
Abstract
Purpose
Technetium-99m (Tc-99m) thyroid scintigraphy is a well known diagnostic tool that shows the entire gland in a single image. We aimed to evaluate its additive diagnostic value in subclinical autoimmune thyroid disease (S-AITD) in systemic lupus erythematosus (SLE) patients.
Methods
We investigated 100 systemic lupus erythematosus (SLE) patients without overt thyroid involvement (eight men and 92 women; mean age 40±6.5 years) and 50 age and sex matched controls. All were subjected to thyroid evaluation using anti-thyroglobulin (anti-TG) and anti-thyroid peroxidase (anti-TPO) antibodies; hormones (FT3; FT4 and TSH) and Tc-99m thyroid scintigraphy.
Results
14/100 (14%) and none (0%) were positive for S-AITD in SLE and control groups, respectively (P = 0.0001). They were classified by thyroid scintigraphy and hormonal profile into 2/14 Hashimoto; 10/14 atrophic thyroiditis and 2/14 Graves' disease. Anti-TPO was elevated in 12 SLE cases, while anti-TG was elevated in only 2/14 (P = 0.0001). Thyroid scintigraphy showed statistically significant associations with FT4, TSH and anti-TPO.
Conclusion
Tc-99m thyroid scintigraphy may have an additional diagnostic role in S-AITD among SLE patients, with an impact on patient management. This potential needs to be further evaluated in a larger series on a multicenter basis.
Introduction
Autoimmune thyroid disease (AITD), marked by the presence of antibodies directed against thyroid antigens, has been associated with a number of non-organ specific rheumatological disorders. These associations include systemic lupus erythematosus (SLE), Sjögren’s syndrome and giant cell arteritis. 1 A number of studies have suggested that thyroid disease is more common in SLE than in the general population, but there is a disagreement whether both hypothyroidism and hyperthyroidism are more common, or if this finding is restricted only to hypothyroidism. 1 The prevalence of AITD in the general population varies between countries. It has been described as 5%–15% in women and 1%–5% in men, 2 although Helvaci et al. 3 reported that AITD affects about 2%–4% of women and up to 1% of men worldwide, and the prevalence rate increases with advancing age.
Thyroid dysfunction is common in SLE. Many are initially treated for thyroid dysfunction before the diagnosis of lupus is made, or vice versa. 4 Although the relationship between AITD and SLE has been reported to precipitate or exacerbate its symptoms, the prevalence of thyroid disease is controversial. 5 The clinical presentation varies among patients; it can be divided into clinical or subclinical hypothyroidism and hyperthyroidism. 6
Mousa et al.7 found abnormal thyroid functions in 15.9% of SLE patients, and the most common abnormality was clinical hypothyroidism in 8.3%, then subclinical hypothyroidism in 5.3%. However, Assal et al. 8 reported that thyroid dysfunction was detected in 46.6% of SLE patients, and the most common abnormality was subclinical hypothyroidism, followed by clinical hypothyroidism.
Both anti-thyroglobulin (anti-TG) and anti-thyroid peroxidase (anti-TPO) antibodies were found with greater frequency in SLE than in the general population, even in those who do not have clinical thyroid disease.9,10
It is still a subject of discussion whether SLE is an independent risk factor for thyroid abnormalities or this is a coincidental finding, because the group most at risk for SLE – young to middle aged women – is precisely the same group most at risk for AITD. 1 Earlier studies reporting the prevalence of thyroid antibodies and AITD in SLE patients were based on relatively small cohorts of patients except for a few. As a result, the reported prevalence (3.9%–24%) of AITD 4 and frequency (11%–51%) of anti-thyroid antibodies11,12 in SLE varied widely. The survey for AITD in these reports was dependent on thyroid function tests and auto-antibodies (anti-TPO and anti-TG).
By reviewing PubMed up to 2104, no previous studies used Tc-99m thyroid scan in the evaluation of AITD in SLE patients, and only one report, from Argentina, 13 utilized radioactive-131 uptake in such a task in six SLE cases. As is known, thyroid scintigraphy shows the entire gland in a single image and allows direct correlation of clinical findings with abnormalities in the image. 14
In this study we aimed to assess the additive value of Tc-99m thyroid scan in detection of sub-clinical AITD (S-AITD) among SLE patients compared to thyroid hormones and thyroid auto-antibodies (anti-TG and anti-TPO).
