
Abstract
Systemic lupus erythematosus (SLE) predominantly affects women of childbearing age, but 15–20% of cases are diagnosed during childhood. It is important for physicians to understand the epidemiology and clinical presentation for early detection and diagnosis of this disease in difference races. The aim of this retrospective review was to provide a 20-year experience for initial clinical and laboratory manifestations and outcomes in pediatric-onset SLE (pSLE) in a medical center in Asia. We reviewed medical records between April 1990 and June 2012 of patients with a diagnosis of International Classification of Diseases, Ninth Revision (ICD-9) code 710.0 (SLE), who admitted or received follow-up in the Department of Pediatrics at Chang Chung Memorial Hospital. Patients with a diagnosis of SLE prior to their 18th birthday and followed up at our hospital were eligible for inclusion in this study. Medical records regarding age, gender, date of birth and diagnosis, clinical manifestations at diagnosis, laboratory results, image studies and the classification criteria were reviewed. Patients received regular outpatient department follow-up and laboratory survey every 1–6 months. The study cohort consisted of 189 patients; 164 females (86.87%) and 25 males (13.23%). The overall mean age at pSLE diagnosis was 12.62 ± 2.77 years. The most common clinical symptom was malar rash, followed by arthritis and oral ulcers. There was no significant difference in clinical and laboratory manifestations between females and males. More than half of the patients presented with renal involvement initially. The most common histological finding was Class IV lupus nephritis (LN), especially in males (p = 0.034) and young age. Even with severe LN, the rate of end-stage renal disease (ESRD) was low if adequate treatment was initiated. The 5, 10 and 15-year ESRD-free survival rates were 95.4%, 94.0% and 89.9% in patients with biopsy-proven LN. However, infection was the leading cause of mortality. Therefore, aggressive treatment for major organ involvement is important, but physicians must also be aware of fatal infection. The overall survival rates were 5 years: 93.4% and 10–20 years: 89.6%.
Keywords
Introduction
Systemic lupus erythematosus (SLE), a chronic inflammatory and multi-system autoimmune disease, is characterized by the presence of autoantibodies and multi-organ system involvement, including skin, joints, the kidney, and the pulmonary and central nervous system, resulting in diverse clinical presentations. Notably, SLE should be considered whenever patients present with multi-organ system disease. 1 Although it predominantly affects women of childbearing age, 15–20% of patients are diagnosed during childhood, with disease onset prior to the age of 16. 2 Clinical presentation ranges from a mild disease characterized by a rash and arthritis to life-threatening disease. Renal, neuropsychiatric and cardiopulmonary disease is seen commonly in pediatric-onset SLE (pSLE). 3 Furthermore, SLE symptoms may be affected by environmental factors and differ among racial groups and ethnic groups. Recent studies have suggested that pSLE is more frequent and severe in non-White populations, especially Black, Asian, Hispanic and Aboriginal populations. 4 Understanding the epidemiology and clinical presentation of pSLE is important for physicians for early detection and diagnosis in subjects of different races. This retrospective study reviews 20 years of experience for initial clinical and laboratory manifestations and outcomes in pSLE at an Asian medical center.
Patients and methods
Study design
This study reviewed the medical records of those admitted or who received follow-up between April 1990 and June 2012 at Chang Chung Memorial Hospital, Taiwan. All patients were diagnosed using the International Classification of Diseases, Ninth Revision (ICD-9) code 710.0 (SLE).
Participants
Chang Gung Memorial Hospital, located in northern Taiwan, is a tertiary medical center. Patients diagnosed with SLE before their 18th birthday and followed at this hospital were eligible for inclusion. Once patients were diagnosed with pSLE, they and their families were invited to participate in this longitudinal observational study. Standardized treatment was applied according to published guidelines. Laboratory studies, including urine and blood, were obtained according to clinical need. For those patients who underwent blood or urine sampling, samples were preserved for further investigations. All patients and their families signed the informed consent forms, and research ethics approval was obtained (IRB99-06378).
Patients without medical records about initial presentation and diagnostic criteria were excluded. Patients with mixed connective tissue disease were also excluded. All enrolled patients met at least four of the 11 American College of Rheumatology Revised Criteria. 5 Patients underwent regular outpatient department and laboratory assessment every 1–3 months, according to their clinical condition and disease activity.
