
Abstract
Neuropsychiatric disorders associated with systemic lupus erythematosus are very common. Treatment generally consists of glucocorticoids and immunosuppressive therapy; however, some cases are unresponsive. Electroconvulsive therapy (ECT) is a recognized treatment modality in psychiatry and is an option for refractory cases of neuropsychiatric lupus. This report describes three cases of neuropsychiatric lupus that improved with ECT after failure of antipsychotics and immunosuppressive therapy. All cases met DSM-5 criteria for catatonia (case 1: agitation, stereotypies, and grimacing; case 2: stupor, mutism, and grimacing; case 3: agitation, mutism, and stereotypies); therefore, ECT was indicated. This case series shows that ECT can be a therapeutic option in patients with neuropsychiatric lupus, especially when associated with catatonia and unresponsive to conventional treatment.
Introduction
Neuropsychiatric disorders are reported in 14–75% of patients with systemic lupus erythematosus (SLE). This wide variability in the prevalence of central nervous system involvement in SLE is partly due to the absence of a gold standard for diagnosis. Psychosis is one of the neuropsychiatric manifestations associated with SLE and generally occurs in the context of multisystemic active disease, associated mainly with cutaneous and hematological manifestations. 1 Diagnosis and management of neuropsychiatric lupus remains a challenge for rheumatologists. Therapy is empirical and based on clinical experience.
Electroconvulsive therapy (ECT) is a psychiatric treatment modality that uses electricity applied via electrodes to the scalp to induce controlled convulsions. It is used for management of severe depression, schizophrenia, mania, and refractory catatonia. In patients with neuropsychiatric lupus, ECT has shown promising results in cases of catatonia, mania, and severe depression, with or without psychotic symptoms. 2
The present report describes three cases of severe neuropsychiatric lupus with catatonia that responded to ECT after failure of antipsychotic and immunosuppressive therapy.
Methods
We report three cases from hospitalized patients with refractory neuropsychiatric lupus with catatonia who received ECT with improvement of symptoms. The patients were from two different centers, one from Hospital de Clínicas de Porto Alegre and the others from Hospital Universitário Clementino Fraga Filho in Rio de Janeiro, both in the division of rheumatology. Subsequently, we conducted an extensive review of the scientific literature about the use of ECT in patients with lupus using the MEDLINE (PubMed), EMBASE, SciELO, Cochrane Library, and BIREME databases. The following search queries were used: “lupus AND electroconvulsive therapy” and “SLE AND electroconvulsive therapy.” Articles and abstracts in Portuguese, Spanish, or English from 1967 to 2014 were included in the literature review. Clinical response to ECT was assessed by the Bush-Francis Catatonia Rating Scale, which is one of the most widely used systems for catatonia classification. Catatonia was identified according to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria (three or more of the following symptoms are required: catalepsy, waxy flexibility, stupor, agitation, mutism, negativism, posturing, mannerisms, stereotypies, grimacing, echolalia, and echopraxia).
Case reports
Patient 1
A 25-year-old female patient with a 13-year history of SLE, who had thrombocytopenia, non-erosive arthritis, positive antinuclear antibodies (ANA), positive anti-ribosomal P protein antibody, and neuropsychiatric lupus, was treated with glucocorticoids and cyclophosphamide, followed by azathioprine as maintenance therapy. Six years later, she presented with a new episode of neuropsychosis and was treated with methylprednisolone and cyclophosphamide pulse therapy for six months, at which time a new relapse was detected. This relapse did not respond to pulse therapy with methylprednisolone, cyclophosphamide, rituximab, or intravenous immunoglobulin. Brain magnetic resonance imaging (MRI) was normal, cerebrospinal fluid (CSF) analysis was nonspecific for infections, and tests for antiphospholipid, anti-double-stranded DNA (anti-dsDNA) and anti-Sm antibodies were negative. The patient developed catatonia (agitation, stereotypies, and grimacing)and depression with suicidal ideation. Despite treatment with immunosuppressive drugs, antipsychotics, antidepressants, and anxiolytics, no response was obtained. As psychiatric symptoms persisted despite intensive medical therapy, the patient received ECT, applied with bilateral electrodes and using a brief-pulse square wave ECT device (Mecta Spectrum 4000 M). After the fourth ECT session, the patient exhibited significant improvement in psychiatric symptoms, with restoration of the sleep-wake cycle. Recovery of function was assessed using the Bush-Francis Catatonia Rating Scale, which yielded scores of 20 before ECT and 8 after the last ECT session, denoting significant clinical improvement.
