
Abstract
Introduction
Many studies have shown that differences were observed between male and female lupus patients. Although systemic lupus erythematosus (SLE) affects mostly females (female:male ratio 9:1), male SLE patients show higher mortality due to kidney and neurological disease. Currently there are limited epidemiological data concerning lupus in the Chinese population. As such, the Chinese SLE Treatment and Research group (CSTAR) developed the first online registry of Chinese lupus patients in 2009, and represents a multicenter observational study that attempts to describe and compile the major clinical characteristics of lupus in Chinese patients.
Objective
To investigate the effect of gender on the phenotypes of Chinese SLE patients.
Patients and methods
Data for 2104 SLE patients were prospectively collected and included in the CSTAR registry. Patients fulfilled the 1997 American College of Rheumatology (ACR) SLE classification criteria. We conducted a cross-sectional case-control study to analyze patient clinical and laboratory data at onset and at enrollment. SLE disease activity scores (SLEDAI) were also measured at enrollment.
Results
This study included 1914 women and 190 men. Males and females showed no differences in mean ages at onset, delay of diagnosis and disease duration. Males presented more frequently with fever (p = 0.003), while musculoskeletal involvement (p = 0.001) and cytopenia (p = 0.017) was more common in females as the initial manifestation at onset of SLE. For manifestations at enrollment, males presented more frequently with fever (p = 0.005), renal disease (p = 0.019), vasculitis (p = 0.032) and neuropsychiatric lupus (p = 0.007). For cumulative manifestations at enrollment, males presented more frequently with discoid rash (p < 0.001) and neuropsychiatric lupus (p = 0.036), while less frequently with arthritis (p = 0.011). However, the laboratory data showed no significant differences between the two groups at enrollment. Males also had higher SLEDAI scores at enrollment (p = 0.002).
Conclusions
Renal disease, vasculitis and neuropsychiatric lupus are more common in male SLE patients with higher SLEDAI scores compared to female SLE patients in China.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease with diverse clinical and immunological features. 1 During the past several decades, different reports have showed that SLE usually affects women of childbearing age, and only 4–22% of the lupus population is male. 2 Many studies showed that differences were observed between male and female lupus patients with respect to epidemiology, clinical manifestations, therapy and outcomes. 3 However, conclusions about distinguishing disease features remain controversial because of several factors, including ethnic origin, genetic and environmental aspects, selected ascertainment of clinical features, duration of follow-up and the small sample size in several studies.2,3 Better characterization of gender-based differences in clinical features and disease severity would assist physicians in providing optimum care for SLE patients. Currently there are limited epidemiological data concerning lupus in the Chinese population. 4 Most studies that do exist were conducted retrospectively or at a single center. As such, the Chinese SLE Treatment and Research group (CSTAR) developed the first online registry of Chinese lupus patients in 2009, and represents a multicenter observational study that attempts to describe and compile the major clinical characteristics of lupus in Chinese patients. 5
The aim of this study was to analyze the prevalence of clinical features of SLE in male patients and compare them to females to investigate the effect of gender on lupus expression in a large (2104) cohort of patients included in CSTAR.
Methods
Patient recruitment
Our analysis of preliminary data was based on the CSTAR online registry, 5 which includes patients from 104 high-ranking rheumatology centers, covering 30 provinces in China. This study was approved by the Medical Ethics Committee of the Peking Union Medical College Hospital, which was the lead site. Written informed consent was obtained from all patients. Baseline data for 2104 Chinese patients with SLE who fulfilled four or more criteria for SLE diagnosis as defined by the 1997 revised American College of Rheumatology (ACR) criteria6,7 were registered between April 2009 and February 2010.
Data collection
All CSTAR centers used the same protocol-directed methods to provide uniform evaluations and to record patient data. Investigators received training on diagnostic confirmation, disease activity evaluation, data input and data quality control. Demographic data were generally collected and included gender, age at onset, age at diagnosis, age at enrollment, family history of rheumatic diseases and reproductive history, as well as socioeconomic status, education and marital status. Delay of diagnosis was defined from the time of the initial manifestation at onset of SLE to the diagnosis time. Manifestations at enrollment meant the manifestations patients had around 10 days at enrollment. Cumulative manifestations at enrollment meant the manifestations that patients had ever had until enrollment. Systemic manifestations (e.g. neuropsychiatric SLE, vasculitis, arthritis, myositis, lupus nephritis, rash, oral ulceration, alopecia, pleuritis, pericarditis and fever) were assessed using the SLE Disease Activity Index (SLEDAI). All occurrences were classified according to SLEDAI definitions. Neuropsychiatric SLE included central nervous system (CNS) involvement and peripheral nervous system involvement. The features of CNS involvement included seizure disorder, psychosis, organic encephalopathy, visual impairment, cranial neuropathy, lupus headache and cerebrovascular disease.
