
Abstract
Objectives
Health-related quality of life (HRQoL) has not been fully explored in antiphospholipid syndrome (APS); therefore, we compared HRQoL between APS patients and the general population and assessed the impact of thromboembolic history.
Methods
HRQoL was measured in a multicentre cohort study by the Medical Outcomes Study Short-Form 36 (MOS-SF-36) questionnaire. HRQoL scores were compared to the French general population norms. Factors significantly associated with an impaired HRQoL were identified.
Results
A total of 115 patients with aPL and/or systemic lupus erythematosus (SLE) were included (mean age 42.7 ± 14.1 years old, 86 women). In 53 patients APS was diagnosed. Compared to general population norms, patients with APS had an impaired HRQoL. SLE-associated APS patients had the worst HRQoL scores (physical component summary (PCS)=40.8 ± 10.6; mental component summary (MCS)=40.6 ± 16.5) in comparison with SLE or aPL patients without thromboembolic history. In APS patients, history of arterial thrombosis significantly impaired HRQoL (PCS score: 42.2 ± 9.4 vs 49.2 ± 8.5; MCS score: 33.9 ± 13.7 vs 44.6 ± 10.3).
Conclusion
Compared to the general population, APS patients experienced a lower HRQoL. In these patients, a history of arterial thrombosis significantly impaired HRQoL. Therefore, measurements of HRQoL should be included in APS patient management to assess the burden of the disease from a patient’s perspective and to provide patients with the support they need.
Keywords
Introduction
Antiphospholipid syndrome (APS) is characterized by the association of thrombotic or obstetrical events and persistent antiphospholipid antibodies (aPL). 1 APS can be considered as primary or associated to an underlying condition such as systemic lupus erythematosus (SLE). 2 APS patients are at high risk for thrombotic recurrences in the absence of an appropriate antithrombotic treatment. 3 Health-related quality of life (HRQoL) is an important outcome in patients with chronic diseases.4,5 While it has been clearly demonstrated that HRQoL is impaired in SLE, 6 and in patients with history of venous thrombosis,7–10 data are lacking in APS patients and it has been suggested that patients with either primary APS or SLE-associated APS had an impaired mental and physical health status.11–13 However, it is unknown to what extent the presence of APS, in particular a thromboembolic history – either arterial or venous – has an impact on HRQoL impairment. Therefore, the objectives of our study were a) to compare the HRQoL of APS patients to the French general population norms, and b) to assess the impact of thromboembolic history (either arterial or venous) on HRQoL in APS patients.
Patients and methods
Study population
This multicentre study was an ancillary study of the case-control TAC(I)T program (
Data collection
At inclusion, a full medical history and physical examination data were recorded. Baseline data included demographic information (age, sex), objectively documented APS (thrombotic, obstetrical events and aPL profile represented by either lupus anticoagulant (LA), anticardiolipin (aCL), or anti-β2 glycoprotein-I antibodies (anti-β2-GPI)) according to Sapporo/Sydney classification, 1 other features associated with APS (heart valve disease, livedo reticularis, thrombocytopenia, nephropathy, superficial vein thrombosis, neurological manifestations) and also thromboembolic and cardiovascular risk factors, medications, and inherited thrombophilia.
Definition of thrombotic events
Thrombotic events (arterial, venous, or small vessel thrombosis, in any tissue or organ) were confirmed by appropriate imaging workup. Thrombotic stroke was defined as a focal clinical neurologic event confirmed by neuroimaging studies such as computed tomography (CT) or magnetic resonance imaging. Acute myocardial infarction was defined as changes in a diagnostic electrocardiogram and increased levels of cardiac enzymes in the presence of typical symptoms such as chest pain and/or nausea, diaphoresis, or dyspnea. Pulmonary embolism was defined as positive result of ventilation/perfusion lung scan or spiral CT in the presence of typical symptoms, such as pleuritic chest pain, dyspnea, or hemoptysis. Deep vein thrombosis was defined by a symptomatic clinical event confirmed by compression ultrasonography. Small vessel thrombosis was defined as symptomatic events confirmed by an appropriate imaging (CT or magnetic resonance imaging) or histological techniques.