Patient 2
A 26-year-old woman with SLE was admitted for management of neuropsychiatric lupus. The patient had been diagnosed with SLE at age 18 years, presenting with the following diagnostic criteria: positive ANA, non-erosive arthritis, malar rash, and photosensitivity. Hydroxychloroquine and intermittent topical and/or oral glucocorticoids had been used to control cutaneous and articular disease activity. Three months before admission, the patient’s cutaneous manifestations worsened gradually, with psoriasiform lesions consistent with subacute cutaneous lupus progressing to diffuse erythroderma with small, painless oral ulcers on the palate and tongue. Subsequently, she developed mental confusion, disorientation, and psychosis, associated with visual and auditory hallucinations, cognitive disturbance, loss of critical judgment, and catatonic episodes (stupor, mutism, and grimacing). The patient had no history of convulsions and no family history of psychotic diseases. Laboratory tests revealed autoimmune hemolytic anemia and low complement levels (C3 and C4). Tests for antiphospholipid, anti-dsDNA, and anti-Sm antibodies were negative. Brain MRI and electroencephalography were normal and CSF analysis was noncontributory. Positron emission tomography (PET) images were consistent with cerebral perfusion defects in the frontoparietal and thalamic regions. After ruling out infection, immunosuppressive therapy with cyclophosphamide and pulse therapy with methylprednisolone were administered in combination with antipsychotics, antidepressants, and anxiolytics, but failed to produce any clinical response. As psychiatric symptoms remained unchanged despite two months of pharmacotherapy, the patient received 12 consecutive sessions of ECT, which were applied with bilateral electrodes and using a brief-pulse square wave ECT device (Mecta Spectrum 4000 M). Progressive improvement was observed after the third session. After the end of ECT, she was able to return to daily activities, with restoration of critical judgment and cognitive improvement. The patient’s Bush-Francis Catatonia Rating Scale score decreased from 45 immediately before ECT to 1 after ECT.
Patient 3
A 35-year-old woman with a six-year history of SLE (with malar rash, photosensitivity, non-erosive arthritis, hemolytic anemia, alopecia, positive ANA and negative antiphospholipid and anti-dsDNA antibodies at the time of diagnosis) was admitted to our hospital with psychotic symptoms, agitation, and disorientation. Brain MRI and CSF analysis showed no abnormalities. The patient received methylprednisolone and cyclophosphamide pulse therapy. After three weeks, psychiatric symptoms progressed to a catatonic state (agitation, mutism, and stereotypies), despite institution of quetiapine and lorazepam therapy. A trial of ECT was started on the 30th hospital day. ECT was performed with unilateral electrodes and using a brief-pulse square wave ECT device (Mecta Spectrum 4000 M) three times a week. The patient exhibited a dramatic response after the third session, with recovery of ability to speak and obey commands. ECT was discontinued after the 10th session. The patient displayed continuous improvement of cognitive function, without recurrence of psychotic symptoms after 12 months of follow-up on maintenance treatment with mycophenolate mofetil, hydroxychloroquine, and risperidone. The patient’s Bush-Francis Catatonia Rating Scale score decreased from 27 immediately before ECT to 3 after ECT.