Laboratory findings were also recorded, including leukocytopenia, thrombocytopenia, hypocomplementemia and autoantibodies. Autoantibodies were measured at the local labs at each center, and included antinuclear antibody (ANA), anti-double-stranded DNA (anti-dsDNA) antibody, anti-Sm antibody, anti-ribosomal RNA-protein (anti-rRNP) antibody, anti-SSA antibody, anti-SSB antibody, anti-u1 small-nuclear RNA-protein (anti-RNP) antibody and antiphospholipid (aPL) antibody. Most centers detected ANA and anti-dsDNA antibodies using an immunofluorescence assay with the Hep-2 cell line, while the anti-extractable nuclear antigen (ENA) antibody (including anti-Sm, anti-SSA, anti-SSB, anti-RNP, and anti-rRNP antibodies) was tested with an immunoblotting assay. The aPL antibody was tested using an enzyme-linked immunosorbent assay (anticardiolipin and anti-β2 glycoprotein I antibody) or dilute Russell viper venom test (lupus anticoagulant) when antiphospholipid syndrome was suspected or we tried to confirm the diagnosis of SLE according to the classification criteria, although these tests were not mandatory. aPL included anticardiolipin, lupus anticoagulant and anti-β2-glycoprotein-I antibodies. aPL positivity was defined as at least one positive result of these three assays. Lupus disease activity was evaluated in all patients by SLEDAI and physician global assessment (PGA). The SLEDAI was analyzed at enrollment.
Statistical analysis
Univariable analyses were performed using chi-square tests for categorical variables, and the student t-test or Mann-Whitney U test for continuous variables according to the normality. Potential risk/likelihood of a particular variable association with male gender was determined by odds ratio (OR). Logistic regression was used to compute ORs and 95% confidence intervals (CIs). All tests were two tailed, and values of p < 0.05 were considered to be statistically significant. Analyses were performed using SPSS for Windows, version 19.0 (SPSS, Chicago, IL, USA).
Results
Patients
Demographic characteristics and disease activity score of SLE patients in different genders.
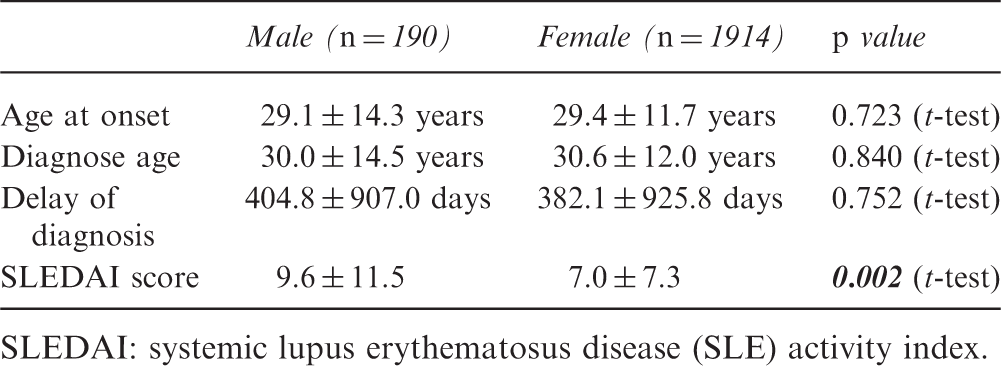
SLEDAI: systemic lupus erythematosus disease (SLE) activity index.
Clinical manifestations
Initial manifestation at onset of SLE patients in different genders.
