
Abstract
In this report we discuss a case of a patient with systemic lupus erythematosus who developed herpes simplex virus type 1(HSV-1) infection presenting with encephalitis as well as necrotic and non-necrotic retinitis. The patient presented with typical clinical symptoms and radiologic abnormalities consistent with HSV-1 encephalitis and HSV-1 retinitis in patients with HIV infection, but lacked cerebrospinal fluid pleocytosis and had bilateral retinitis with poor visual acuity. To the best of our knowledge, this is the first such case reported in the literature.
Keywords
Introduction
Neuropsychiatric (NP) symptoms are reported in 10–80% of patients with systemic lupus erythematosus (SLE). These symptoms can be due either to SLE-related conditions (e.g. vasculopathy, antibody) or to non-SLE-related conditions (e.g. infections associated with immunosuppressive therapy, metabolic complications of organ failure, hypertension, toxic effects of corticosteroid therapy). In general, the latter set of conditions is the more common cause of NP symptoms. When a patient presents with NP symptoms, it is vital to successfully differentiate between non-SLE-related conditions, such as central nervous system (CNS) infections, and neuropsychiatric lupus (NPSLE), because the inability to distinguish them can lead to severe complications and patient mortality.
Herpes simplex virus type 1 (HSV-1) encephalitis is a rare condition in patients with SLE. Here, we present the case of a patient with SLE, who had HSV-1 encephalitis, necrotic retinitis, and non-necrotic retinitis, and who was initially misdiagnosed with NPSLE.
Case report
A 42-year-old woman was referred to the emergency department in April 2012 with a 2-day history of fever and 1-day history of irrelevant speech and disorientation without any sign of antecedent virus infection. The patient had been diagnosed with SLE in June 2011. She presented with nephrotic syndrome, dysmorphic hematuria, hypertension, leucopenia, and was positive for antinuclear antibodies (ANA), anti-double-strand DNA antibodies (anti-dsDNA), and anti-SSA antibody, with a low complement count. A renal biopsy revealed class IV + V lupus nephritis. She was treated continuously with 40 mg of methylprednisolone (MP) once a day and 750 mg of mycophenolate mofetil (MMF) twice a day for 3 months. The patient’s lupus nephritis resolved, but she developed herpes zoster in her left calf, and hence, corticosteroid and MMF dosages had been tapered. At the time of admission, she was taking 18 mg of oral MP once a day and 500 mg of MMF twice a day.
Upon examination, we found that the patient was lethargic and disoriented, giving slow and illogical responses to questions. Her neck was supple. Her blood pressure was 148/102 mmHg. The remainder of the parameters examined was normal. Approximately 8 h after the patient’s arrival at the hospital, the patient suffered a tonic–clonic seizure.
The initial laboratory findings revealed a white cell count of 9090/µl (77.8% neutrophils), a hemoglobin level of 10.9 g/dl, and a platelet count of 161,000/µl. Liver and renal function tests were normal. Complement levels were normal. The tests for ANA and anti-dsDNA were negative. The patient’s urine was positive (1 g/l) for protein; the sediment contained 80 red cells/µl and no casts. The patient’s brain was normal, based on magnetic resonance imaging (MRI) findings. A lumbar puncture revealed normal opening pressure. The cerebrospinal fluid (CSF) was negative for cells, with normal glucose and protein levels. Smears and cultures for Cryptococcus neoformans, Mycobacterium tuberculosis, and other bacteria were negative. Serum tests for viruses were positive for cytomegalovirus (CMV) IgM. We did not perform polymerase chain reaction (PCR) or antibody assays using CSF for viruses.
We started the empirical treatment of the patient for bacterial meningitis with ceftriaxone, HSV-1 encephalitis with acyclovir, and possible NPSLE with MP. On the fifth hospital day, the patient was alert and afebrile, but had memory impairment. We continued ceftriaxone and acyclovir administration for 2 weeks.
On the 16th hospital day, the patient reported decreased vision in her left eye. Visual acuity (VA) was tested by counting fingers. Funduscopic examination revealed arteriolar occlusion and neuroepithelium atrophy in the macula region (Figure 1(a)). She was diagnosed with chronic retinal vasculitis attributed to SLE. Upon this diagnosis, we started treatment with 80 mg of MP per day and 0.4 g of cyclophosphamide (CTX) per week.
