
Abstract
Posterior reversible encephalopathy syndrome (PRES) is an uncommon neurologic condition associated with systemic lupus erythematosus (SLE). This study aimed to demonstrate the risk factors and clinical outcome of PRES in patients with SLE.
Fifteen patients with SLE were diagnosed with PRES by characteristic clinical manifestations and magnetic resonance imaging (MRI) features from 2000 to 2012. Clinical profiles and outcomes were assessed for this study population. Additionally, 48 SLE patients with neurologic symptoms who underwent brain MRI were included for comparative analyses.
The median age and duration of SLE in patients with PRES was 27 and 6.1 years, respectively. Comparison between patients with and without PRES revealed significant differences in the presentation of hypertension and seizure, lupus nephritis with renal insufficiency, treatment with high-dose steroid and cyclophosphamide, recent transfusion, and lupus activity measured by SLE disease activity index. Renal failure was the single independent factor with a high odds ratio of 129.250 by multivariate analysis. Of 15 patients, four experienced relapse and two died of sepsis during hospitalization.
Our results suggest that lupus nephritis with renal dysfunction and other related clinical conditions can precede the occurrence of PRES in patients with SLE. It is important to perform early brain imaging for a timely diagnosis of PRES when clinically suspected.
Keywords
Introduction
Posterior reversible encephalopathy syndrome (PRES), also known as reversible posterior leukoencephalopathy syndrome, is a clinico-radiological syndrome characterized by brain imaging that includes vasogenic edema and clinical symptoms of hypertension, headache, and seizure. Since Hinchey and colleagues categorized this syndrome in 1996, 1 the number of cases has been increasing with the advent of neuroimaging techniques and clinicians’ awareness of PRES. Previous studies have suggested that PRES develops in association with hypertension, renal disease, autoimmune disorders, and treatment with cytotoxic drugs.1–4
Systemic lupus erythematosus (SLE) is one of the predisposing conditions related to PRES, particularly when accompanied by lupus nephritis.4–9 However, SLE is an uncommon autoimmune disease in which the occurrence of PRES is even rarer. This rarity makes it difficult to clarify the clinical course of PRES in patients with SLE, and there are some inconsistencies between the studies performed with case reports. Furthermore, it is challenging to distinguish PRES from other neuropsychiatric manifestations of SLE,10,11 since SLE patients can present various neurologic manifestations encompassing neuropsychiatric lupus and other neurologic complications due to metabolic or infectious causes.
Clinical suspicion and early neuroimaging are required for a timely diagnosis because management of PRES, which is mainly supportive, differs from immunosuppressive therapy or other specific treatment for neuropsychiatric complications of SLE. The present study aimed to elucidate the clinical features predicting the development of PRES and to demonstrate the clinical course of PRES.
Methods
Patients and controls
We retrospectively reviewed the medical records of patients with SLE who were admitted to Seoul St. Mary’s Hospital, tertiary care university hospital and referral center, between January 2000 and December 2012. Of the 740 patients who fulfilled the 1997 updated version for classification of SLE,12,13 15 with PRES were identified. PRES was diagnosed using a multidisciplinary approach based on clinical symptoms and typical brain imaging. Forty-eight age- and sex-matched control subjects were recruited from SLE patients with neuropsychiatric problem other than PRES. Diagnoses in the control group were systematically determined by the clinical course, and laboratory and radiological tests. The control group was composed of 19 patients with neuropsychiatric lupus, 10 with cerebral infection, four with migraine, two with benign intracranial hypertension, two with seizure disorder, two with fibromyalgia, two with headache secondary to upper respiratory infection, and seven with other causes. The study population was entirely Korean.
All included patients underwent brain magnetic resonance imaging (MRI) to evaluate neurologic symptoms including seizure and/or headache. This study protocol was approved by the Institutional Review Board of Seoul St. Mary’s Hospital.