Patients and methods
Study population
The study was approved by the local ethics committee of Cairo University scientific review board, and informed consent was obtained from all subjects according to the Declaration of Helsinki, General Assembly, October 2008. The study included 100 SLE patients (92 women, eight men; mean age 40±6.5) and 50 age and sex matched healthy subjects served as a control group (45 women and five men; mean 41±7.3). All patients were recruited from Rheumatology and Rehabilitation Outpatient Clinic of Cairo University Hospitals. All SLE patients in this study fulfilled the American College of Rheumatology (ACR) 1997 revised criteria for the classification of SLE. 15
The exclusion criteria included patients with other autoimmune diseases (other than autoimmune diseases secondary to SLE, such as secondary Sjogren's), known thyroid dysfunction, pregnant or breast feeding patients, those with HCV or interferon therapy, diabetics, patients with cardiac diseases using drugs that could induce thyroiditis such as amiodarone, history of recent CT with iodine containing contrast and smokers. The investigations were done simultaneously for each subject at the time of the study.
Laboratory investigations
The following laboratory investigations were performed:
Free T4 (FT4), free T3 (FT3) and thyroid–stimulating hormone (TSH) serum levels were determined by immunometric assays (Immulite TM 2000 Third Generation, DPC Diagnostic Products Corporation, Los Anglos, CA, USA). Serum anti-TPO and anti-TG antibodies were assayed by the ELISA method supplied by Calbiotech Inc 10461 Austen Dr, Spring Valley, CA, USA.
Tc-99m thyroid scan
Imaging was performed approximately 15 minutes after intravenous administration of 5 mCi (185 MBq) of Tc-99m pertechnetate. The scans were obtained with large field-of-view dual-head gamma cameras (Philips-Axis, Eindhoven, The Netherlands) mounted with a low-energy parallel-hole collimator. All scans were obtained with a 20% energy window centered at 140 keV and a 128 × 128 matrix for 500.000 counts per view. Thyroid percentile uptake was generated by computer assistance (normally 0.3%–4 %). 14
Assessment of Tc-99m thyroid scan
It was carried-out by two nuclear medicine physicians as follows:
○ Thyroid size (average or enlarged). ○ Thyroid uptake percentage (normal or elevated or reduced). ○ Tracer distribution:
□ uniform, or □ heterogeneous, or □ focal absent uptake changes as cold nodule, and faint uptake in whole of the gland. AITD included Graves' disease (diffuse toxic goiter), Hashimoto (auto-immune hypothyroidism) and atrophic auto-immune thyroiditis. Atrophic thyroiditis:
○ Poor tracer uptake by the thyroid gland. ○ High neck background activity. Chronic thyroiditis ( = decompensated dyshormonogenesis) (high TSH, low T3 and T4):
○ High tracer uptake by the thyroid gland. ○ Depletion of neck background activity. Graves' disease: (low TSH, high T3 and T4):
○ High tracer uptake by the thyroid gland. ○ Depletion of neck background activity.
Patterns of autoimmune thyroid dysfunction on TC-99m pertechnetate thyroid scan include:
16
Statistical method
All statistical calculations were done using computer program SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA) version 17 for Microsoft Windows. Data were statistically described in terms of mean ± standard deviation (±SD). Comparison of numerical variables between the study groups was done using t test, paired t test and chi-square test. Linear Correlation Coefficient was used for detection of correlation between quantitative variables in one group. Also, standard linear least-squares regression analysis was used, P-value < 0.05 in the linear regression analysis was considered significant. Bland and Altman’s analysis was referred to agreement between the two methods for independent samples.
Results
This study included 100 patients, 92 (92%) women and eight men (8%). Their ages ranged between 23 and 54 years, with a median of 29 years (mean 40±6.5). The control group included 45 women (90%) and five men (10%). Their ages ranged between 25 and 57 years, with a median of 38 years (mean 41±7.3). 14/100 SLE (14%) patients had AITDs by thyroid scan, where 12/14 were positive for abnormal hormonal profile and auto-antibodies.