Discussion
Psychosis is an uncommon and severe neuropsychiatric manifestation of SLE. In a longitudinal study that followed SLE patients for nine years, Appenzeller et al. reported symptoms of psychosis in 17% of patients; 66% of cases were attributable to disease activity, 31% were associated with glucocorticoid therapy, and 3% were a result of primary psychosis.3,4 In another study of 11 SLE patients who presented with psychosis, the average time between diagnosis of SLE and onset of psychotic symptoms was 10 months, with 80% of cases occurring in the first year of the disease and 60% of patients presenting with psychotic manifestations at the time of SLE diagnosis. 5 The average age at diagnosis of psychosis was 29 years (similar to that of the cases described in our series), with all patients developing psychosis as part of multisystem SLE activity and 90% presenting with simultaneous cutaneous lesions. 5
Clinical profile and results of ECT treatment of patients with refractory neuropsychiatric lupus
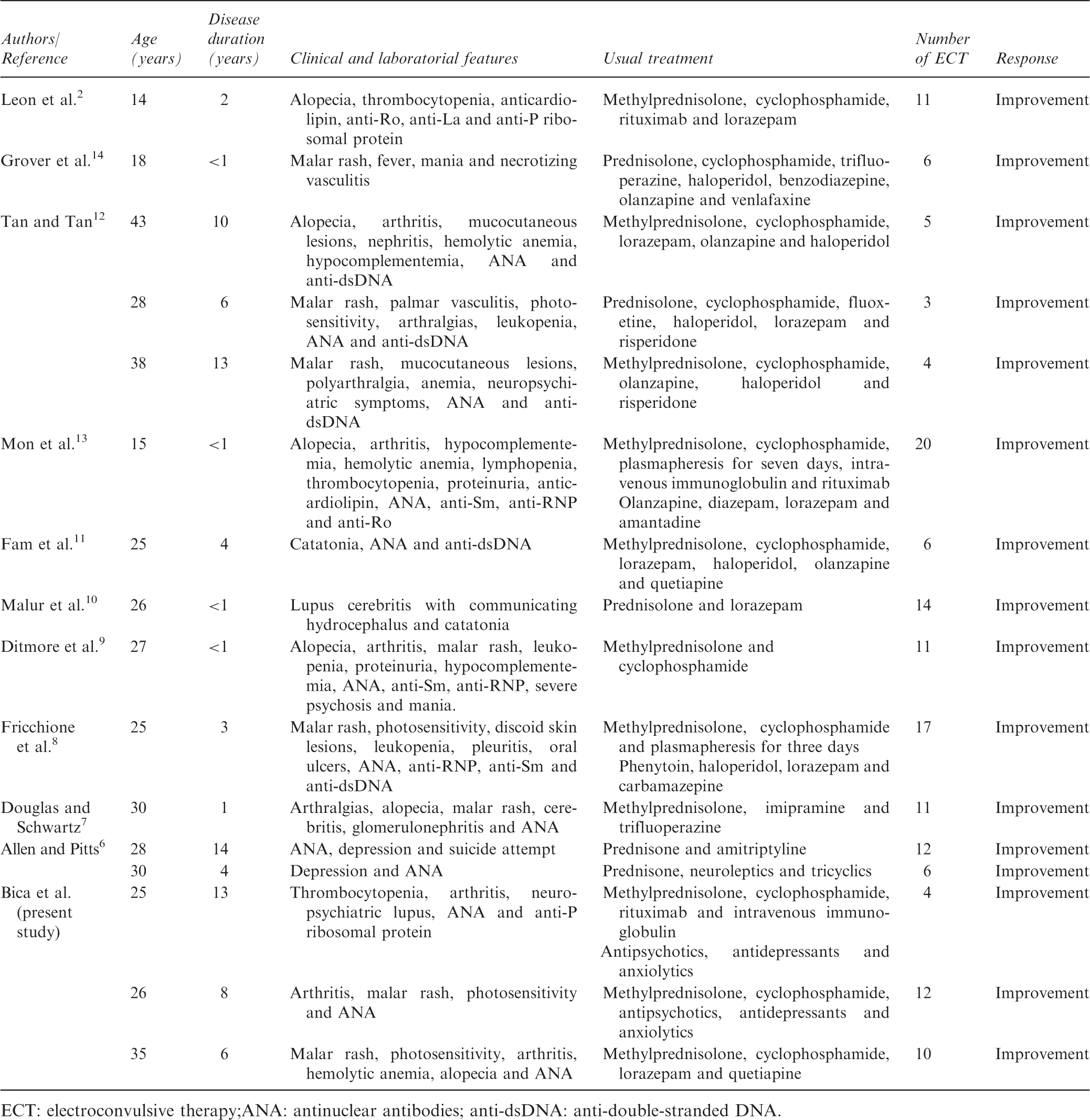
ECT: electroconvulsive therapy;ANA: antinuclear antibodies; anti-dsDNA: anti-double-stranded DNA.
In view of the current literature, neuropsychiatric SLE with catatonia appears to respond satisfactorily to ECT, but these data must be approached with caution because of the likelihood of publication bias (i.e. positive results tend to be published more often than studies with negative results). Despite promising results with the use of ECT, the European League Against Rheumatism (EULAR) recommendations published in 2010 do not include ECT as an alternative treatment for refractory neuropsychiatric lupus. 16 Therefore, we believe that additional studies should be conducted to clarify the role of ECT in the treatment of neuropsychiatric lupus, especially when associated with catatonia.
Conclusion
Severe neuropsychiatric lupus is an unusual manifestation of SLE, but it can have a devastating effect on patient quality of life. In cases refractory to immunosuppressive therapy and antipsychotics, ECT may be considered a safe and promising treatment option.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have no conflicts of interest to declare.