HRQoL assessment
HRQoL was assessed using the Medical Outcomes Study Short-Form 36 (MOS-SF-36) questionnaire. This tool is widely used to measure HRQoL in patients as well as in the general population. 16 Of note, while the MOS-SF-36 questionnaire is a generic, reliable and valid measure for HRQoL and has been used in a variety of conditions including APS,11–13 its validity and reliability in APS has not been assessed. The MOS-SF-36 questionnaire is self-administered and contains eight dimensions: bodily pain (BP), general health (GH), mental health (MH), physical function (PF), role-emotional (RE), role-physical (RP), social function (SF) and vitality (VT). A score from 0 (worse) to 100 (best) was calculated for each dimension of the MOS-SF-36. Two subscales were computed as two different weighted sums of dimension scores, i.e. a mental (MCS) and a physical component summary (PCS) score to obtain a mean of 50 with a standard deviation (SD) of 10 in a healthy general population. 17 Higher scores represent a better HRQoL. Three scales (BP, PF, RP) correlate most highly with the physical component and contribute most to the scoring of the PCS measure. The mental component correlates most highly with the MH, RE, and SF scales, which also contribute most to the scoring of the MCS measure. Three of the scales (GH, SF, and VT) have noteworthy correlations with both components.
Statistical analysis
Description of data
Qualitative data were presented as numbers and percentages and were compared using Fisher’s exact tests. Quantitative data were presented as the mean with SD or median with interquartile range (IQR) and were compared using the non-parametric Wilcoxon test.
HRQoL analysis: Comparison to the French general population norms
Regarding French MOS-SF-36 norms, details of the national survey assessing HRQoL in the French general population have been published elsewhere: 18 MOS-SF-36 was evaluated in 3617 French individuals (mean age was 49.6 ± 18.6 years old, female: 54%, non-responders: 1.18%). Seven age categories ranged from 18 to more than 74 years with 275 to 864 patients in each group. Cronbach’s coefficient ranged between 0.80 and 0.92, confirming the reliability of MOS-SF-36 in this population. MOS-SF-36 dimension scores were compared to the French population norms 18 according to age groups and sex using a Student t-test. In addition to statistical significance of the tests, a difference of more than five points in one of the eight dimension scores was considered as clinically significant.18,19 Because PCS and MCS weights had not been produced for the French norms, we did not use them for this comparison.