Serology
Thyroid hormones
Statistically significant differences were found between FT4 and TSH in patients and controls (
Thyroid auto-antibodies
A statistically significant difference was found between SLE patients and controls regarding anti-TPO (12/100 (12%) vs 0/50;
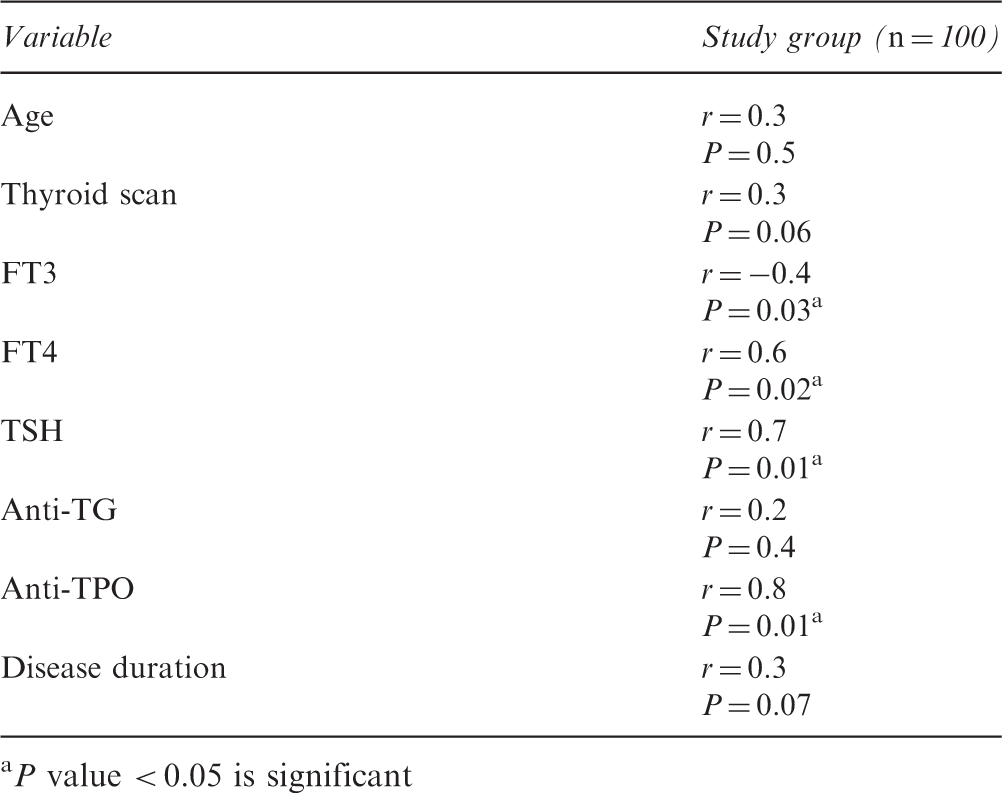
Associations of anti-TPO with some of the demographic and investigational parameters of SLE patients
Tc-99m thyroid scan (Table 2)
Outcomes of Tc-99m pertechnetate thyroid scan, autoantibodies, and thyroid functions in SLE patients

Disease activity score (SLEDAI)
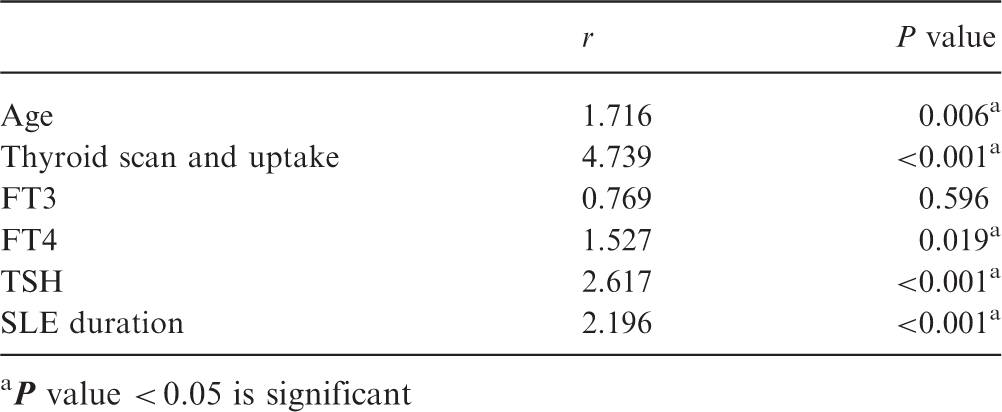
Associations of SLEDAI with some demographic and thyroid investigational data in SLE group.
P value < 0.05 is significant
Discussion
This study was carried out on 100 SLE patients and 50 control subjects. 14/100 (14%) and 12/100 (12%) were positive for S-AITD based on thyroid scan and anti-TPO respectively. The thyroid scan in combination with thyroid hormonal profile showed that 2/14 (2%), 10/14 (10%) and 2/14 (2%) were Hashimoto, atrophic auto-immune thyroiditis and Graves' disease, respectively. Neither hormonal profile nor auto-antibodies could achieve such precise classification of AITD in the studied patients. To our knowledge no previous reports have focused on the value of thyroid scanning for screening of S-AITD in SLE patients.