Fundus color photograph of the patient. (a) Day 16 fundus appearance showing arteriolar occlusion and neuroepithelium atrophy in the macula region in the left eye. The right eye was normal. (b) Day 39 fundus appearance showing ischemic retinal whitening, macula edema, and scattered hemorrhage in the right eye. (c) Day 53 fundus appearance showing diffuse yellow or white necrosis and hemorrhage in the right retina.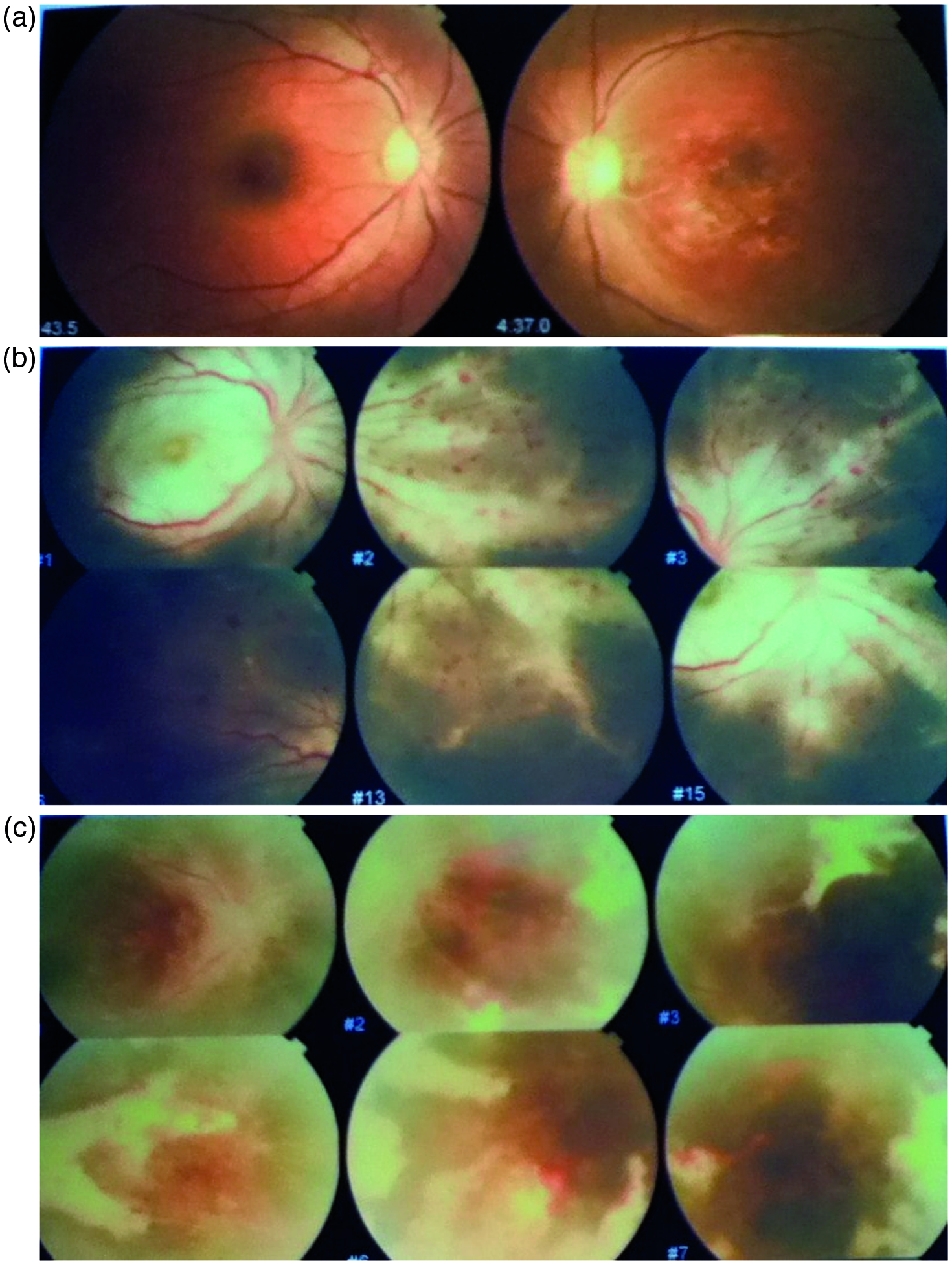
On the 37th hospital day, the patient noted decreased vision in her right eye, and on the 38th day she was unable to distinguish between light and dark. Funduscopic examination revealed ischemic retinal whitening, macular edema, and scattered retinal hemorrhage (Figure 1(b)). She was diagnosed with central retinal artery occlusion (CRAO). Non-contrast MRI of the brain was performed to obtain T2-weighted images, in which hyperintense signal was observed prominently in the left temporal lobe (Figure 2(a)). Magnetic resonance angiography was negative.