Clinical and laboratory profiles
The following conditions were assessed for the 15 patients with PRES: demographic characteristics such as age, sex, and disease duration, clinical features, laboratory profiles, current treatment for SLE, management and clinical outcomes of PRES. Of laboratory tests, anti-double-stranded DNA (anti-dsDNA) antibody was measured using enzyme-linked immunosorbent assay (ELISA) (anti-dsDNA ELISA kit, GENESIS, Leicester, UK), and anti-DNA antibody was determined by the Farr assay. Lupus disease activity was evaluated with the SLE Disease Activity Index (SLEDAI). 14 Additionally, modified SLEDAI, excluding neuropsychiatric manifestations, was calculated, as PRES frequently accompanies neurologic symptoms. Clinical and laboratory profiles were compared between patients with and without PRES to assess risk factors for PRES.
Statistical analysis
Differences in continuous variables between the patients with and without PRES were analyzed by the Mann Whitney U test. Fisher’s exact test was used to compare categorical data. We performed multivariate logistic regression using forward stepwise selection to determine the independent risk factors for PRES. Variables with p ≤ 0.10 in a univariate analysis were included in a multivariate analysis. A p value < 0.05 was considered statistically significant. All data were analyzed using SAS 9.1 software (SAS Institute, Inc, Cary, NC, USA).
Results
Patient characteristics
Clinical characteristics of 15 SLE patients with PRES
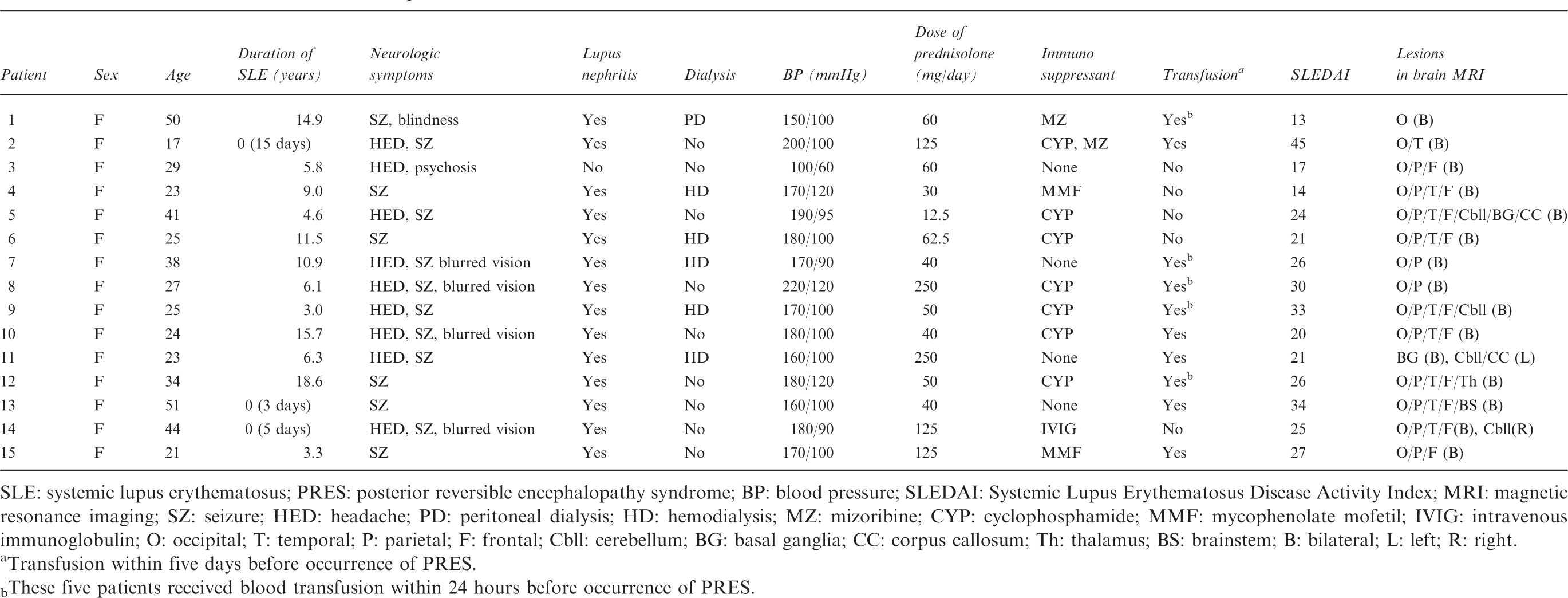
SLE: systemic lupus erythematosus; PRES: posterior reversible encephalopathy syndrome; BP: blood pressure; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; MRI: magnetic resonance imaging; SZ: seizure; HED: headache; PD: peritoneal dialysis; HD: hemodialysis; MZ: mizoribine; CYP: cyclophosphamide; MMF: mycophenolate mofetil; IVIG: intravenous immunoglobulin; O: occipital; T: temporal; P: parietal; F: frontal; Cbll: cerebellum; BG: basal ganglia; CC: corpus callosum; Th: thalamus; BS: brainstem; B: bilateral; L: left; R: right.