HRQoL analysis: Identification of characteristics associated with an impaired HRQoL
To assess the impact of clinical characteristics on HRQoL, all dimension scores as well as PCS and MCS scores were computed for different clinical variables and groups of patients. Firstly, univariate analysis identified all clinical variables associated with impaired HRQoL – defined as a lower PCS or MCS score. Then, we performed a multivariate analysis using multiple linear regression to identify independent variables. A p value < 0.05 was considered statistically significant. SAS 9.3 software (SAS Institute Inc, Cary, NC, USA) was used to perform analyses.
Ethics policy
This study was approved by the institutional regional review board (CPP III Est), and written informed consent was obtained from all participants.
Results
Patient characteristics at inclusion
Patient characteristics at inclusion
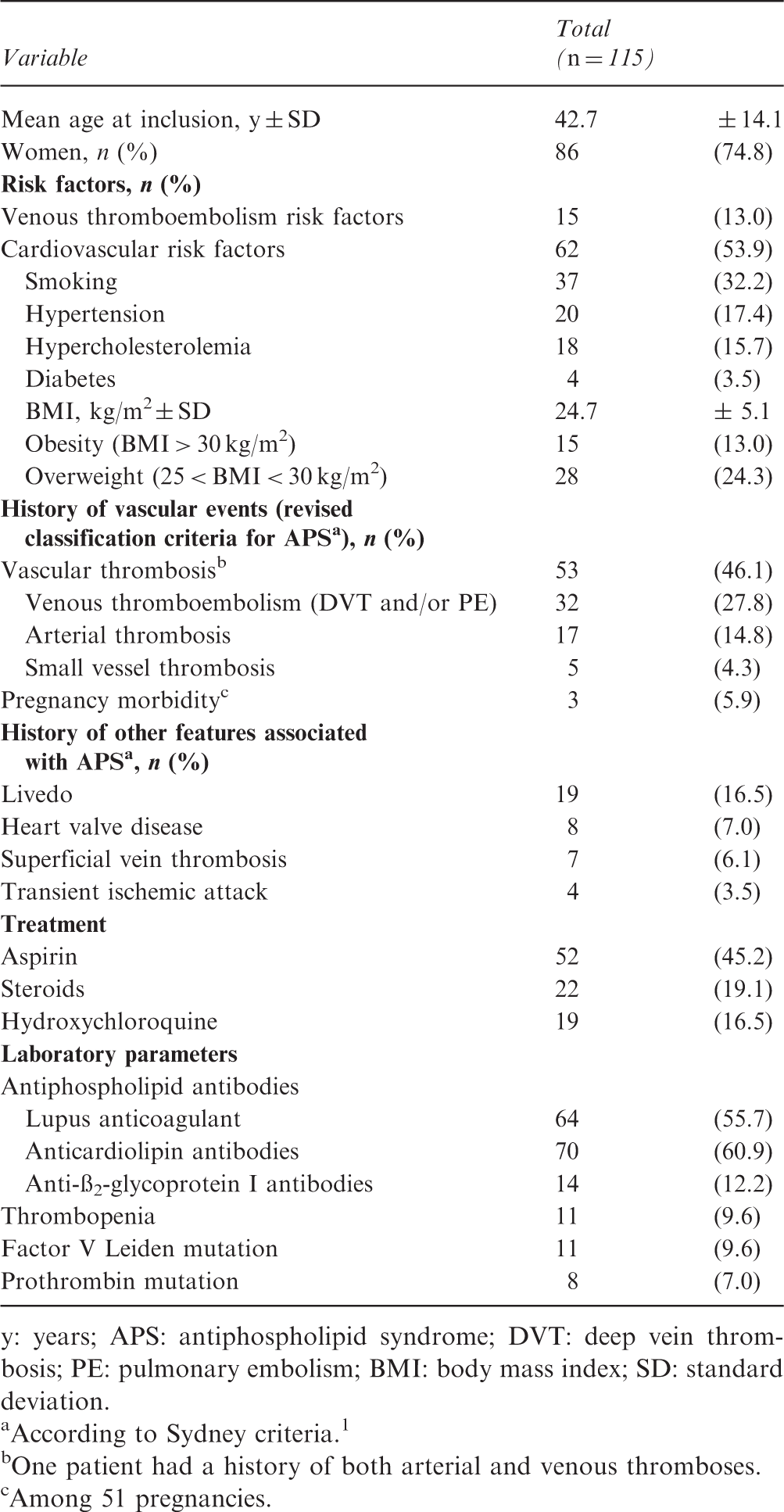
y: years; APS: antiphospholipid syndrome; DVT: deep vein thrombosis; PE: pulmonary embolism; BMI: body mass index; SD: standard deviation.
According to Sydney criteria. 1
One patient had a history of both arterial and venous thromboses.
Among 51 pregnancies.
Comparison of HRQoL between patients and the French general population
Among these patients, all dimension scores – except for the PF dimension – were significantly lower than French general population norms (Supplemental Table 1).
HRQoL according to age
In comparison with the French general population norms, all HRQoL dimension scores were significantly impaired from the 25- to 54-year-old age groups. These impairments were also considered as clinically relevant based on a difference of more than five points. In patients aged 18 to 24 years, only three dimensions were significantly lower than in the general population (RP, GH, RE). In patients aged 55 to 64 years, SF, RE and MH were significantly lower while no difference of dimension scores was found between ages 65 to 74 years (Supplemental Table 1). Patients from 45 to 54 years old had the highest HRQoL impairment compared to the general population. PF, BP, VT and SF were significantly and dramatically impaired from age 25 to 54 years old, RP and GH from 18 to 54 years old, RE from 18 to 64 years old, and MH from 25 to 64 years old (Supplemental Figure 1).