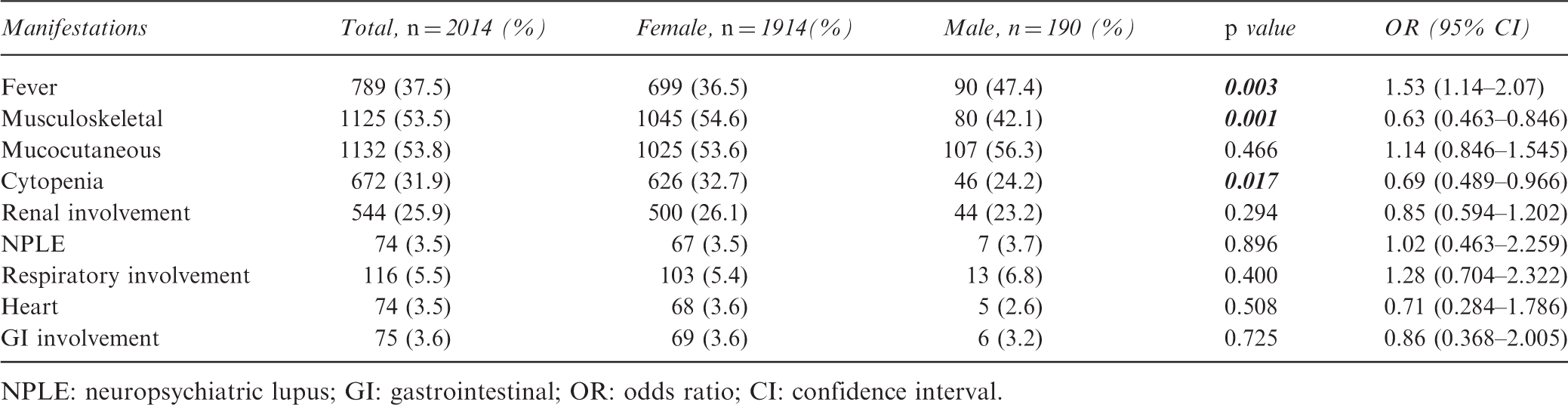
NPLE: neuropsychiatric lupus; GI: gastrointestinal; OR: odds ratio; CI: confidence interval.
Manifestations at enrollment of SLE patients in different genders.
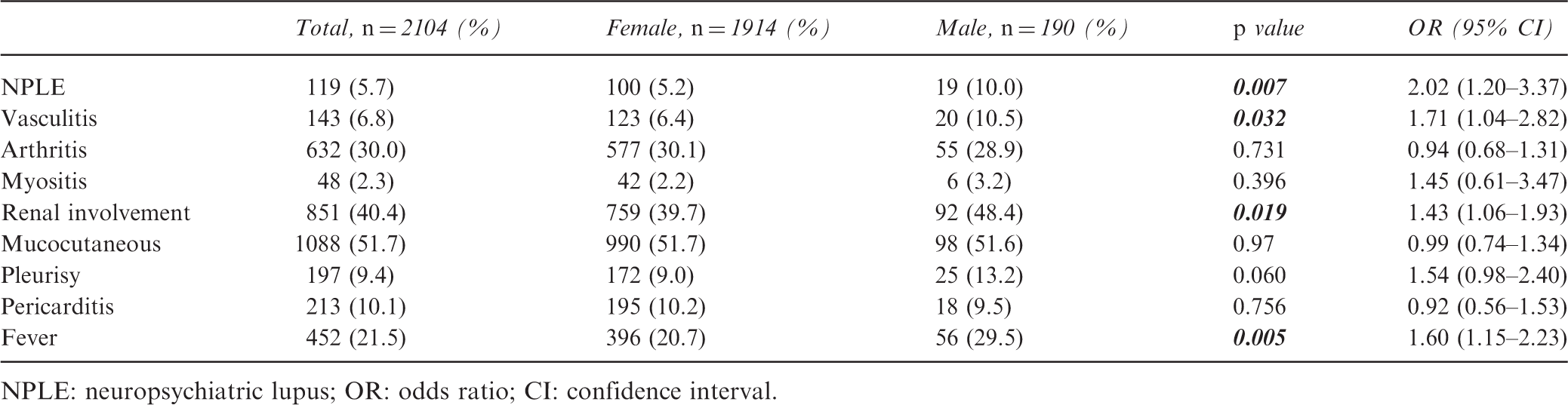
NPLE: neuropsychiatric lupus; OR: odds ratio; CI: confidence interval.
Cumulative manifestations at enrollment of SLE patients in different genders.