Transfusion within five days before occurrence of PRES.
These five patients received blood transfusion within 24 hours before occurrence of PRES.
Laboratory profiles of 15 SLE patients with PRES
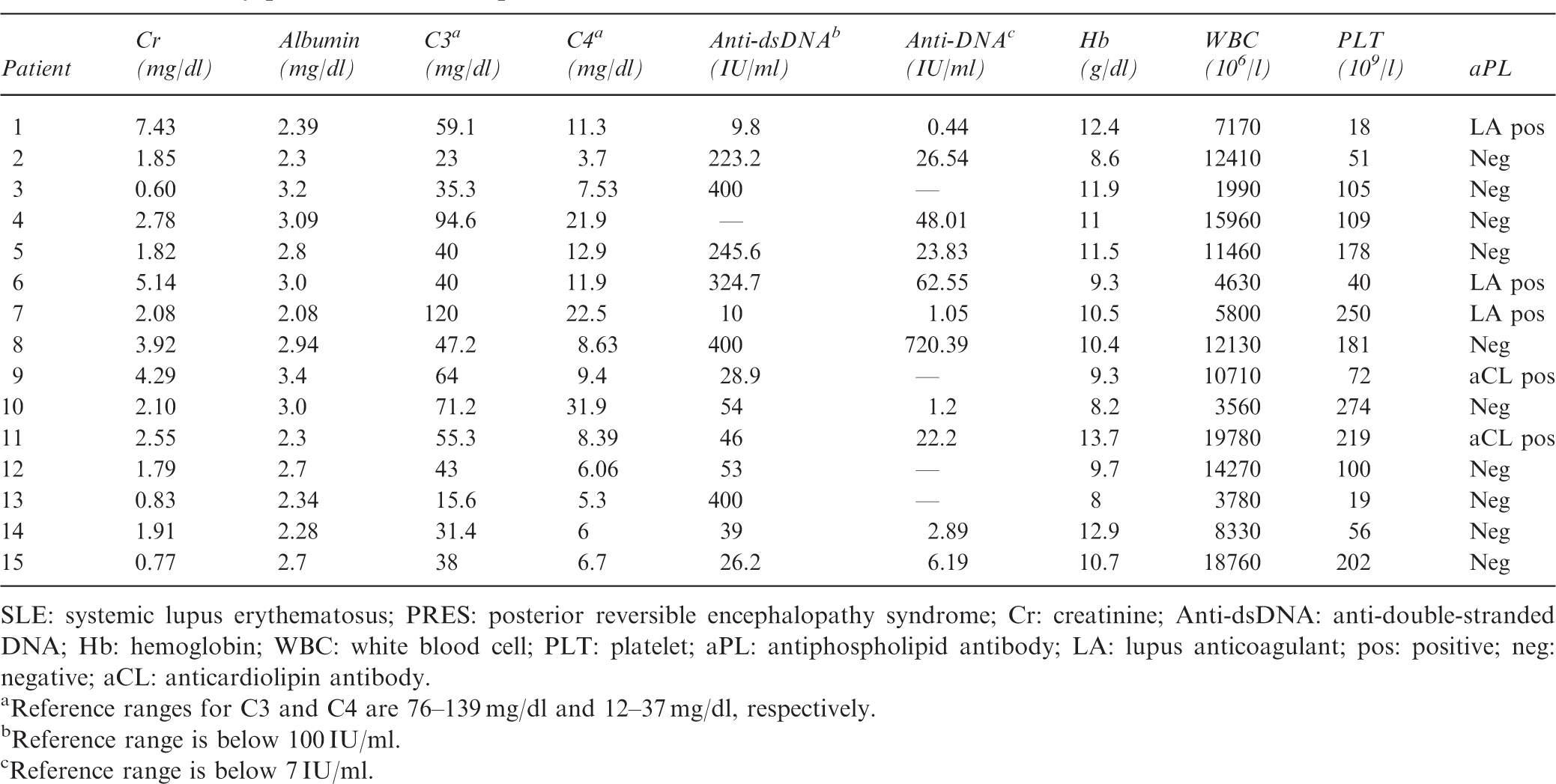
SLE: systemic lupus erythematosus; PRES: posterior reversible encephalopathy syndrome; Cr: creatinine; Anti-dsDNA: anti-double-stranded DNA; Hb: hemoglobin; WBC: white blood cell; PLT: platelet; aPL: antiphospholipid antibody; LA: lupus anticoagulant; pos: positive; neg: negative; aCL: anticardiolipin antibody.