Variables
Subject age, gender, date of birth, diagnosis, clinical manifestations at diagnosis, laboratory results, imaging study results and classification criteria were reviewed in detail.
Standardized tests results for complete blood count and autoantibodies including antinuclear antibody (ANA), anti-double strand DNA (dsDNA), anti-SSA, anti-SSB, anti-Smith, anti-RNP, and anti-phospholipid antibodies (anti-cardiolipin, beta-2 glycoprotein and lupus anti-coagulant) were analyzed if available.
In patients who presented with overt proteinuria, hematuria, or impaired renal function, a renal biopsy was performed at initial diagnosis or during the follow-up period. Renal pathology was reviewed by an experienced pathologist and classified according to World Health Organization classification, which was revised in 1982. For those patients who underwent renal biopsy at other hospitals, a pathology report was documented and pathology slide was reviewed if needed. Once lupus nephritis (LN) was confirmed by renal pathology, standardized treatment was initiated. In accordance with previous study results from the National Institutes of Health,6,7 patients with proliferative nephritis were treated with pulse cyclophosphamide (CYC). The treatment regimen was pulse CYC monthly for the first 6 months and then every 3 months in the following 18 months. The total course comprised 12 pulse CYC treatments over 24 months. The CYC first dose was 0.5 g/m2, followed by 0.75 and 1.0 g/m2 for the 2nd and 3rd treatment, respectively. Thereafter, the treatment dose was 1.0 g/m2. For patients who could not tolerate the side effects of CYC (including nausea/vomiting and leukopenia) or who had poor treatment response (continuing proteinuria or hematuria), mycophenolate mofetil was prescribed after a discussion with the patient and their family.