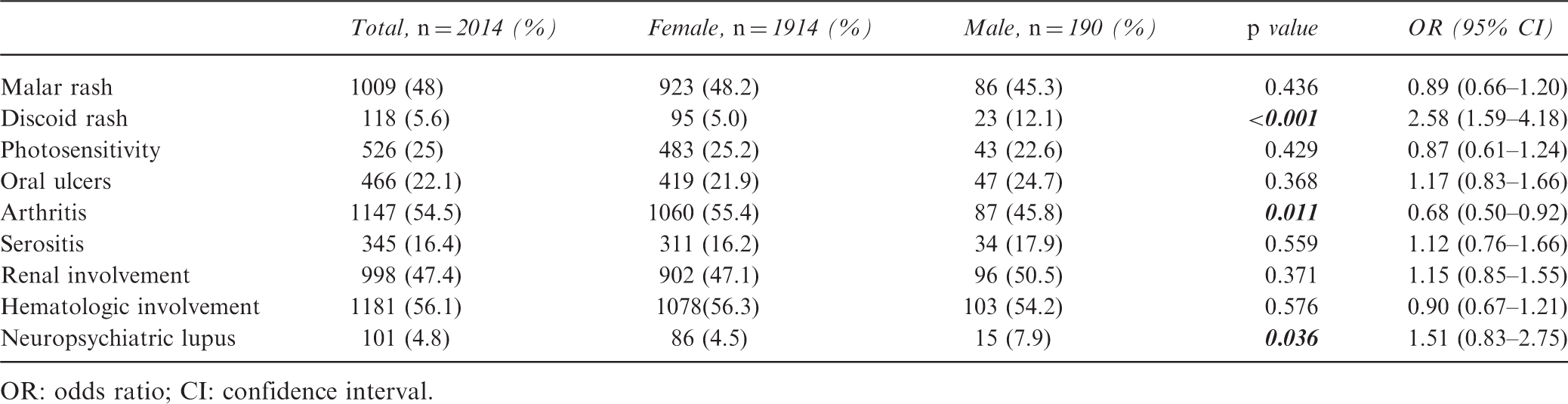
OR: odds ratio; CI: confidence interval.
Laboratory findings
Laboratory tests of SLE patients in different genders.
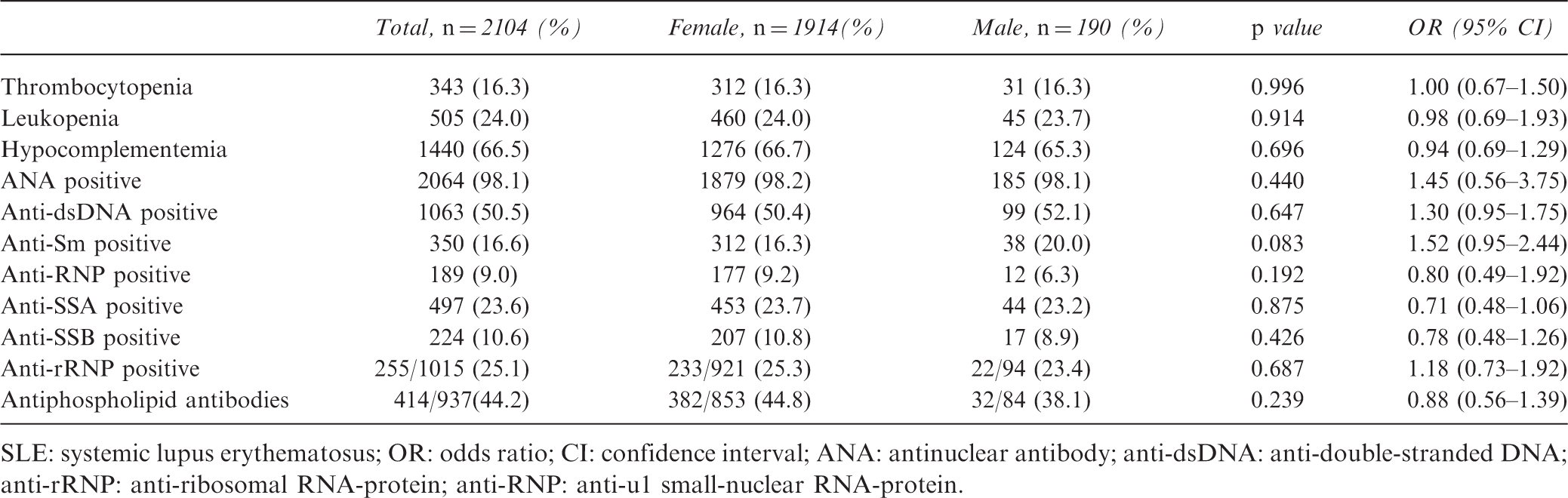
SLE: systemic lupus erythematosus; OR: odds ratio; CI: confidence interval; ANA: antinuclear antibody; anti-dsDNA: anti-double-stranded DNA; anti-rRNP: anti-ribosomal RNA-protein; anti-RNP: anti-u1 small-nuclear RNA-protein.
