
Abstract

Sir,
Discoid lupus erythematosus is a chronic autoimmune connective tissue disorder characterized by specific skin manifestations of lupus erythematosus, which is a part of the spectrum of systemic lupus erythematosus. The cutaneous lesions observed in the patients are typically circumscribed, raised, erythematous and scaly and found on the face, scalp and ears in 70% of patients. 1 Orbital myositis is a rare inflammatory disorder of the extraocular muscles, resulting in painful diplopia exacerbated by eye movement. Some case reports have shown that orbital myositis is often associated with widespread systemic immunological inflammatory diseases. Systemic lupus erythematosus complicated with the orbital myositis is very rare,2–4 and there have been no reports of orbital myositis associated with discoid lupus erythematosus. We herein report the case of a discoid lupus erythematosus patient who manifested orbital myositis with subacute progressive ophthalmoplegia and pain with ocular movement.
A 42-year-old Japanese female complained of progressive diplopia in all directions with eyelid edema and ocular pain lasting for two weeks. She had a 10-year history of discoid lupus erythematosus treated with 50 mg/day of mizoribine. Discoid lupus erythematosus was diagnosed based on a facial discoid rash and a skin biopsy exhibiting lymphocytic infiltration throughout the dermis and epidermal layers. Although the patient also had arthralgia, she had experienced no active discoid lupus erythematosus episodes for five years. A physical examination revealed hyperpigmentation on her face, and a neurological examination showed bilateral ophthalmoplegia with a total limitation of eye movements, particularly vertical movement of the left eye (Figure 1(a)) and bilateral ocular pain in all directions. The laboratory evaluation revealed no leukopenia, thrombocytopenia or hemolytic anemia. The values of creatine phosphokinase, C3, C4, CH50 and thyroid function were normal. An immunological test revealed an increased antinuclear antibody titer of 1:40 (normal <40) with a speckled pattern while there were no serum autoantibodies, including anti-acetylcholine receptor, antithyroid and anti-dsDNA antibodies. No myositis-associated autoantibodies, including anti Jo-1, PM-Scl-100, PL-7, PL-12, M2, Ku (p70/80), SRP and Rib-P antibodies, or antimitochondrial antibodies of the M2 subtype were detectable in the serum. No malignant tumors were observed on whole-body computed tomography (CT). Orbital magnetic resonance imaging (MRI) scans revealed high-intensity signals of the extraocular muscles on fat-suppression T2-weighted images (Figure 1(b)) and an increased thickness of the extraocular muscles (Figure 1(c)).