Magnetic resonance imaging (MRI) of the patient. (a) Day 40 MRI showing hyperintense signal in the left temporal lobe on T2-weighted images. (b) and (c) Day 50 MRI showing new hyperintense signal bilaterally in the occipital lobe and right parietal lobe on T2-weighted images.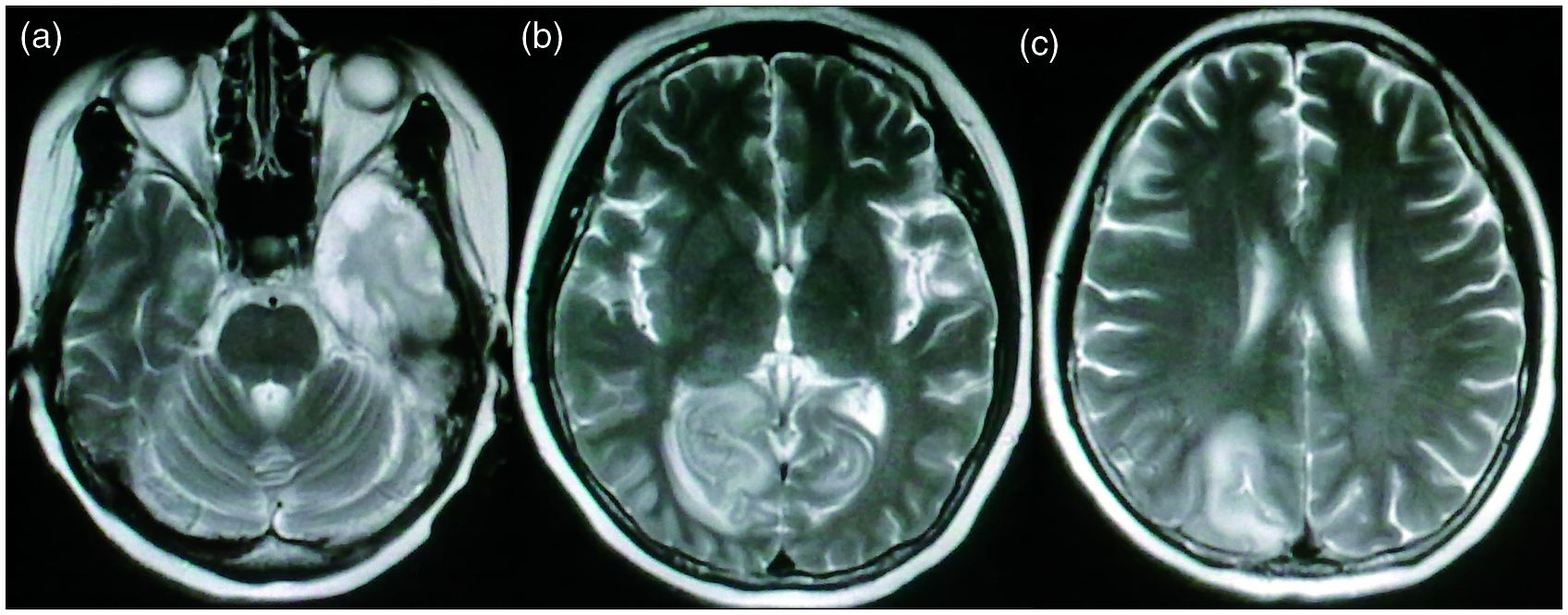
Based on these findings, we believed that the patient suffered from vasculitis affecting retinal and intracranial vessels due to SLE. We administered MP pulse therapy at 1 g per day for 3 days.