SLE disease activity
The SLEDAI score was significantly higher in male patients than in female patients (9.6 ± 11.5 vs 7.0 ± 7.3, p = 0.002) (Table 1).
Discussion
The CSTAR patient study examined here showed a female:male incidence ratio of 10:1, which is similar to that seen in previous studies.8,9 Other studies reported that the incidence rose among females during the teenage and child-bearing years, while males exhibited no concurrent increase, suggesting that female sex hormones are a possible factor for this disease. 8 We found no differences between the two groups in terms of the age at onset or diagnosis age. However, two previous studies did report an older age of SLE onset in males compared with females in the Caucasian subpopulation of their cohort.10,11 Thus, the age of onset in males and females may differ among certain ethnicities. 12
Our study showed some major clinical differences between lupus in males and females. We found that males presented more frequently with fever, which was similar to a study from Latin America that suggested that males might display more constitutional symptoms at diagnosis. 13 Furthermore, these observations may indicate that male patients experience more inflammatory conditions than female patients with lupus.
Discoid rash occurred at a significantly higher rate in males, which is in agreement with several past studies.14–16 However, we found no differences in other mucocutaneous features between the two sexes. Some previous reports showed that men were less likely to have dermatologic manifestations, including malar rash, photosensitive rash, oral ulcers, alopecia, and Raynaud’s phenomenon (RP). 10 Arthritis was found to be significantly less common in male SLE patients in our study, which concurred with previous studies.10,15,17–21 Moreover, reduced arthralgia/arthritis rates have been reported in Chinese (p = 0.02), 4 Greek (p = 0.004) 22 and Caucasian (p < 0.03)12,15 populations.
Many authors reported that male patients with SLE might have a more aggressive disease course, 10 especially for renal disease.3,4,10,13,15,18,20,21,23,24,25 In our study, we obtained results that were similar to prior studies in that males had renal disease (p = 0.019) more frequently than females. Results from previous cohorts have also suggested that male SLE patients have an increased risk of renal disease that is independent of ethnicity and age.10,20,26 However, several studies showed no difference in renal biopsy frequency at diagnosis or the resultant histology.2,12 Besides lupus nephritis, we also found that male patients had neuropsychiatric lupus (p = 0.007) more frequently than females, which is in agreement with previous reports.10,25 In addition, male patients had a higher incidence of vasculitis (p = 0.032) than females. Lupus nephritis, neuropsychiatric lupus and vasculitis all contribute to the SLEDAI score, which would explain why male SLE patients had higher SLEDAI scores than females and a more severe disease condition (p = 0.002), which is also supported by past studies. Although several studies found that the status of some autoimmune antibodies such as anti-dsDNA, anti-RNP, anti-Ro antibody and anti-La antibody differed by gender, 12 we found no significant serological differences between the two groups.
Other researchers also reported that compared to female patients, male patients with lupus showed more frequent system involvement, such as increased rates of gastrointestinal (GI) symptoms 22 and cardiovascular damage.4,10 However, no significant difference was found between the two genders in our study for manifestations in either the GI or cardiovascular systems.
Many studies, including ours, showed substantial gender differences in disease manifestations, and that male SLE patients had more severe disease expression in some organs. Although the mechanisms behind these differences await detailed characterization, Lu et al. 2 have reviewed some hypotheses to explain these gender differences, including the sex hormone, sex chromosome and intrauterine selection hypotheses.10,27,28 Umiker et al. showed that dosage of X-linked Tlr8 plays a major role in the high incidence of disease in females. 29 Hughes et al. found that men required a higher cumulative genetic load than women to develop SLE, suggesting that sex bias in autoimmunity could be influenced by autosomal genetic susceptibility loci. 30 However, a recent study has shown the lack of a clear trend toward higher genetic risk in one of the sexes for the analyzed SLE loci. 31 The pathogenesis of SLE remains unclear, but most likely involves the interaction of genetic, hormonal and environmental factors.32,33 Beyond these factors, some studies showed that men tended to have later onset of SLE and diagnosis, leading to the speculation that male patients might be less likely to seek medical assistance which in turn leads to later presentation with more clinical manifestations, and subsequently greater organ damage and higher mortality rates.10,34
Summary of studies of male vs female SLE.