Since age, especially puberty, may alter the incidence and presentation of SLE, all enrolled patients were divided into three age groups based on when the diagnosis was made: <8 years (preschool age); 8 to less than 12 years (school age); and 12–18 years (adolescents). We assume most children enter puberty between the ages of 8 and 12 years.
Statistical analyses
Statistical analysis was performed by SPSS17.0. Characteristics were presented as n (%) for categorical data, and Chi-square test or Fisher’s exact test was used to test correlation in gender and age. A two-proportion Z-test was applied to compare proportion in gender. The survival curve plot was based on the Kaplan–Meier method with the log rank test. Statistical significance was determined based on p < 0.05.
Results
The study cohort consisted of 189 patients, of which 164 were female (86.87%) and 25 were male (13.23%). All children were ethnic Taiwanese. The female to male ratio was 6.56:1. Overall mean age at pSLE diagnosis was 12.62 ± 2.77 years. Mean age at diagnosis was 12.92 ± 2.77 years (range, 3.92–17.25 years) for females and 11.96 ± 2.68 (range, 5.75–16.58 years) for males. Mean disease follow-up duration was 6.94 ± 4.63 years (range, 0.01–22.24 years).
The clinical presentation and laboratory result of enrolled pSLE patients
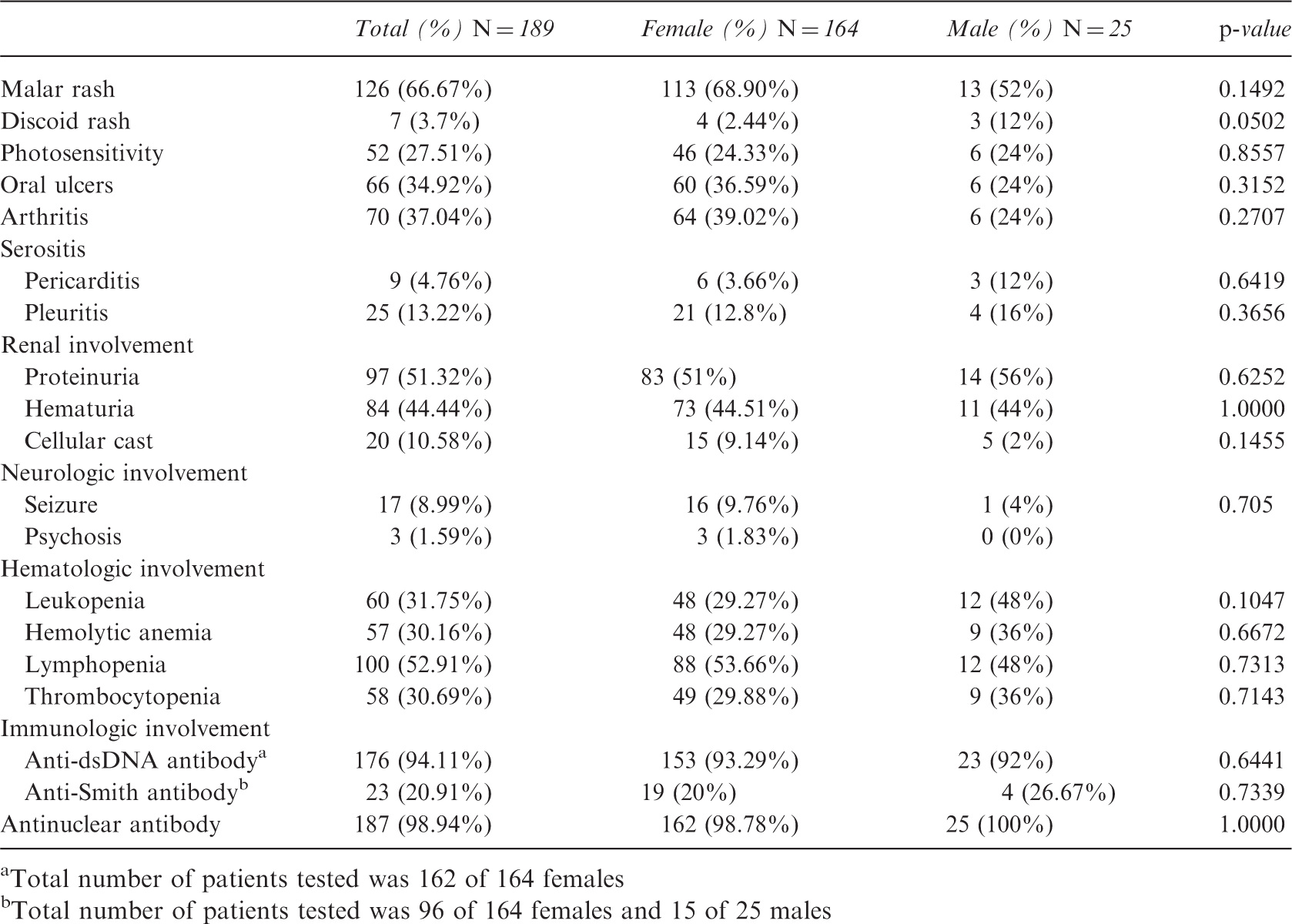
Total number of patients tested was 162 of 164 females
Total number of patients tested was 96 of 164 females and 15 of 25 males
Antinuclear antibody was the autoantibody detected most frequently; its positive rate was 100% (n = 25) for males and 98.78% (n = 162) for females. Only two female patients were diagnosed with pSLE without ANA positivity. One female patient, aged 14 years 5 months, had malar rash, photosensitivity, biopsy-proven Class IV LN, lymphopenia and was anti-dsDNA positive. The other female, aged 15 years 9 months had malar rash, oral ulcer, photosensitivity, leukopenia, lymphopenia and was anti-dsDNA positive.