Reference ranges for C3 and C4 are 76–139 mg/dl and 12–37 mg/dl, respectively.
Reference range is below 100 IU/ml.
Reference range is below 7 IU/ml.
Risk factors for PRES
Comparison of SLE patients with or without PRES
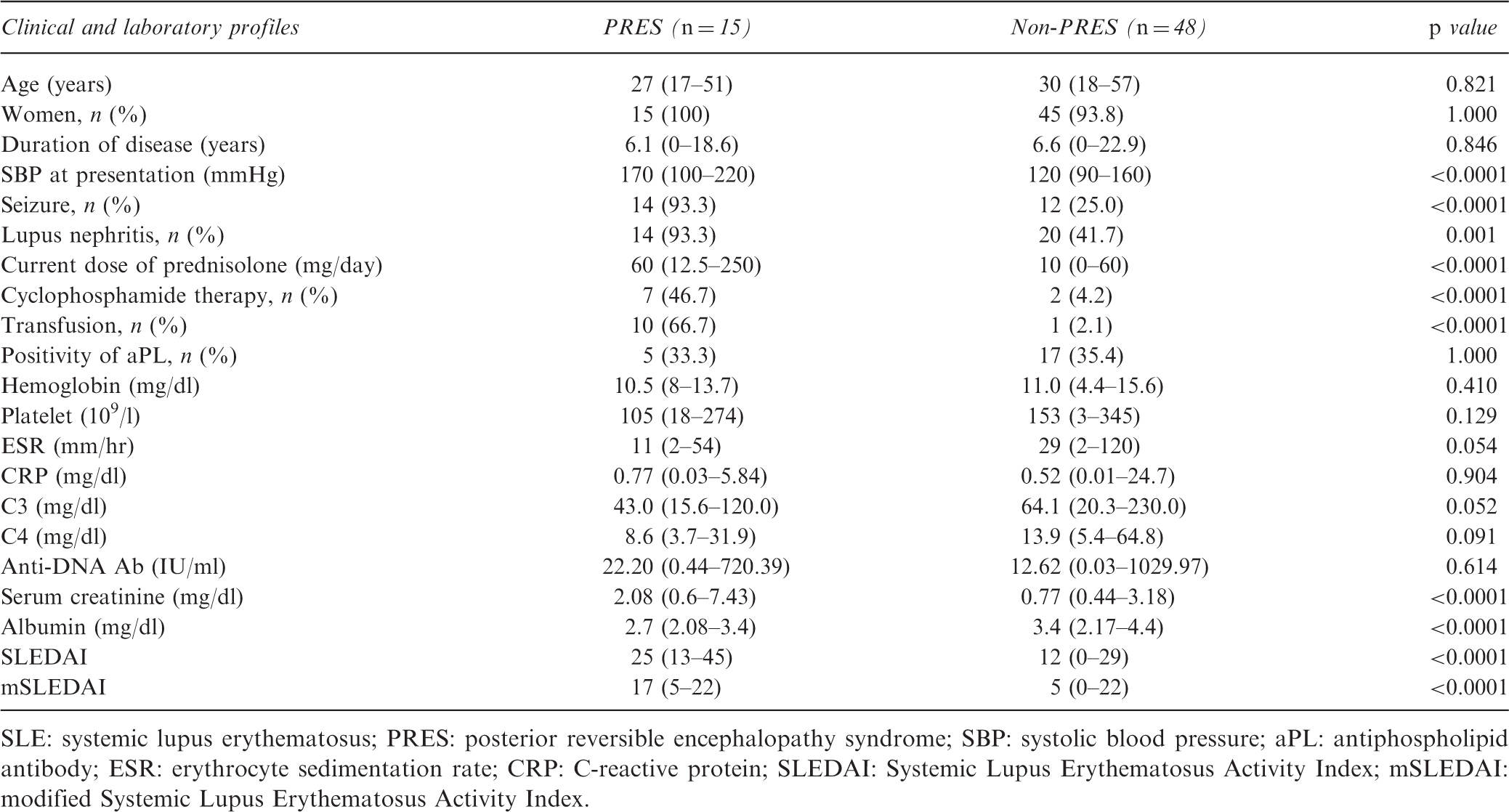
SLE: systemic lupus erythematosus; PRES: posterior reversible encephalopathy syndrome; SBP: systolic blood pressure; aPL: antiphospholipid antibody; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; SLEDAI: