
Abstract
Objectives
Sleep disorders are common among patients with systemic lupus erythematosus (SLE) with unclear underlying mechanisms. We assessed the role of vitamin D in sleep quality of patients with SLE.
Methods
A retrospective study was conducted on women with SLE for whom the following data were available at the same time; sleep quality (Pittsburgh Sleep Quality Index (PSQI)), disease activity, cumulative disease damage, psychological state (Hospital Anxiety and Depression Scale (HADS)), and serum vitamin D level. Bivariate and regression analyses were computed to find contributors of sleep quality.
Results
In total, 63 women were studied. Serum vitamin D level was correlated with physical activity (r = 0.310, p = 0.015), season of assessment (r = −0.302, p = 0.016), the PSQI global score (r = −0.262, p = 0.043), anxiety score (r = −0.298, p = 0.021), and non-significantly with depression score (r = −0.218, p = 0.094). Including all variables into a linear regression model, vitamin D level was independently associated with the global PSQI score (beta = −0.364, p = 0.042). Association of vitamin D level with psychological state disappeared after controlling for season of assessment (beta = −0.248, p = 0.154).
Conclusions
We found a role for vitamin D in sleep quality of SLE patients. Further studies are warranted to confirm these results and to find possible mechanisms of action.
Introduction
Sleep disorders are highly frequent in patients with systemic lupus erythematosus (SLE), but the underlying mechanisms are yet unclear. 1 Previous studies have been focused on disease-related factors including disease activity, cumulative damage, and using corticosteroids, as well as psychological factors, mainly depression. 1 The results of previous studies have been controversial regarding disease-related factors, albeit most of them confirmed the major role of psychological factors in sleep quality of patients with SLE. 1
Vitamin D deficiency is commonly seen in patients with SLE and is associated with disease activity and clinical course. 2 In non-SLE populations, vitamin D deficiency has been shown to be associated with sleep disturbances and psychological health, particularly depression.3,4 Although several factors can affect sleep quality in patients with SLE, including demographic and disease-related as well as psychological factors, a role for vitamin D deficiency is also plausible.
There is no report on the effects of vitamin D on sleep quality in patients with SLE. Through a study on sleep quality of patients with SLE, we had access to simultaneous data on vitamin D levels of a part of our studied population. This study was a retrospective analysis of these data, and evaluated the association of vitamin D level with sleep quality in women with SLE.
Methods
Patients and settings
This retrospective study was done on data gathered from women with SLE referring to an outpatient clinic of rheumatology in Isfahan City (Iran) between January and July 2013. Inclusion criteria were a) the diagnosis of SLE based on the American College of Rheumatology (ACR) revised criteria for SLE; 5 b) age between 18 and 65 years; and c) having data on sleep quality, disease activity, cumulative disease damage, psychological state and serum vitamin D level at the same time. The original study was approved by the local university ethics committee and consent had been obtained from the patients for participation.
Assessments
Data included age, years of education, weight, height, physical activity (never/rarely, sometimes, and regular), disease duration, disease activity, cumulative disease damage, prednisolone use, serum vitamin D level, sleep quality, and anxiety and depression. Vitamin D deficiency was defined as serum 25-hydroxyvitamin D level of <50 nmol/l and insufficiency was defined as a level of 50–75 nmol/l. 6 The following standard measures have been used in the assessments.
Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K)
As one of the most commonly used measures of SLE activity, the SLEDAI-2K contains 24 items and covers clinical (16 items) and laboratory (8 items) variables. A total score of ≥6 indicates active disease state. 7
Systemic Lupus International Collaborative Clinics/American College of Rheumatology (SLICC/ACR) Damage Index
This index estimates the accumulated damage since the onset of the disease. It evaluates 12 organs and lupus-related as well as treatment-related complications. Damage is assessed only if it is persistent for at least 6 months. 8
Pittsburgh Sleep Quality Index (PSQI)
The PSQI is an 18-item self-report scale of the sleep quality within the preceding month. The PSQI evaluates seven components of sleep quality including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of medication for sleep, and daytime dysfunction due to poor sleep. Each component score is calculated and coded from 0 to 3, where 0 indicates “no difficulty,” and 3, “severe difficulty”. The global score ranges from 0 to 21, where scores of >5 indicates poor sleep quality. 9
The Hospital Anxiety and Depression Scale (HADS)
The HADS is a brief and widely used measure of anxiety and depressive symptoms in outpatient setting. The HADS contains 14 items and consists of two subscales of anxiety and depression. Each item is rated on a 4-point scale, giving a maximum score of 21 for each subscale. 10
Statistical analysis
Data were analyzed using the SPSS software for windows version 16.0. Pearson’s and Spearman’s correlations were computed to examine bivariate correlations between vitamin D level and other variables. Regression analyses were computed to test the association of vitamin D with global sleep quality and composite anxiety–depression score while controlling for demographic- and disease-related factors as well as season of assessment. A p-value of <0.05 was considered as statistically significant in all analyses.