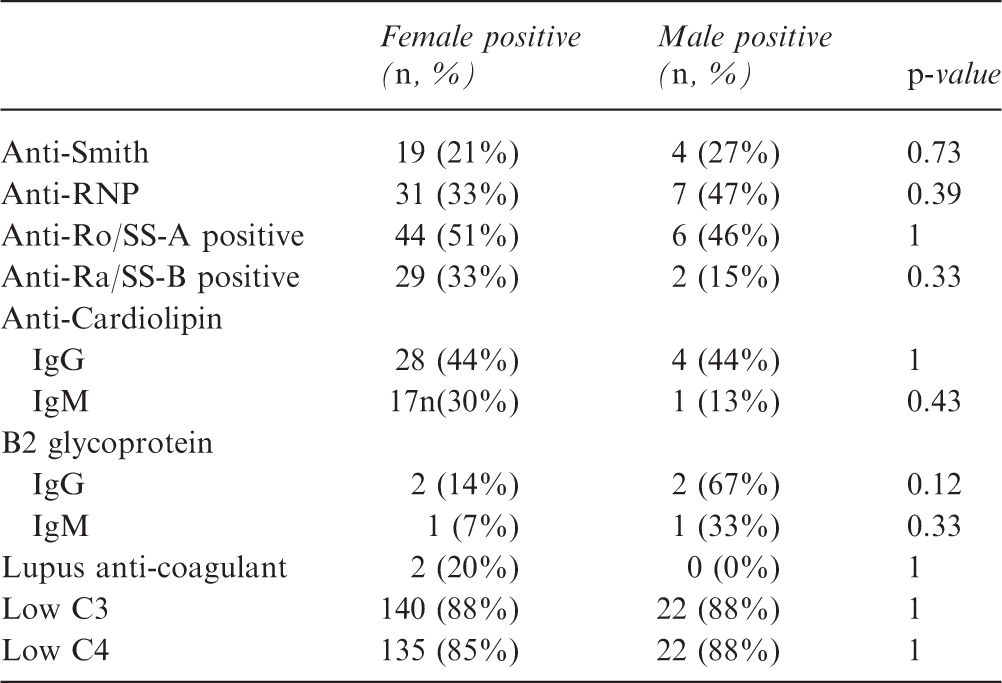
Positivity for autoantibody and hypocomplementemia
The clinical presentation and laboratory result in different age groups
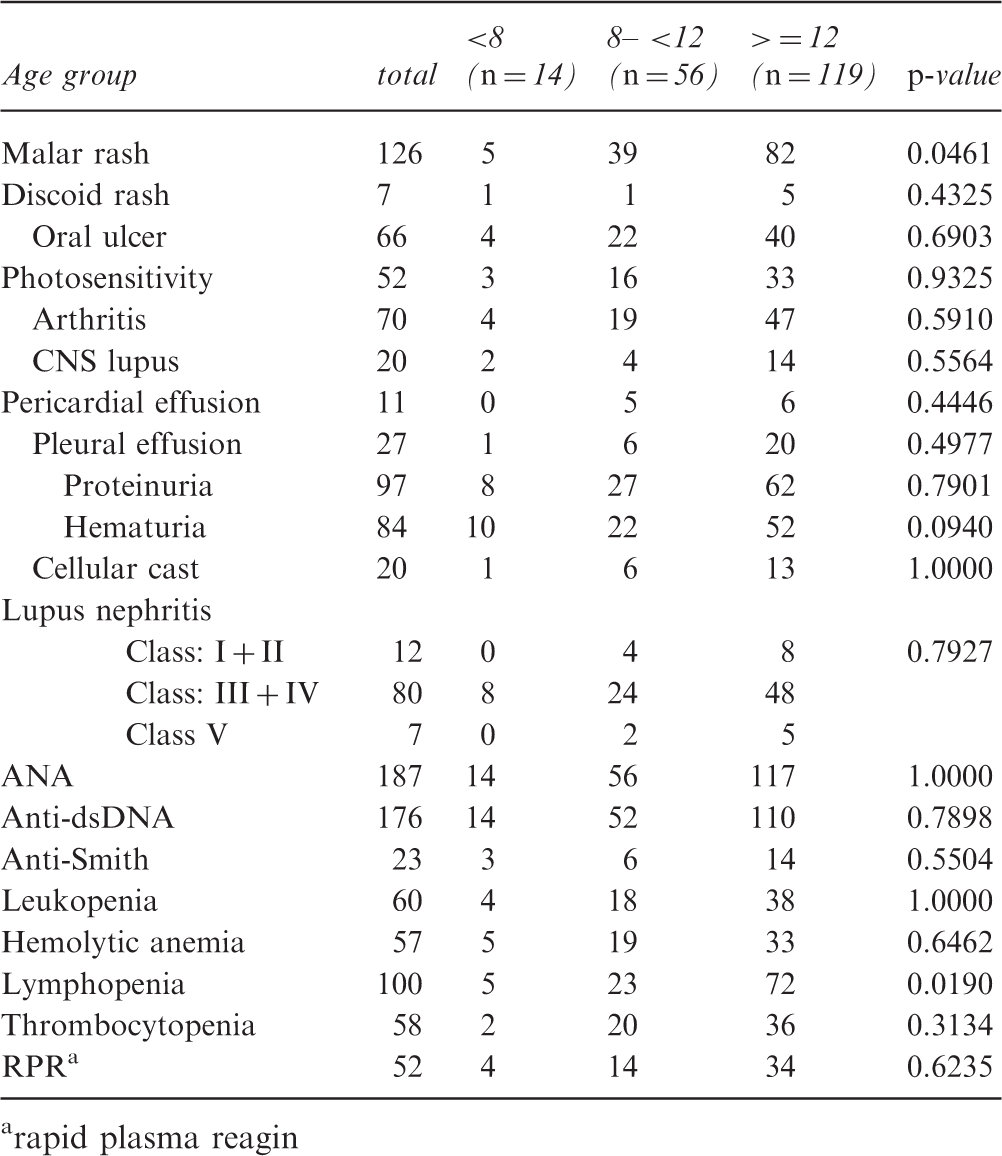
rapid plasma reagin
Classification of lupus nephritis
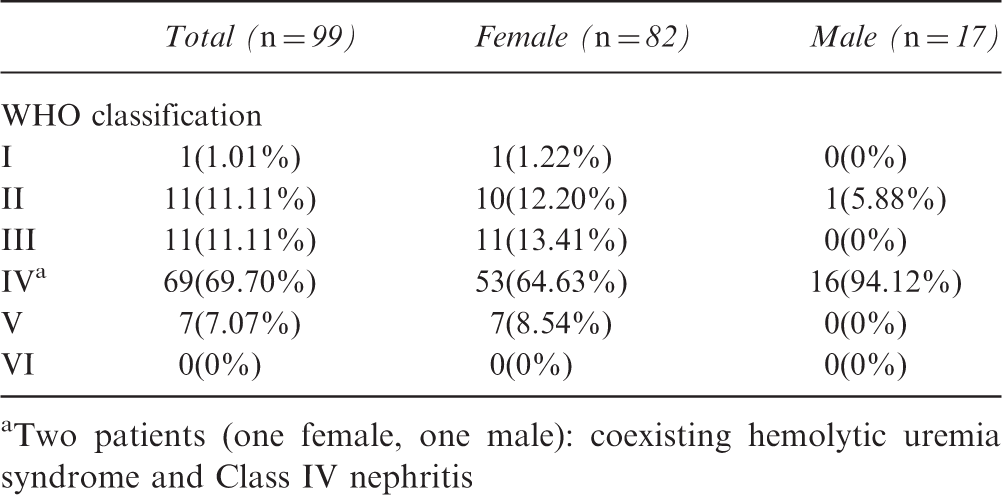
Two patients (one female, one male): coexisting hemolytic uremia syndrome and Class IV nephritis
Of all patients, seven (six female and one male) were progressing to end-stage renal disease (ESRD) and received regular dialysis. Of those seven patients with ESRD, six (85.7%) patients underwent renal biopsy. Histological findings showed Class IV nephritis in four patients. Two patients had Class III nephritis initially and then Class IV nephritis in the subsequent biopsy due to renal function deterioration. Renal biopsy was not performed in one patient because of her critical condition, and she received dialysis soon after follow-up. Kidney survival estimation was performed. The 5-, 10- and 15-year ESRD-free survival rates were 95.4%, 94.0% and 89.9%, respectively, in patients with biopsy-proven LN. The kidney survival rate was 93.1% at 5 years, 90.9% at 10 years and 83.9% at 15 years for patients with Class IV nephritis.
Fifteen patients expired. Eight died of infection, three died of cardiovascular accidents (two cerebral infarctions and one cerebral hemorrhage), one died of type B aortic dissection, and one died of necrotizing pancreatitis. Two patients died in other hospitals; the accurate cause of death was not fully investigated. Only three expired without LN development. One patient, who had proteinuria without biopsy proof, died of Staphylococcus aureus sepsis soon after diagnosis of pSLE; another died of Escherichia coli sepsis and pulmonary hemorrhage 5 days after diagnosis of pSLE; and another, who had congenital chromosome anomaly, was only 3 years 11 months at diagnosis and died as a 10-year-old from pneumonia. However, no significant difference existed between patients with LN and without LN for mortality. Kaplan–Meier survival analysis was applied (Figure 1). The overall 5-year survival rate was 93.4%, and 89.6% for 10–20 years. The patients were placed into two groups: those with and without LN. Patients with LN had a worse 5-year survival rate than those without LN (84.6% vs. 97.4%), and a worse 10–20-year survival rate (80.6% vs. 97.4%). No significant difference existed in survival rates between patients with LN and without LN (p = 0.127).