The nine cardinal positions of gaze (a). The patient exhibited limitation of movement of the eyes, particularly the left eye. Coronal and axial and fat-suppression T2-weighted MRI scans of the orbit: orbital coronal MRI showed high signal intensity in the bilateral extraocular muscles (b), and axial MRI showed thickening of the bilateral medial and lateral rectus muscles with high intensity (c).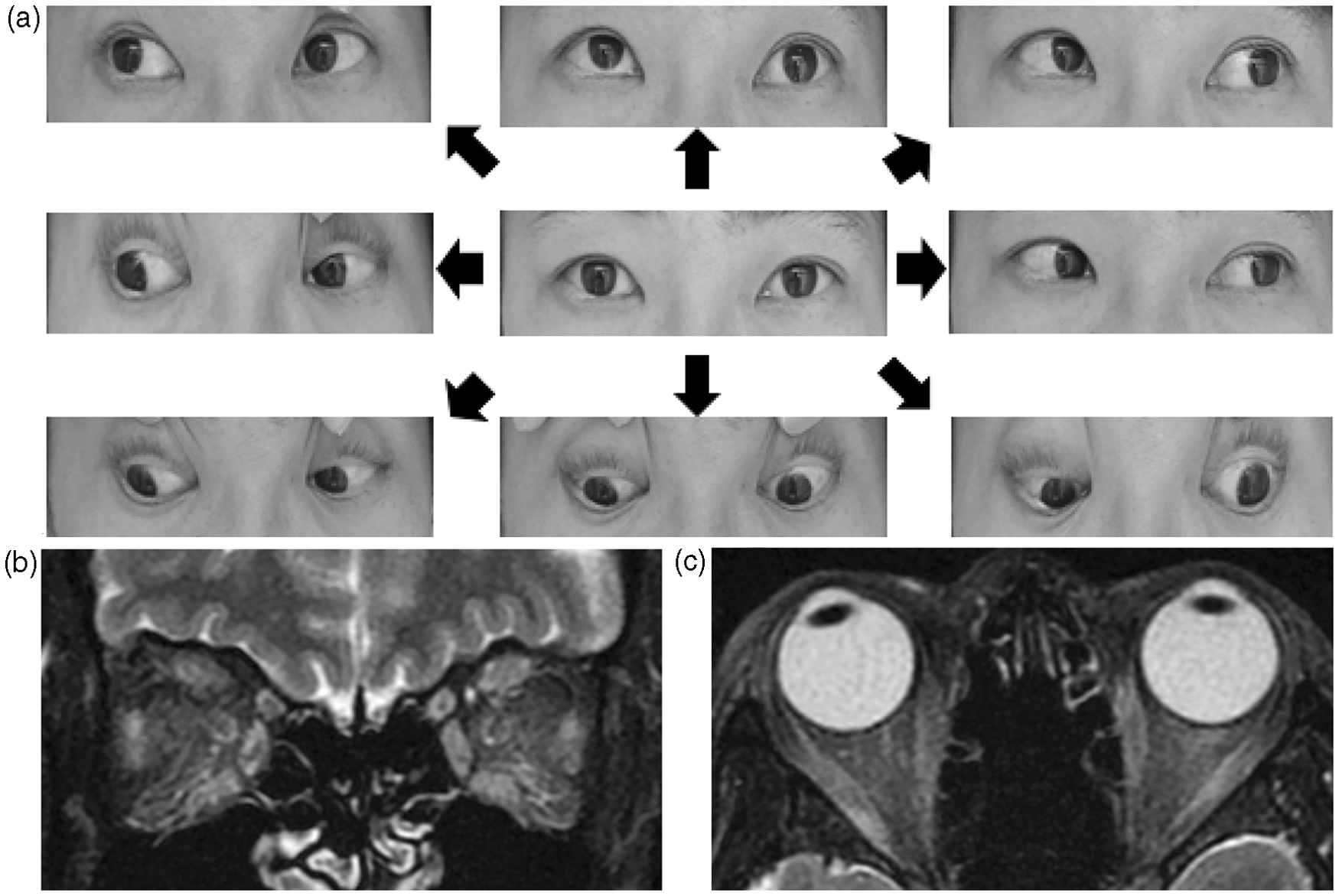
A diagnosis of orbital myositis was made based on the patient’s clinical features and abnormal MRI findings. Treatment was initiated with three courses of intravenous methyl prednisolone (1 g/day) for three days followed by oral prednisolone (20 mg/day). The patient’s ocular pain rapidly improved within several days, and the diplopia and abnormal MRI findings markedly improved two months after the steroid therapy.
Orbital myositis is characterized by the onset of painful and limited extraocular movements, diplopia, ptosis and swelling of the eyelids. Imaging of orbital myositis on MRI shows enlargement and high-intensity signals on T2-weighted images of the extraocular muscles, suggesting an inflammatory process in the orbital muscles. Orbital myositis may be a component of more widespread autoimmune-mediated inflammatory processes, such as systemic lupus erythematosus,2–4 rheumatoid arthritis, 5 dermatomyositis, 6 Crohn's disease 7 and the more recently described IgG4-related disease. 8 These reports indicate that an immune-mediated mechanism may underlie the pathology of orbital myositis. The pathological analysis showed a nonspecific inflammatory process with the infiltration of neutrophils, lymphocytes, macrophages and fibroblasts. 9 An immunohistochemical study showed infiltration with mast cells that was associated with the pathological condition. 10 However, it is not known why the extraocular muscles are specifically targeted. There has been no report of any specific autoantibody found in orbital myositis.
A previous clinical case report demonstrated presymptomatic enlargement of the extraocular muscles on CT imaging in a patient with discoid lupus erythematosus of the eyelids who presented with neither diplopia nor ocular pain. 1 Orbital myositis is associated with autoimmune disorders common to patients with discoid lupus erythematosus, as well as systemic lupus erythematosus. Additional case studies including the results of an orbital muscle biopsy and immunological investigations are needed to clarify the pathogenesis of orbital myositis associated with discoid lupus erythematosus.
This is the first case report of discoid lupus erythematosus accompanied by orbital myositis. Painful diplopia and abnormalities of the extraocular muscles on orbital MRI were diagnostic clues. Early treatment with a corticosteroid was useful for confirming the diagnosis and preventing permanent cicatricial ocular muscle changes.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors have no conflicts of interest to declare.