Results
Patient characteristics
Characteristics of study participants (n = 63)
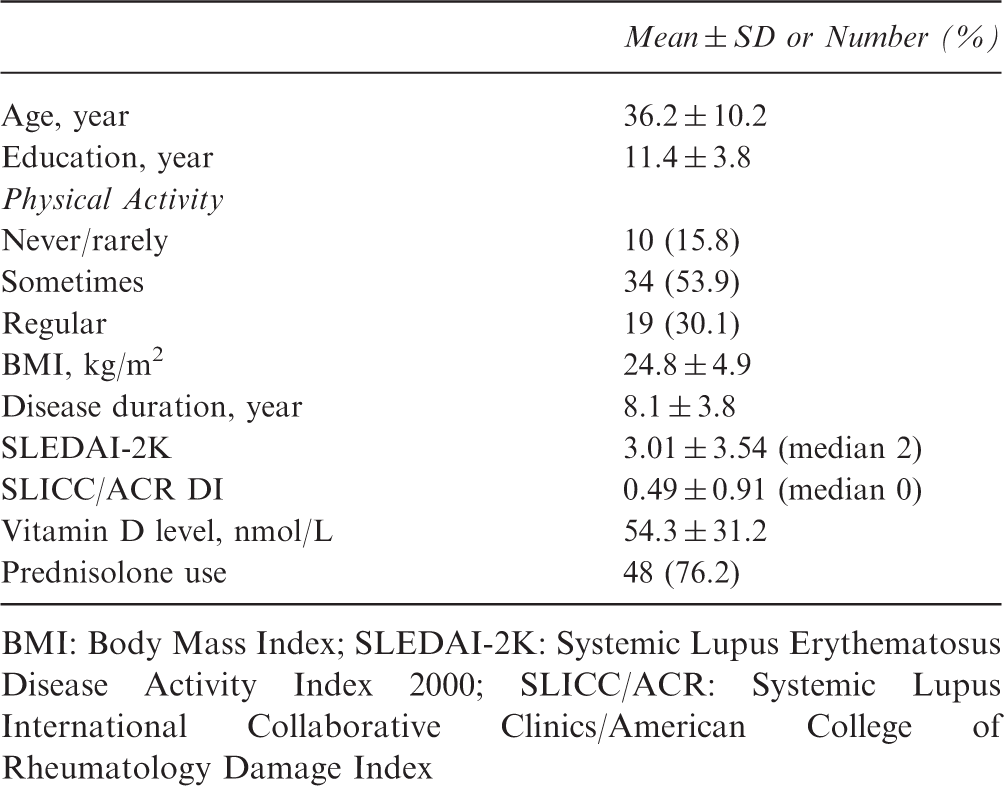
BMI: Body Mass Index; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000; SLICC/ACR: Systemic Lupus International Collaborative Clinics/American College of Rheumatology Damage Index
Bivariate correlations
Correlations of vitamin D level with study variables
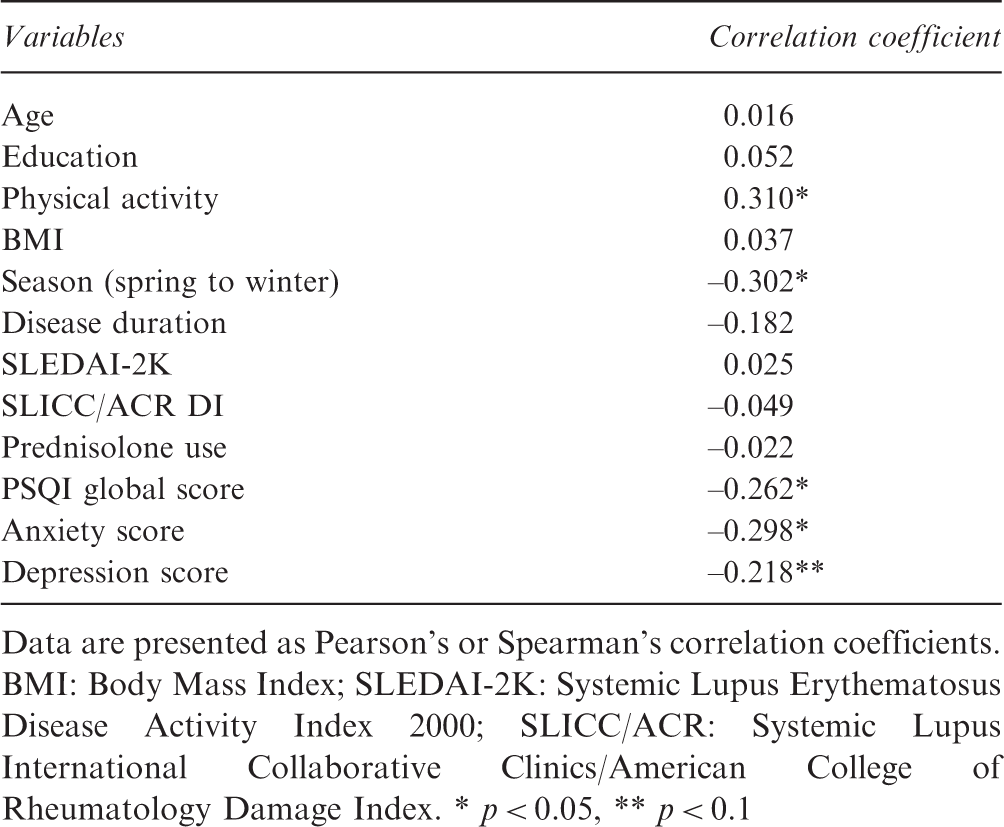
Data are presented as Pearson’s or Spearman’s correlation coefficients. BMI: Body Mass Index; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000; SLICC/ACR: Systemic Lupus International Collaborative Clinics/American College of Rheumatology Damage Index. * p < 0.05, ** p < 0.1
Multivariate analyses of vitamin D in association with sleep quality and psychological state
Regression analyses of vitamin D in association with sleep quality and psychological state
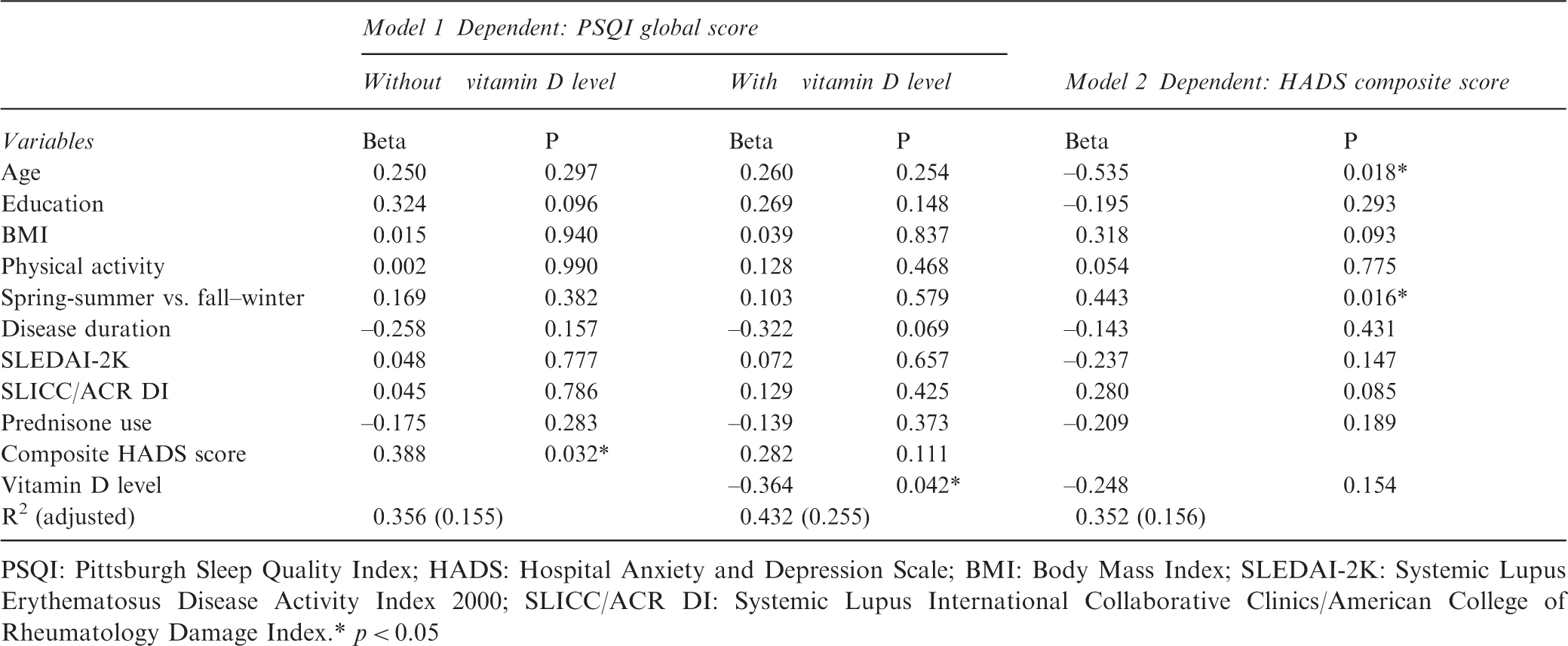
PSQI: Pittsburgh Sleep Quality Index; HADS: Hospital Anxiety and Depression Scale; BMI: Body Mass Index; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000; SLICC/ACR DI: Systemic Lupus International Collaborative Clinics/American College of Rheumatology Damage Index.* p < 0.05
Discussion
The pathogenesis of sleep disorders in patients with SLE is complex and multifactorial. Disease activity, pain, and fatigue, as well as psychological factors, particularly depression, are suggested as the underlying mechanisms by recent studies. 