Kaplan–Meier survival estimation in all pSLE patients.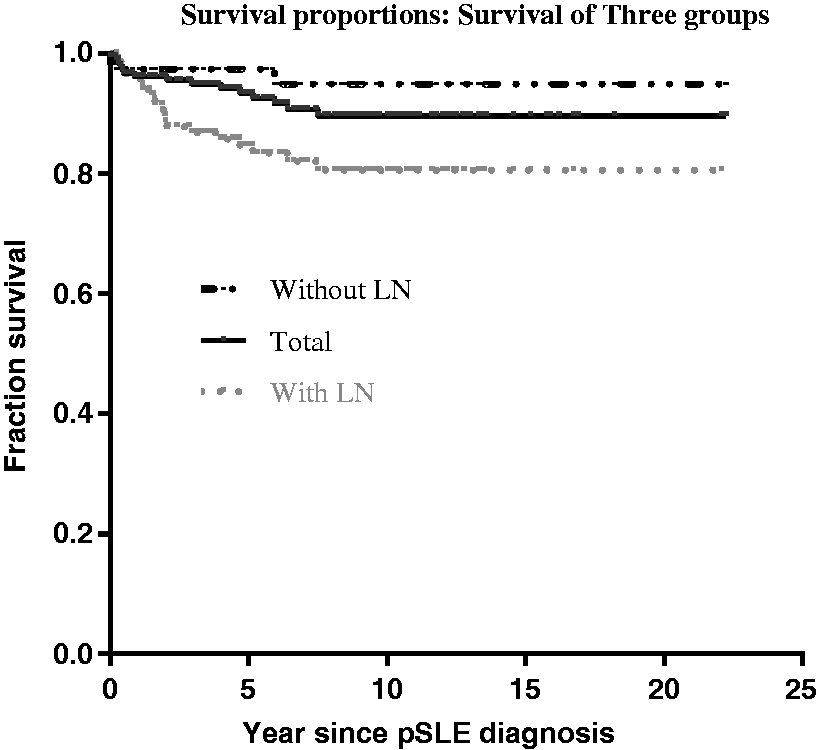
Discussion
Oral ulcers, malar rash and photosensitivity were more common in females, but no significant difference existed in their incidence between females and males. Only discoid rash was more common in males. Overall, clinical presentation did not differ by gender in this study. Clinical presentation, however, differs among races. For example, Aboriginals and Blacks were found to have a lower frequency of malar rash, Asians had a lower frequency of arthritis, and serositis was more common in Aboriginals and Blacks in a Canadian cohort. 4 Arthritis was more commonly observed in school-age and adolescent patients compared with preschool age; 8 however, the findings obtained by this study differed.
Renal disease was found to be more common for Asian and Black patients. 4 The occurrence of nephritis in pSLE in Asian countries varies greatly at 29–81%. 9 The most common histopathology of LN in Asian children was Class IV nephritis, which occurred in 39.4–54%. 9 According to a 2010 literature review, Class IV nephritis was a dominant histological finding in males. 10 Males also had a higher risk of renal failure than females. 10 For this cohort, more than half of the patients (51.32%) had renal involvement. Renal involvement was also common in pSLE in other cohorts and its incidences were similar: 47% at onset in a UK study 11 , 56% at disease onset prior to the 12th birthday and 47% in patients aged at least 12 years old in the USA, 12 and 55% in Canada. 13 In total, 112 patients had a renal biopsy at time of diagnosis or follow-up period. Class IV nephritis was the most common histopathological presentation, accounting for 69.7% of subjects in this cohort. As in Asia, Class IV nephritis was also the most common nephritis in other countries – 38% in the USA 14 and 46% in Canada. 13 Although Class IV nephritis is common worldwide, compatible with previous results Class IV nephritis was relatively more common in Asia.
Eight (six female and two male) patients (57.1%) of preschool age at diagnosis underwent renal biopsy; all were diagnosed with Class IV nephritis.
By gender, males had a significantly higher incidence of Class IV nephritis than females (p = 0.034). Males and females had a similar occurrence of renal involvement. When it existed, LN was most severe in males or in the preschool age group, which was confirmed by renal histological findings.