Comparison of mean MOS-SF-36 dimension scores according to disease status.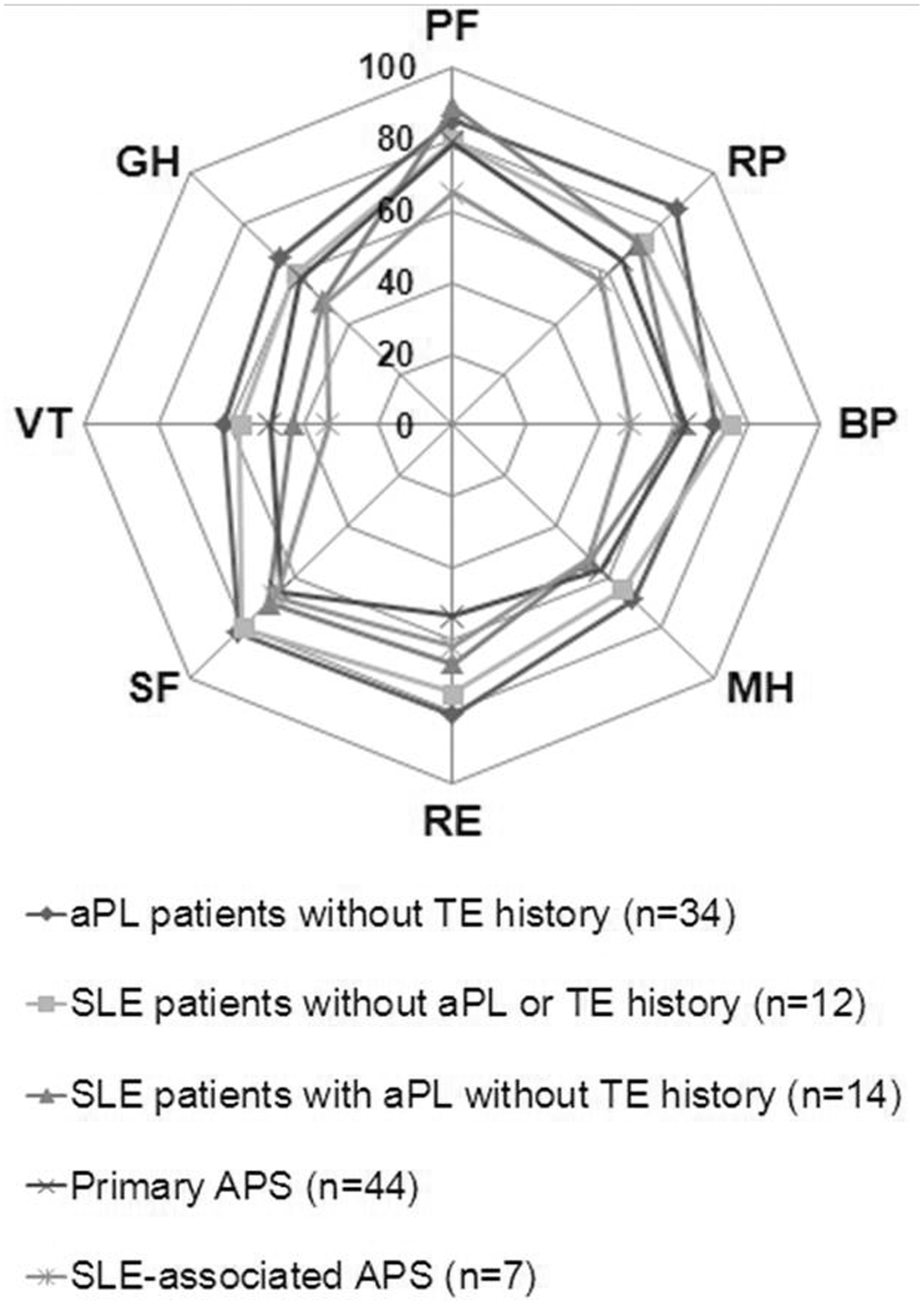
HRQoL according to sex
Compared to the general population, HRQoL in men was significantly impaired in all dimension scores. In women, only GH, VT, SF, RE and MH dimensions were significantly lower than in the general population (Supplemental Table 1). For 25- to 34-year-old patients, more HRQoL dimensions were impaired in women than in men (all dimensions except SF in women and PF, RP, BP and GH in men). Furthermore, in 35- to 44-year-old patients, more HRQoL dimensions were impaired in men than in women (all dimensions in men and only BP, GH, MH dimensions impaired in women). These results suggest that an impairment of HRQoL began earlier in women than in men.