AITD is a term used to bring together a group of pathologies that have thyroid dysfunction and an autoimmune response against this endocrine organ as their hallmark.17,18 However, being a group of autoimmune diseases clustered together, the clinical presentation varies among these diseases, and can be divided into those inducing hypothyroidism or hyperthyroidism or both. 19 The most clinically relevant anti-thyroid auto-antibodies are anti-TPO directed against the thyroperoxidase enzyme, thyrotropin receptor antibodies (TR-Abs) and thyroglobulin antibodies directed against thyroglobulin protein (anti-TG). Also, anti-sodium/iodide (anti–Na+/I−) symporter antibodies have been reported as a relatively recent discovery and their clinical relevance is still unknown.20,21
On the other hand, autoimmune thyroiditis is often related to non-specific autoimmune organ diseases such as rheumatoid arthritis, SLE or polymyalgia rheumatic. 22 Thyroid disease is often difficult to diagnose clinically in the general population, and could certainly be under diagnosed in SLE patients because of the overlapping symptoms of SLE and thyroid disease. Both SLE and thyroid disorders can cause fatigue, focal edema, weakness, myalgia, arthralgia and a variety of other non-specific complaints. 23
Initially, why did we select SLE patients? Innocencio et al. 24 reported ‘as known there is increased auto-production of antibodies in SLE and thyroid disorders may be the result of one of them’. Also, they stated ‘it is possible that during flares of SLE, elevated interferon levels lead to aberrant major histo-compatibility complex antigen expression by thyrocytes provoking an autoimmune response and the development of anti-thyroid antibodies’.25,26
In the current study, AITD was found in 14% of the studied cases, being 10% atrophic auto-immune thyroiditis, while Hashimoto and Graves' were 2% each. The prevalence of thyroid disorders in Korean SLE patients was studied by Park et al.,
27
and thyroid function was evaluated, where AITD was found to be 14.3% among 63 SLE patients (Hashimoto's thyroiditis (9.5%) and Graves' disease (4.8%)). They concluded that thyroid disease was not uncommon in SLE patients. Also, by comparing our prevalence with other studies (Table 4) the following can be elicited:
A wide range of prevalence of AITD among SLE patients is noted, shooting up to 24% and dropping down to 0%. The overall prevalence of hypothyroidism was higher than that of hyperthyroidism in most of the studies, and this concurs with our findings regarding the elicited forms of thyroid dysfunction. The vast majority of the aforementioned studies relied on thyroid function tests and auto-antibodies. Autoimmune thyroid disease and auto-antibodies among SLE patients in different worldwide studies
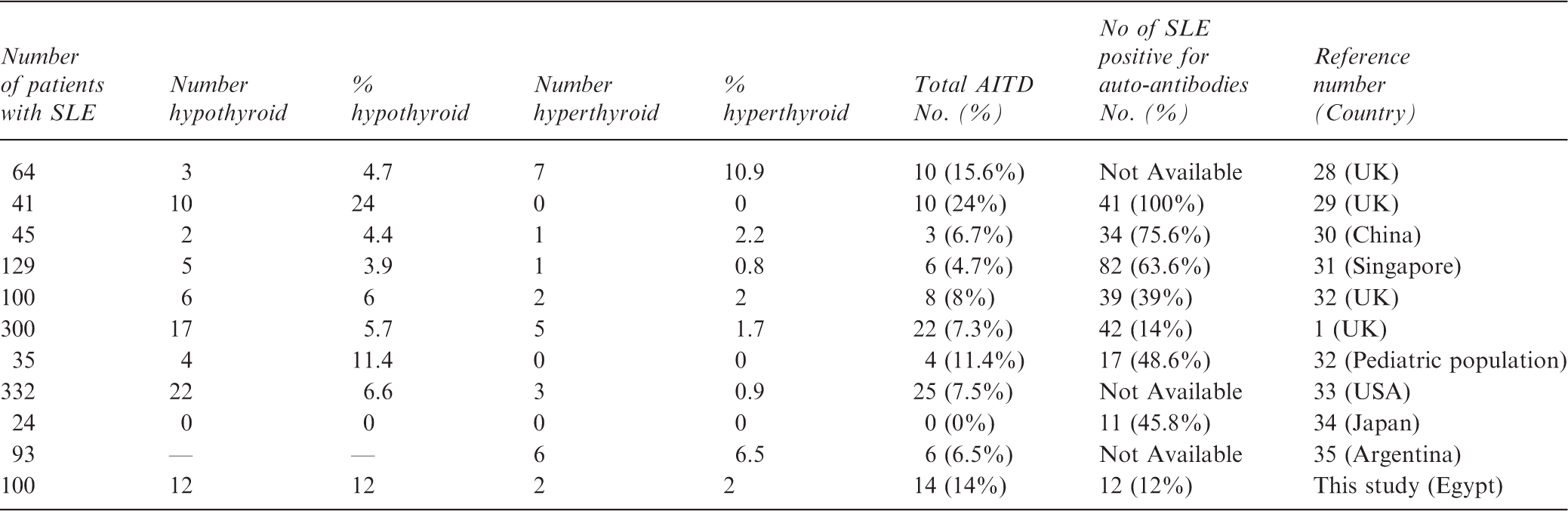
On the other hand, the presence of thyroid auto-antibodies is usually independent of thyroid dysfunction and auto-antibodies could be present even before the development of AITD, as demonstrated in different studies (Table 4):
Pyne and Isenberg
1
showed 22/300 (7.3%) SLE cases had AITD where only 15 (5%) were positive for auto-antibodies. In only 27/300 (9%) thyroid auto-antibodies were found without AITD. The great discrepancies between AITD and auto-immune antibodies in these studies were noted. Contrary to the worldwide reports, auto-antibodies were only found in SLE cases being positive for AITD. Our explanation is quoted from Kohno et al.:
34
‘the over-usage of autoimmune inhibitors’.