Nevertheless, the patient’s condition deteriorated, as she reported increasing pain in the right periorbital region and occiput. MRI showed new hyperintense signals in the bilateral occipital lobe and right parietal lobe in T2-weighted images with contrast enhancement and bleeding along the sulci in T1-weighted images (Figure 2(b) and (c)). Funduscopic examination revealed diffuse yellow or white necrosis and hemorrhage of the right retina. Based on these findings, we diagnosed the patient with acute retinal necrosis (Figure 1(c)). Lumbar puncture revealed normal opening pressure and CSF was negative for cells, with a glucose level of 1.7 mmol/l (normal range: 2.3–4.1 mmol/l), and a protein level of 1370 mg/dl (normal range: 150–450 mg/dl). The CD4+ T-cell count was roughly 33 cells/µl. CSF cultures were negative for bacteria. Toxoplasmosis, rubella, cytomegalovirus, and herpes simplex virus (TORCH) panel tests of CSF were positive for HSV-1 IgG. The patient was treated with intravenous acyclovir for 28 days, followed by oral acyclovir for 14 days. We stopped the administration of immunosuppressants and tapered MP dosage down. The patient’s condition improved gradually and the titer of HSV-1 IgG in her CSF declined. No new lesions appeared on follow-up MRI, but the original lesion and her vision problems did not improve.
Discussion
NP symptoms are common in patients with SLE. A prospective analysis of NP events in a cohort of SLE patients found that, over a mean follow-up of 1.9 ± 1.2 years, 486 out of 1206 (40.3%) patients had at least one NP manifestation, of which 13.0–23.6% were attributed to SLE, as a much higher percentage of events were attributed to non-SLE-related causes. 1 It is a challenge when a patient with SLE presents with NP symptoms, as there are usually a range of possible causes. Differentiating CNS infections from NPSLE is particularly difficult, because SLE can resemble every type of infection. For example, SLE with CNS manifestations resembling herpes simplex encephalitis has been reported. 2 However, HSV-1 encephalitis, necrotic retinitis, and non-necrotic retinitis occurring concomitantly in a patient with SLE has never been reported.
A recent review found that, after cytomegalovirus and human parvovirus B19, HSV is the third most common cause of viral infections in SLE patients. Moreover, HSV causes organ-specific infections and systemic infections, such as hepatitis, esophagitis, pneumonitis, pharyngitis, laryngitis, retinitis, cervix involvement, and encephalitis. 3 HSV-1 is the most common cause of sporadic encephalitis through CNS invasion via the trigeminal nerve, olfactory tract, or reactivation of latent HSV-1 in situ within the CNS. Diagnosis of HSV-1 encephalitis is based on its typical clinical presentation, including temporal lobe symptoms, new onset of epileptic seizures and/or disturbances in consciousness, detection of lesions in the mesial temporal lobe or in other parts of the limbic system by MRI, and a lymphocytic pleocytosis in the CSF. The gold standard for establishing the diagnosis is the detection of HSV-1 DNA in the CSF by PCR. The test has high sensitivity (98%) and specificity (94–100%).4,5 The use of purified HSV glycoprotein B to detect HSV antibodies in the CSF has a sensitivity of 97% and a specificity of 100%. 6
Although HSV-1 encephalitis is not more common among immunosuppressed patients, cases in immunocompromised patients, including those receiving radiotherapy or chemotherapy, those with different hematologic malignancies, transplant patients, and HIV-seropositive individuals, have been reported. HSV-1 encephalitis in this population presents with typical clinical symptoms and radiologic abnormalities, but CSF pleocytosis is usually absent or minimal.7–9 As described in the literature, our patient had typical lesions in the mesial temporal lobe and did not have CSF pleocytosis. Even though we did not test for HSV-1 DNA in the patient’s CSF, positive IgG for HSV-1 and the decline in titer after antiviral therapy confirmed the diagnosis. The patient’s complicated presentation unfortunately delayed the diagnosis.