The occurrence of ESRD was similar in both genders, in contrast to a previous study which found that males had higher risk for renal failure. 10 However, the number of patients with renal failure in this cohort was relatively small. Class IV nephritis at presentation was most highly predictive of progression to ESRD 15 in a previous study. The same result was obtained by this meta-analysis. All patients had or were developing Class IV nephritis before ESRD, except for one patient who did not have renal biopsy before dialysis.
After intravenous CYC was introduced to treat proliferative LN, renal survival improved worldwide. Before intravenous CYC treatment, kidney survival in all LN patients was only 44.4% at 5 years and 29% at 10 years after initial LN diagnosis. 15 Kidney survival for children and young adults with proliferative LN improved to 77% at 5 years 16 after the introduction of intravenous CYC treatment. Intravenous CYC treatment was initiated at Chang Gung Memorial Hospital after a series of reports was published. In this study, all enrolled patients with proliferative LN received intravenous CYC treatment. Kidney survival for patients with proliferative LN was as high as 89.9% at 15 years for this cohort.
Previously, most studies have only reported the short-term survival rates for renal function and death. Bogdanović et al. 17 reported a 5-year kidney survival rate of 88.6% for all patients and 82.4% in the Class IV nephritis group. In Thailand, the 5-year kidney survival rate from time of diagnosis to the endpoints of terminal renal failure was 94% for the whole group, and 91% in Class IV nephritis group. 18 A recent UK national pSLE cohort study, which enrolled 232 patients, with follow-up of over 4.5 years was published in 2012. Only one (0.5%) patient had ESRD and one (0.5%) patient had a reduced estimated glomerular filtration rate less than 50%. 11 However, histopathological results were not reported for that cohort. Moreover, follow-up duration was less than 5 years. In a longer follow-up duration, overall kidney survival rate was 79% at 15 years in Thailand 19 and 81.7% at 15 years in Hong Kong. 20 For Class IV nephritis, survival rates without ESRD at 5, 10 and 15 years were 91.5%, 82.3% and 76%, respectively, in Hong Kong. 20 The cohort enrollment start time in this study was the same as that in Hong Kong; 20 however, the survival rate without ESRD at 5, 10 and 15 years was better at 93.1%, 90.9% and 83.9% in patients with Class IV nephritis. This study reported a large Chinese cohort with a detailed pathological review and follow-up period of over 20 years.
In this cohort, more than half of the patients who expired died of infection. A similar result was obtained in a prospective study of adult SLE in Hong Kong. 21 Although intravenous CYC treatment has markedly improved renal function preservation and survival, CYC treatment may also cause fatal infection, especially for patients on a concomitant high dose of prednisolone. 22 Therefore, for patients with severe organ damage, clinical physicians should carefully weigh the benefit and harm of using a glucocorticoid and immunosuppressant, because infection was the most frequent cause of mortality.
This study has several limitations. Most importantly, this was a prospective cohort with retrospective review. Several constitutional symptoms were common in pSLE including fever, edema, and lymphadenopathy. Because this was a retrospective review, symptoms, apart from diagnostic criteria, were not well documented. To avoid underestimation, this study did not analyze common constitutional symptoms, and disease activities were not assessed. Nomenclature for neuropsychiatric lupus syndromes was not well defined until 1999 23 ; hence, we did not analyze those symptoms. Last, all patients were ethnic Taiwanese and most lived in northern Taiwan, such that the results of the analysis may only reflect a small population. Nevertheless, the results were comparable with those obtained by other studies, particularly those of Asian populations.
In summary, the occurrence of pSLE was higher for females without a distinctive clinical or laboratory presentation. Renal involvement was common in pSLE. Class IV nephritis was the most common histopathological result, especially in males and the preschool age group. Although active disease and acute illness were associated with pSLE, the survival rate was good. Even with severe LN, the rate of ESRD was low when adequate treatment was initiated. Infection was the leading cause of mortality. Therefore, aggressive treatment for major organ involvement is important, and the physician must be aware of fatal infection.
Footnotes
Funding
This study was supported by Chang Gung Medical Research Progress Grant (IRB 99-06379B) and National Science Council Grant (CMRPG400041).
Conflict of interests
None declared.
Acknowledgements
We would like to thank all of the patients and their families for participating in this cohort study. We also appreciate all the efforts made by Huang et al. in disease diagnosis and treatment. Ted Knoy is thanked for his editorial assistance.