HRQoL according to disease status
PCS and MCS scores according to diseases status
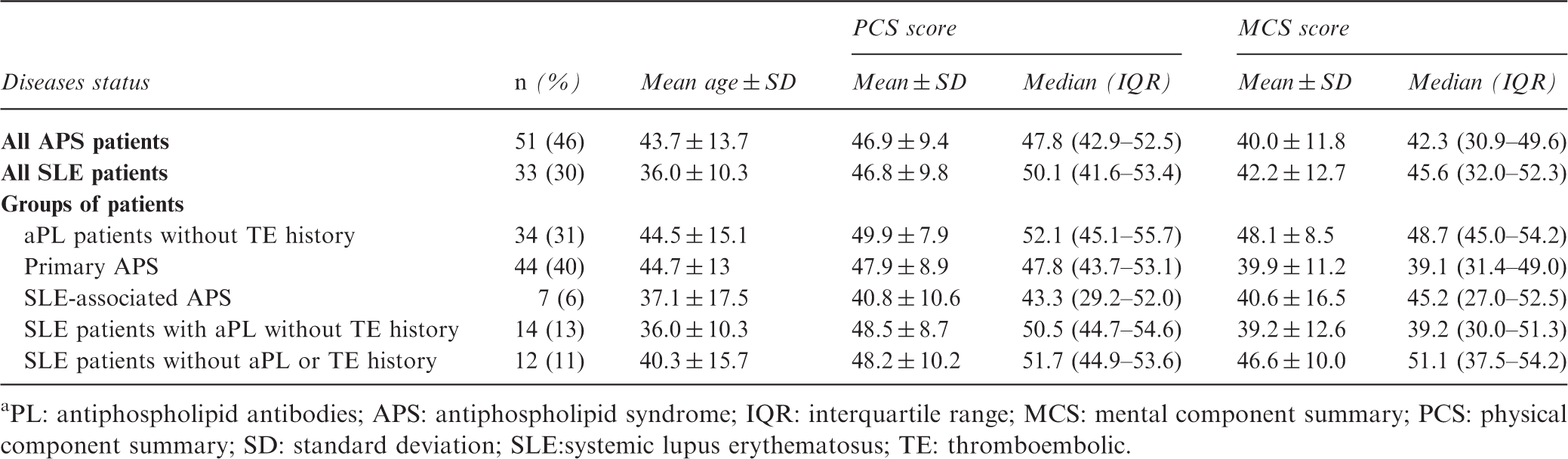
PL: antiphospholipid antibodies; APS: antiphospholipid syndrome; IQR: interquartile range; MCS: mental component summary; PCS: physical component summary; SD: standard deviation; SLE:systemic lupus erythematosus; TE: thromboembolic.
Regarding MOS-SF-36 dimensions (Figure 1), MH (p = 0.03), SF (p = 0.03), VT (p = 0.001) and GH (p = 0.04), were significantly different among groups of patients. SLE-associated APS patients seemed to be associated with the worst HRQoL scores in comparison with other patients. Furthermore, among SLE patients, a significant negative correlation was found between SLEDAI values and PF dimension only (R = 0.38, p = 0.03).
MOS-SF-36: Medical Outcomes Study Short-Form 36; aPL: antiphospholipid antibodies; APS: antiphospholipid syndrome; SLE: systemic lupus erythematosus; TE: thromboembolic. SF-36 dimensions: PF: physical function; RP: role-physical; BP: bodily pain; MH: mental health; RE: role-emotional; SF: social function; VT: vitality; GH: general health.
Impact of clinical variables on HRQoL impairment
Impact of cardiovascular risk factors on HRQoL impairment
Hypertension (p = 0.016), hypercholesterolemia (p = 0.031) and obesity (p < 0.001) were significantly associated with impaired PCS scores, and smoking was associated with impaired MCS scores (p = 0.028) (Supplemental Table 2).