If untreated, HSV-1 encephalitis mortality rate approaches 70%, and for those patients who do survive, significant neurologic morbidity occurs at a rate of nearly 97%. Acyclovir dosed at 30 mg/kg/day given in three divided doses improves upon mortality and morbidity, as evidenced by 28% mortality and 62% of survivors having some form of neurologic debility. The current course of 21 days of antiviral therapy is based primarily on the observation that patients whose CSF remains PCR positive for HSV DNA after the completion of 10 days of acyclovir still experience significant morbidity and mortality. With some reports of persistently positive PCR samples after 21 days of acyclovir, the duration of therapy beyond 21 days has been recommended in certain cases. 10
The outcome of HSV-1 encephalitis in immunosuppressed patients is not different from that in immunocompetent patients. Based on two case series,8,9 the mortality of HSV-1 encephalitis in patients with HIV infection is about 33.3% (2/6), which is not more than it is in immunocompetent patients. The mortality rate increases to 75% (9/12) when HSV-1 infection is concurrent with other viral encephalitis conditions, including CMV, Epstein-Barr virus, and HSV-2. In addition, a renal transplant patient with HSV encephalitis recovered completely without neurologic sequelae with acyclovir treatment for 4 weeks. 11 In view of our patient’s serious immunosuppressed state, we extended the antiviral treatment duration to 6 weeks. This extension in treatment saved her life, but if she had been diagnosed earlier she might not have suffered neurologic sequelae.
Ocular HSV-1 infections occur in less than 5% of patients, and cause conditions including keratitis, acute retinal necrosis (ARN), conjunctivitis, blepharitis, and chorioretinitis. Diagnosis of ARN is based on the presence of focal and well-demarcated areas of retinal necrosis located in the peripheral retina; rapid, circumferential progression of necrosis; evidence of occlusive vasculitis; and a prominent inflammatory reaction in the vitreous and anterior chamber. The etiologic agents of ARN, including varicella-zoster (VZV), HSV-1, HSV-2, and CMV, can be detected with PCR testing of vitreous and aqueous specimens. HSV-1-related ARN is highly associated with encephalitis. For example, a study showed that six of seven patients with HSV-1 ARN had a history of HSV encephalitis diagnosed from 3 months to 16 years prior to the onset of ARN. 12 HSV-related ARN is associated with poor VA (<20/200) in 48% of cases at presentation and 35% at 12 months follow-up. 13 The current treatment strategies include intravenous acyclovir, intravitreal antivirals, aspirin, and oral steroids. A recent study showed that not all treatments improve visual outcomes, 14 but treatment of ARN with acyclovir decreased the risk of fellow eye involvement. 15 Based on diffuse yellow or white necrosis of right retina and confirmed HSV-1 encephalitis, our diagnosis of HSV-1 ARN was definite. The patient’s poor VA, however, was not improved with acyclovir treatment.
A recent study proposed that, in addition to classic ARN, there are three additional types of herpetic uveitis with posterior involvement: (1) a slow type, with ARN-like necrotic lesions located in the retinal periphery, but characterized by slow progression, (2) vasculitis/papillitis, with absence of retinal necrotic lesions, and (3) panuveitis with lack of necrotic lesions and no obvious vasculitis or papillitis. 16 Several cases have shown that CRAO can be a rare complication of ARN,17–22 and in one of these cases, HSV-1 was the etiology of CRAO followed by ARN. 22 Thus, we concluded that the arteriolar occlusion and atrophy of the neuroepithelium in the macula region in the left eye was due to type 2 herpetic uveitis, and CRAO in the right eye was a complication of HSV-1-related ARN or the early presentation of the slow-type ARN.
With regards to ARN in immunosuppressed patients, a case series determined the characteristics of ARN in HIV-infected patients: rapid progression, a greater proportion of eyes with poor VA (80%), increased bilateral eye involvement (82%), increased sustained retinal detachment (70%), and more patients with accompanying CNS diseases (73%). 23 Thus, similar to patients with HIV that have the very low CD4+ T-cell counts, our patient had bilateral eye involvement with HSV-1 retinitis, poor VA outcome, and encephalitis.
In conclusion, immunocompromised due to MMF therapy, our patient suffered from HSV-1 encephalitis, necrotic retinitis, and non-necrotic retinitis simultaneously, with a presentation very similar to that of patients with HIV infections. Our extended treatment regime with acyclovir saved her life; however, the patient still suffered from remaining neurologic sequelae and poor VA. In addition, there were some limitations in this case: first, PCR for HSV-1 and VZV in the CSF, vitreum, or aqueous fluid was not obtained; second, a brain biopsy was not performed. In conclusion, a valuable lesson from this case was that we should differentiate CNS infections and NPSLE in patients with SLE, especially in those receiving immunosuppressive therapies.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors have no conflicts of interest to declare.