The study by Rodrique et al. 35 used radio-active iodine-131 uptake curves at 1, 24 and 48 hours to prove the AITD. It included six SLE patients who had Graves' disease. The latter predated SLE in 3/6 and two had simultaneous SLE and Graves' disease in association. They concluded: ‘It is suggested that hyperthyroidism associated with SLE may be a form of presentation that may pass unnoticed because of the similarity of some clinical manifestations’. Also, Goh and Wang 36 reported 14/319 SLE patients, nine of whom had hyperthyroidism, where, in 8/14, thyroid disease preceded SLE by 1–11 years. It is worth mentioning that in the latter study no evidence-based actual cause was achieved, while in Rodrique et al. 35 study diagnosis of Graves' disease was based on radio-active iodine 131 uptake curves, while we base the diagnosis of AITD subtypes on Tc-99m thyroid scan.
The study by Byron and Mowat 28 reported 10/64 (15.6%) SLE women with AITD (7/64 (11%) and 3/64 (4.7%) had thyrotoxicosis and hypothyroidism, respectively). Among the ten cases, 6/7 (85.7%) and 1/3 (33.3%) predated diagnosis of SLE by 1–17 years. So, rheumatologists must be concerned with AITD, as Graves' or Hashimoto could be the first presentation of auto-immune diseases as SLE. It is now accepted that Graves' disease and Hashimoto's thyroiditis are considered different forms of the same process.37,38
Finally, what is the added value of thyroid scan? This could be determined by emphasizing the following points:
Scan pattern and calculated uptake are of optimal importance as this can differentiate Graves' vs Hashimoto vs atrophic thyroiditis.
14
Activating thyroid receptor anti-bodies is characteristic of Graves' disease. Anti-TPO antibody is measured more easily than other auto-antibodies and used in the diagnostic tree of Graves' disease.
11
Anti-TG are found in 70% of Hashimoto's thyroiditis, 60% of idiopathic hypothyroidism, 30% of Graves' disease, a small proportion of thyroid carcinoma and 3% of normal individuals. Anti-TPO antibodies are present in the majority of Graves' disease, but up to 35% of these cases also demonstrate anti-TG,
20
as was the case in 2/14 (14.3%) of our SLE cases. This overlap makes the reliability of auto-antibodies in the precise diagnosis of AITD among SLE really questionable, so thyroid scan can assist in the differentiation of such an overlap. The scan can provide functional and morphologic information (FMI), and in this study it showed evidence of S-AITD in 14%.
Therefore we make the following suggestions:
A screening algorithm of S-AITD among SLE patient based on thyroid hormonal profile. If the latter is normal nothing further is needed, and if abnormal, then Tc-99m thyroid scan ± auto-antibodies is needed. The scan can diagnose Graves' vs Hashimoto vs chronic atrophic thyroiditis. Thyroid scan can help in achieving a precise etiology of the detected thyroid hormonal changes.
Conclusion
This study showed 14% of S-AITD among Egyptian SLE patients was associated with elevated auto-antibodies and thyroid hormonal changes. Tc-99m thyroid scan might have an additional diagnostic role in such a task in tailoring treatment that is feasible by incorporating the scan into the clinical decision tree; however, these results merit further study in larger SLE series.
Footnotes
Conflicting of Interest Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Acknowledgements
The authors thank Dr Zeinab Nawito for helpful contributions in the finalization of this work regarding grammatical aspects, and Dr Abd Megeed R and Dr Ahmad Abd Alsameea for cordial support.