Impact of clinical characteristics on HRQoL impairment
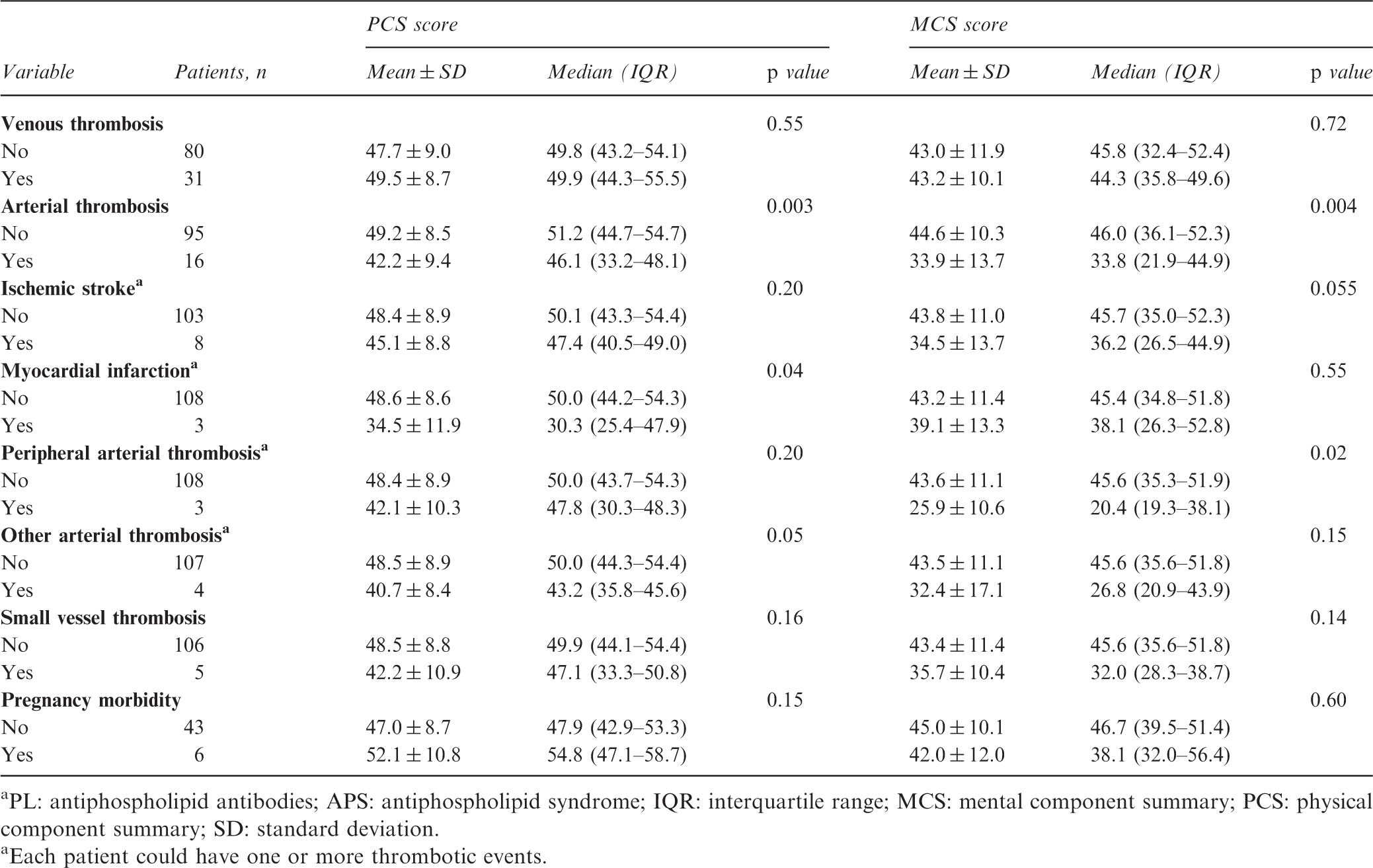
In APS patients with a history of arterial thrombosis compared to those without, HRQoL was dramatically impaired in all dimensions (Figure 2) and in both PCS and MCS scores (Table 3). In particular, a history of myocardial infarction was significantly associated with impaired PCS scores (p = 0.04) while peripheral arterial thrombosis was associated with impaired MCS scores (p = 0.02). Decreased MCS scores of patients with a history of ischaemic stroke did not reach statistical significance (p = 0.055). Other APS clinical classification criteria such as history of venous thromboembolism, of small vessel thrombosis or of pregnancy morbidity were not significantly associated with HRQoL impairment (Table 3).