Systemic Lupus Erythematosus Activity Index; mSLEDAI: modified Systemic Lupus Erythematosus Activity Index.
Factors preceding the diagnosis of PRES
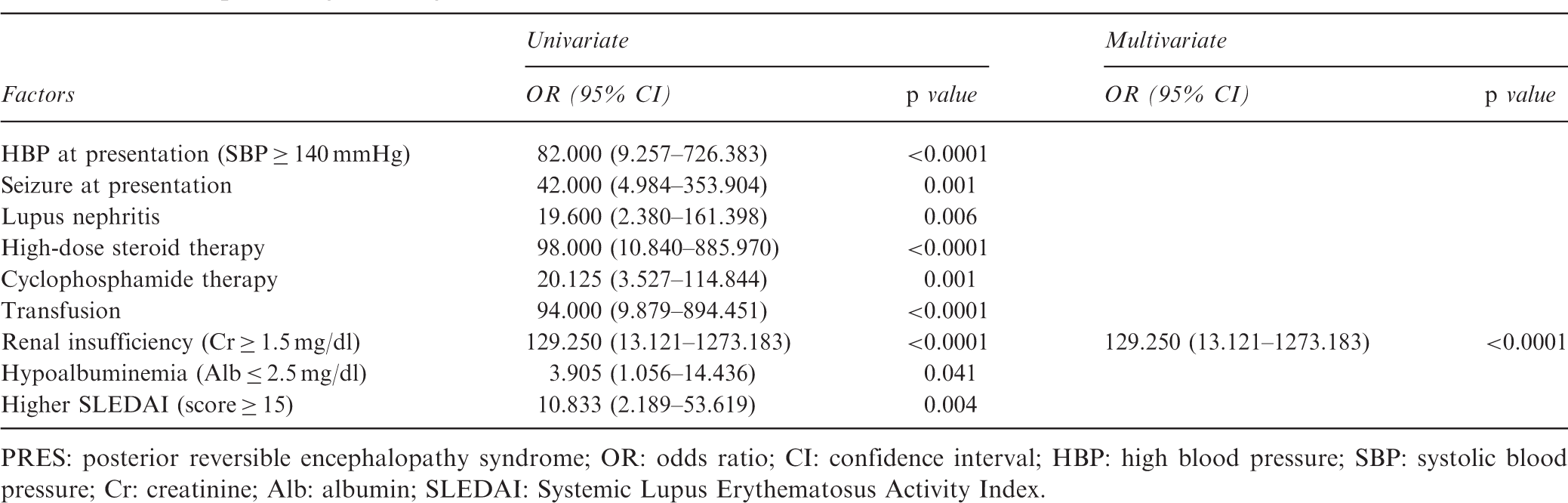
PRES: posterior reversible encephalopathy syndrome; OR: odds ratio; CI: confidence interval; HBP: high blood pressure; SBP: systolic blood pressure; Cr: creatinine; Alb: albumin; SLEDAI: Systemic Lupus Erythematosus Activity Index.
