SLE treatment due to its good safety profile and numerous beneficial effects.39,40 Treatment of the ICU patients with SLE may be further improved by education and/or through a multidisciplinary team approach.38,41
Reasons for the observed mortality decline in the critically ill patients with SLE cannot be determined in this study. However, it is likely that the mortality decline was somewhat attributed to increased use of early, effective lupus medication such as mycophenolate mofetil and hydroxychloroquine along with reduced side effects from lower doses of corticosteroids for SLE patients. Another reason for the mortality decline is likely attributed to the general improvement of critical care because the decline persisted after changes in patient and hospital characteristics were adjusted and there are still no treatment guidelines specific for these patients. Beginning in the early 2000s, there has been an increasing worldwide application of some important concepts of critical care, such as improving patient safety through quality improvement initiatives and implementing care bundles or protocols through evidence-based medicine. These approaches may help reduce adverse events and provide early and effective treatment for critically ill patients with SLE, leading to the improved outcome.
Three poor prognostic factors (i.e., older age, infection, and organ dysfunction) found in the present study may potentially hamper the temporal improvement of the short-term survival in the ICU patients with SLE. Improved treatment of SLE reduces and postpones the occurrence of acute critical illnesses, as was shown in our study: the median time from SLE diagnosis to ICU admission had increased by four years during the 10-year study period. However, the improved survival is achieved at the costs of immunosuppression and accrual of organ damage.42,43 Moreover, the increasing patient age and incidence of infection and organ dysfunction in the ICU patients with SLE will pose greater challenges to caring physicians in the future.
Comorbidity, measured by the Charlson Comorbidity Index, is associated with a decreased long-term survival in SLE patients, 44 independent of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index. 43 In the present study, non-SLE comorbidity was not associated with the short-term survival in the multivariable model. Because acute organ dysfunction is closer to death than comorbidity, we speculated that the inclusion of acute organ dysfunction in the model may attenuate the effect of comorbidity on mortality. When acute organ dysfunction was excluded from the model, we confirmed the speculation and found that non-SLE comorbidity was associated with increased risk of hospital mortality (aOR 1.21, 95% CI 1.02–1.44).
Several limitations deserve comments. First, the status of anticardiolipin antibodies, the disease activities of SLE, the renal status related to lupus activity and the acute severity and organ dysfunction scores of the critical illnesses were not available in the database. Despite these, we provided data on patients with chronic renal disease and acute renal dysfunction as well as those undergoing hemodialysis. Information on acute organ dysfunction shown in Table 1 may also provide a surrogate measure of the severity of the acute illnesses. Second, the disease duration is likely underestimated because the onset of SLE usually predates the registry as a catastrophic illness in the database. Third, the prevalence of some comorbidities and the incidence of infection and organ dysfunction may be underestimated due to the limited diagnosis space in the database. Fourth, we did not measure the use of antibiotics for the patients because the information is complex and the issue is not the primary purpose of this study. Further research on this topic is needed. Finally, hospital mortality may also be underestimated because of inability to verify through death certificate. Despite these limitations, using the same ICD-9-CM codes over the study period would retain the internal validity of the temporal trend analyses.
In conclusion, the characteristics and outcomes of the ICU patients with SLE are changing over time. The short-term survival of these patients is improving in Taiwan despite an increasing severity of the acute critical illnesses.
Footnotes
Acknowledgements
The study was based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
Funding
The study was performed in Chi Mei Medical Center and supported by grant CMFHR10081 from the hospital. The funding source had no role in the design, execution, analysis and interpretation of data, or writing of the study.
Conflict of interest
None declared.