Comparison of mean MOS-SF-36 dimension scores according to the presence of arterial thrombosis. MOS-SF-36: Medical Outcomes Study Short-Form 36; MOS-SF-36 dimensions: PF: physical function; RP: role-physical; BP: bodily pain; MH: mental health; RE: role-emotional; SF: social function; VT: vitality; GH: general health. Association between APS classification clinical criteria and PCS and MCS scores PL: antiphospholipid antibodies; APS: antiphospholipid syndrome; IQR: interquartile range; MCS: mental component summary; PCS: physical component summary; SD: standard deviation. Each patient could have one or more thrombotic events.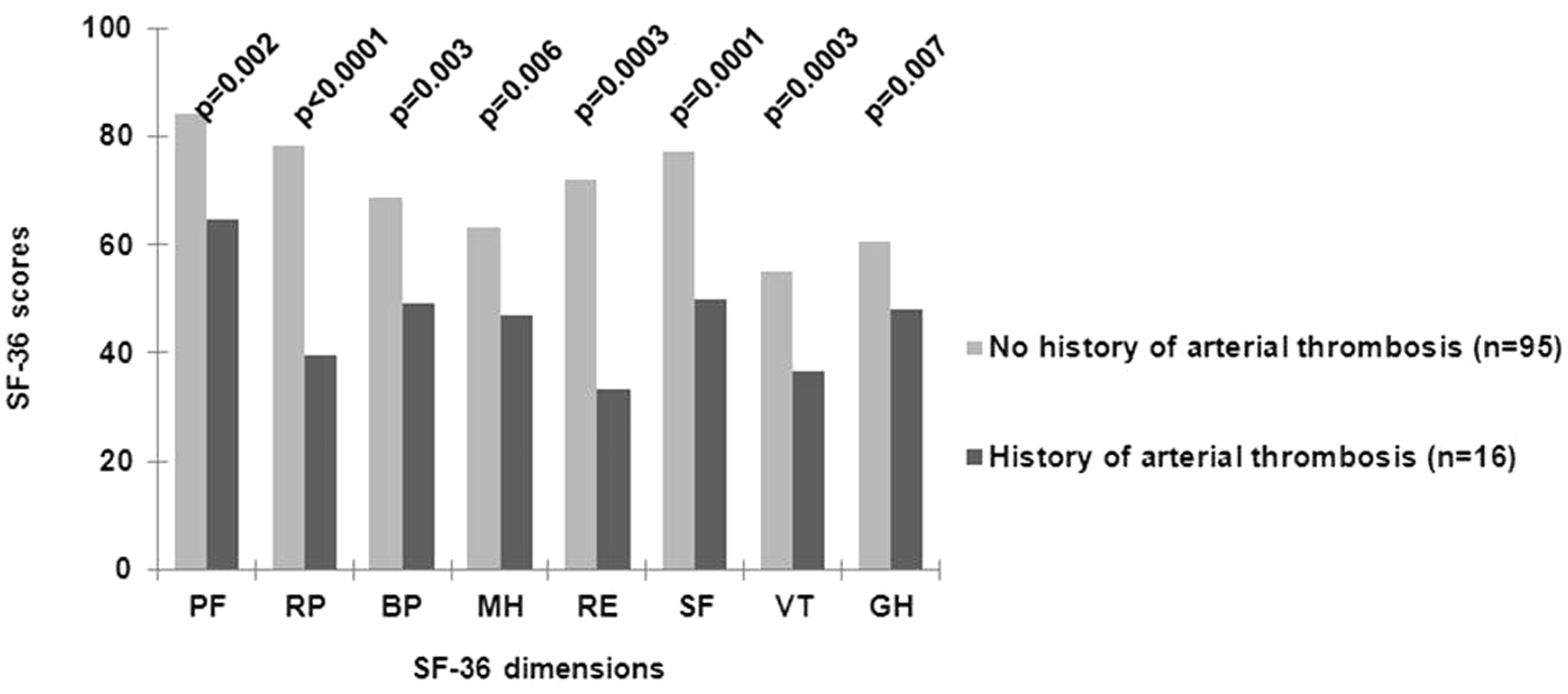
Finally, when age, arterial thrombosis and any cardiovascular risk factors were entered in a multivariate model using multiple linear regression, arterial thrombosis remained the only independent factor significantly associated with an impaired PCS or MCS score.
Discussion
Our study clearly demonstrated that patients with APS had an impaired HRQoL in comparison with general population norms stratified by age and sex. Furthermore, our results showed that SLE-associated APS patients have the worst HRQoL in comparison with patients with aPL and/or SLE. Finally, we found that arterial thrombosis was associated with the worst HRQoL in APS patients.