Treatment and clinical outcomes
Treatments and clinical outcomes of 15 SLE patients with PRES
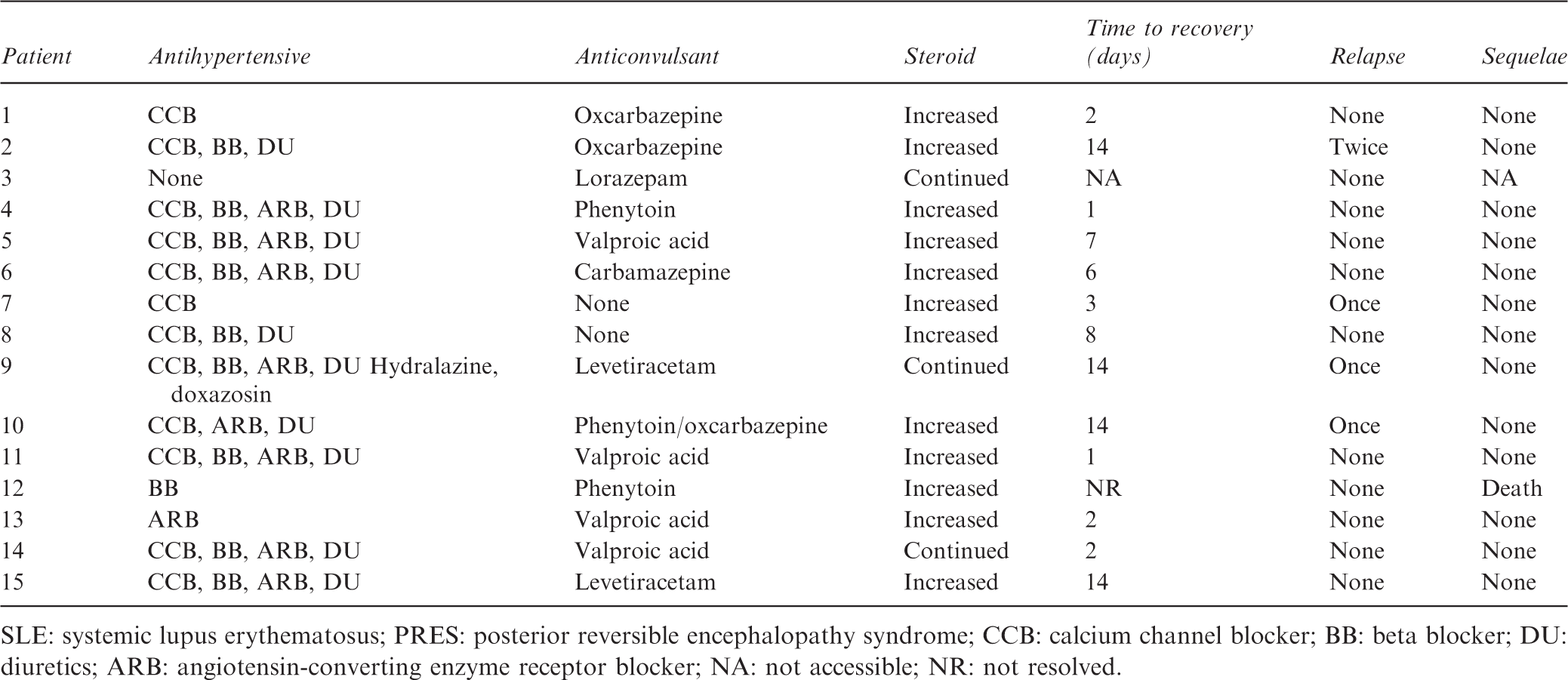
SLE: systemic lupus erythematosus; PRES: posterior reversible encephalopathy syndrome; CCB: calcium channel blocker; BB: beta blocker; DU: diuretics; ARB: angiotensin-converting enzyme receptor blocker; NA: not accessible; NR: not resolved.
Four patients experienced relapse of seizures, and one (Patient 12) did not recover from PRES. Patient 12 remained unconscious after onset of PRES until death. The resolution of PRES was not established in Patient 3 who had been diagnosed previously with bipolar disorder, because psychosis, one of the presenting manifestations, continued thereafter. Two patients (Patients 1 and 12) died of sepsis during hospitalization.