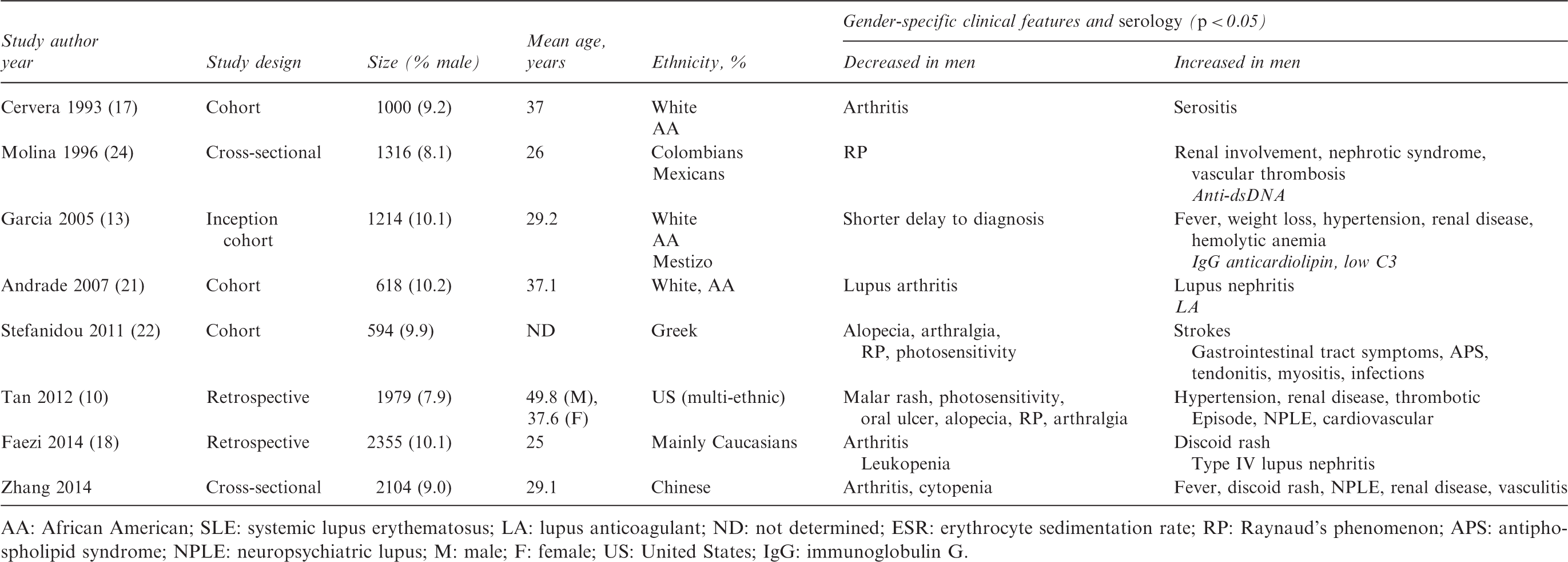
AA: African American; SLE: systemic lupus erythematosus; LA: lupus anticoagulant; ND: not determined; ESR: erythrocyte sedimentation rate; RP: Raynaud’s phenomenon; APS: antiphospholipid syndrome; NPLE: neuropsychiatric lupus; M: male; F: female; US: United States; IgG: immunoglobulin G.
In summary, renal disease, vasculitis and neuropsychiatric lupus were more common in male SLE patients in the CSTAR study. Male patients also showed higher SLEDAI scores.
Footnotes
Funding
This work was supported by the Chinese National Key Technology R&D Program, Ministry of Science and Technology (2008BAI59B02), the Chinese National High Technology Research and Development Program, Ministry of Science and Technology (2012AA02A513), the Research Special Fund for Public Welfare Industry of Health, Ministry of Health (201202004) and National Major Scientific and Technological Special Project for “Significant New Drugs Development” Ministry of Science and Technology (2012ZX09303006-002).
Conflict of interest statement
The authors have no conflicts of interest to declare.