The impact of aPL and APS on HRQoL has not been fully clarified yet. Costa et al. showed that primary APS patients had a lower HRQoL in comparison with healthy individuals. 12 Similarly, we confirmed that APS patients had an impaired HRQoL when results were compared with French norms stratified by age and sex. Balitsky et al. found that SLE patients with aPL without thrombosis had better PCS scores than APS or SLE patients with thromboembolic history. 11 Likewise, we have confirmed that asymptomatic aPL-positive patients had better HRQoL scores than patients with either APS or aPL and SLE. Furthermore, our results have shown that HRQoL in asymptomatic aPL patients was close to the mean score of a healthy general population. 18 Finally, in this study, we found that APS patients have the worst HRQoL, especially those who have both APS and SLE, which is in line with another recent study. 13
Whether the type of thromboembolic history influenced HRQoL has not been studied in APS patients previously. In the general population, a history of either arterial20,21 or venous thrombosis is associated7–10,22 with impaired HRQoL assessed by the MOS-SF-36. Because of the design of the study patients had either arterial or venous thrombosis and we were able to compare the two groups. Our results demonstrated important differences between the types of thrombosis in APS patients. Comparing all subscales of the MOS-SF-36 questionnaire to the French general population norms adjusted for age and sex, we identified a subset of young patients between 25 and 54 years old with a clinically significant impaired HRQoL mainly associated to a history of arterial thrombosis. A history of arterial thrombotic events dramatically impaired HRQoL independently of cardiovascular risk factors, which was not previously reported in this population. Myocardial infarction rather affected physical health more than other types of arterial thrombosis. These data are in line with previous results described above in a general population. Regarding mental dimensions, peripheral arterial disease and to a lesser extent stroke impaired HRQoL. Regarding history of venous thrombosis, the absence of reported HRQoL impairment may be due to the age of APS patients. While patients with a post-thrombotic syndrome in the general population appeared to have an impaired HRQoL, 23 it can be hypothesized that younger APS patients –who have experienced a venous thrombotic event – had not yet developed a severe post-thrombotic syndrome potentially affecting their HRQoL. The role of cardiovascular risk factors on HRQoL has been studied in the general population. It has been established that obesity, 24 smoking,25,26 hypertension 27 and hypercholesterolemia 28 could lead to a decreased HRQoL and that risk factors had cumulative effects. 29 Our results did show that obesity, smoking, hypertension and hypercholesterolemia were associated with a lower HRQoL in the study population. Finally, even if age was different among groups of patients (e.g. APS or SLE patients), analyses were adjusted for age and confirmed the impact of thrombosis history on HRQoL impairment.
Some characteristics of our cohort may lead to possible limitations: First, we have included consecutive patients either with aPL/APS and SLE – two closely related disorders – 30 that reflected everyday clinical practice. Second, patients were not on oral anticoagulants at inclusion; thus, we measured only the burden of the disease and not that of anticoagulant treatment. Moreover, we may have selected less-severe patients than typical APS patients whose quality of life may even be lower. Finally, even if we found a correlation between HRQoL and lupus activity measured by the SLEDAI, we could not demonstrate that APS patients with mild SLE had better HRQoL compared to APS SLE patients with moderate or severe disease.
In conclusion, our study clearly demonstrates that APS patients have a dramatic impairment of their HRQoL compared to the general population. A history of arterial thrombosis was the main factor affecting HRQoL. Thus, we suggest that measurements of HRQoL should be included in everyday APS patient management to assess the burden of the disease from a patient’s perspective as well as an outcome criterion in therapeutic studies especially in clinical trials, together with classical endpoints such as recurrence of thrombosis and survival. Further studies should investigate the characteristics of HRQoL impairment in APS and specifically evaluate health interventions to improve patients’ perception of quality of life.
Footnotes
Acknowledgements
The authors wish to thank Alfousseyni Coly for his assistance in project coordinating and monitoring and Benoît-Damien Caritey for his assistance in statistical analysis.
Funding
This work was supported by grants from the Ministère Français de la Santé et des Sports (Programme Hospitalier de Recherche Clinique) (D.W., T.L.), the Fondation de France (D.W., T.L.), and the Région Lorraine (D.W., T.L.). The funding organizations are public institutions and had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
Conflict of interest statement
The authors have no conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.