Discussion
The advance of neuroimaging techniques and the accumulation of case reports have enabled a further understanding of PRES during the last decade. However, PRES in association with lupus is still uncommon to characterize the clinical features distinct from other neuropsychiatric manifestations of SLE.
The present study shows similarity to prior studies in terms of the clinical manifestations and the preceding features of PRES. As described in earlier cases, most of our patients complained of headache and visual disturbance, and presented with suddenly increasing blood pressure and seizure. Lupus nephritis with renal dysfunction, hypoalbuminemia, treatment with high-dose steroid, and cyclophosphamide therapy were predisposing conditions for PRES as reported previously.6,7,9,10,15
The clinical features that appeared significant for the development of PRES are closely interrelated. As expected, the renal function of patients with lupus nephritis deteriorated, and high-dose steroid and/or cyclophosphamide were used to manage the nephritis. Therefore, we evaluated the independent factors for the development of PRES in patients by using a multivariate analysis. As a result, renal failure, as defined by elevated creatinine, was the only significant factor in our study. The association between renal insufficiency and PRES has been described extensively.1,2,16–19 The pathogenic mechanism of PRES is considered to be vasogenic edema caused by hypertension with autonomic dysregulation and disruption of the blood-brain barrier. 1,11,20 Considering the increased incidence of fluid retention and resulting elevated blood pressure in patients with renal failure, hypertension would be one of the common pathways. High-dose steroid therapy and blood transfusions also lead to volume expansion, accounting for one of the preceding factors for PRES.
Despite the close connection with hypertension, several reports are available regarding development of PRES in SLE patients with normal blood pressure.21,22 In our series, Patient 3 was normotensive. We concluded that the neurologic manifestation of Patient 3 was PRES by typical MRI findings, although the clinical features were distinct from the other patients. A case of PRES without hypertension suggests that the vasogenic edema can be derived from endothelial injury. SLE is a systemic autoimmune disease in which organ damage is mediated by autoantibody production and immune complex formation. The blood-brain barrier can be damaged by immune-mediated attack in patients with SLE.13,23 Four patients in our series were suspected to have vasculitis of the central nervous system when brain MRIs were reviewed. This presumption is supported by higher lupus activity measured by the SLEDAI score in the PRES group. In addition, four of 13 patients, excluding two patients who had not recovered from PRES (30.8%), experienced a recurrent attack of PRES despite supportive care. For a similar reason, there is an opinion that although immunosuppressive therapy is predisposed to PRES, immunosuppressive agents are required to reverse PRES after failure of symptomatic treatment. 8 The association of PRES with autoimmune disease is quite apparent, but the relevant pathophysiology remains to be explained. Thus further investigation is required to explore the mechanism of how lupus affects the development of PRES.
Some dissimilarities with the prior studies were observed in our cases. Several reports have suggested an association between aPL and PRES,15,24 but we found no statistical difference in aPL positivity between patients with and without PRES. Our patients with PRES were relatively older than earlier cases in which PRES developed in mostly adolescent or young adults <40 years.7,9,25
Some limitations of our study should be mentioned. First, the clinical records of the patients were collected retrospectively. The treatment for PRES was not standardized, and a follow-up MRI was not possible in most patients. Thus, the impact of therapeutic modalities could not be evaluated, and the resolution of PRES was only determined clinically but not confirmed radiologically. Second, this study had defects stemming from its small sample size. Considering the low incidence of PRES in patients with SLE, a multicenter study would overcome this weakness. Nevertheless, the present study is composed of a relatively large number of patients with SLE and PRES, and to our knowledge, this is the only case-control study on the development of PRES.
In summary, PRES with underlying SLE is being increasingly encountered. Some preceding clinical features of PRES were apparent when lupus patients presented with neuropsychiatric manifestations. Our results indicate that lupus nephritis, particularly when accompanied by renal dysfunction, is one of the most significant risk factors for PRES. As an early diagnosis of PRES is essential for proper management involving control of blood pressure, it is important to be aware of PRES and to perform brain imaging when this syndrome is clinically suspected.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors have no conflicts of interest to declare.