1 Vitamin D deficiency is highly frequent in patients with SLE 2 and has been shown to be associated with sleep quality and psychological health, especially depression, in non-SLE populations.3,4 However, no study to date has addressed the role of vitamin D in sleep quality of patients with SLE. Our preliminary study showed an independent contribution of vitamin D in sleep quality of women with SLE. Low vitamin D level in patients with SLE was associated with poorer sleep quality independently of demographic, disease, and psychological-related factors as well as season of assessment.
The underlying mechanisms of the association between vitamin D deficiency and sleep disorders are as yet unclear but seem to be multifactorial. 3 There is some evidence indicating an association between vitamin D deficiency and nonspecific skeletal pain which may disrupt sleep. 11 Evidence exist that vitamin D supplementation can improve pain and sleep in patients with chronic pain. 12 Vitamin D is also involved in immune regulation, and its deficiency can result in altered immunomodulation and increased production of inflammatory cytokines with effects on sleep. 3 Altered immune functions may lead to adenotonsillar hypertrophy, airway muscle myopathy, and chronic rhinitis, the contributor factors to obstructive sleep apnea, 3 which is a common type of sleep disorder seen in patients with SLE. 1 However, direct evidence is not reported in this regard in patients with SLE.
The other mechanism by which vitamin D may play a role in sleep quality of patients with SLE is its possible effect on psychological health. Emotional disturbances, mainly anxiety and depression, are significant contributors to insomnia and sleep quality, both in clinical and subclinical populations. 13 Depression is reported by previous studies as a significant contributor to sleep disturbance in patients with SLE. 1 A recent meta-analysis on cross-sectional as well as cohort studies showed an association between low vitamin D level and depression. 4 We found an association of vitamin D with the psychological state of patients with SLE, but the association was not significant after controlling for confounding factors including season. We found that season of assessment is associated with psychological state of the patients; autumn–winter was associated with more severe anxiety/depression compared with spring–summer. However, it is still possible that this association is partially mediated by vitamin D, as there is modest evidence on the role of vitamin D in seasonal mood variations. 14 Therefore, further studies are needed to investigate if vitamin D is associated with sleep problems via psychological mediators in patients with SLE.
In summary, the results of this preliminary study suggest a role for vitamin D in the sleep quality of patients with SLE. The association of vitamin D and sleep quality was independent of demographic, disease, and psychological factors as well as season of assessment. However, these results should be interpreted cautiously considering the retrospective design and limited sample size of the study. Further studies with larger sample size and prospective studies are warranted in this regard.
Footnotes
Funding
This study was supported by the Isfahan University of Medical Sciences [grant number 390534].
Conflict of interest statement
The authors have no conflicts of interest to declare.
Contributors
All authors of the manuscript contributed to: conception and design, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content and final approval of the version to be published.
Acknowledgments
We thank the patients who participated in this study.