
Abstract
Neutrophils are implicated in a wide range of non-infectious inflammatory conditions. A subset of neutrophils in the peripheral circulation of systemic lupus erythematosus (SLE) patients has been described and termed low density granulocytes (LDGs). This study investigates the expression of LDG in juvenile-onset SLE (JSLE) patients compared to controls, and any correlations with disease activity.
Neutrophils and LDGs were isolated from JSLE (n = 13) and paediatric non-inflammatory control patients (n = 12). Cell populations were assessed and compared using flow cytometry and morphological analysis. Standard clinical data, which included disease activity markers/scores, were collected for each patient.
Significantly increased LDG expression (%mean ± SEM, range) was observed in JSLE patients (10.4 ± 3.26, 3.41–36.3) compared to controls (2.4 ± 0.44, 0.36–5.27; p = 0.005). A statistically significant positive correlation was observed between LDG expression and the British Isles Lupus Activity Group (correlation coefficient 0.685; p = 0.010) and SLE Disease Activity Index (correlation coefficient 0.567; p = 0.043) and the biomarker of dsDNA-antibodies (correlation coefficient 0.590; p = 0.043).
Here we observe increased expression in LDGs in JSLE patients, which correlate with dsDNA antibody concentration and scores of disease activity. These correlations indicate that the increased LDG expression observed in this study may have a potential role in the pathogenesis of JSLE, and may be a useful biomarker.
Introduction
Neutrophils are one of the first cell types to be recruited to the sites of inflammation or infection. However, neutrophils have been implicated in a wide range of non-infectious inflammatory conditions, 1 and associated with increased propensity towards apoptosis in many autoimmune diseases, where, in view of their numbers, they pose an enormous apoptotic burden potential. Defects in processing and removal of apoptotic neutrophils can contribute significantly to autoimmune disease development. 2 Recent evidence also suggests that increased neutrophil extracellular trap (NET) formation, or insufficient dismantling of them, can lead to breaking of tolerance and the promotion of autoimmunity. 3
Juvenile-onset systemic lupus erythematosus (JSLE) is a systemic autoimmune disease, characterized by inflammation and loss of tolerance to nucleic acid-binding antigens. The presence of autoantibodies raised against nuclear autoantigens correlate closely with disease activity and is of diagnostic and prognostic value. 4 JSLE has a wide spectrum of major clinical manifestations affecting any organ.
Genomic approaches analysing peripheral blood mononuclear cell (PBMC) gene expression profiling of children with SLE have shown neutrophil-specific genes to be the second most prevalent PBMC gene expression signature, and the differential expression of these genes correlates with disease activity. 5 It is speculated that this signature is due to the presence of low density granulocytes (LDGs) in the blood, which reflects early neutrophil release from the bone marrow. 6 The aim of this study was to measure the expression of LDGs in JSLE patients compared to controls, and any correlations with disease activity.
Material and methods
Patients and controls
This study was approved by Liverpool Paediatric Research Ethics Committee. Written informed patient/parental assent/consent were obtained from all participating subjects. All JSLE patients fulfilled the revised American College of Rheumatology (ACR) criteria for the diagnosis of SLE 7 before the age of seventeen. Paediatric non-inflammatory controls, defined as children investigated for non-inflammatory musculoskeletal symptoms or attending for elective surgery where no inter-current infection was present. All paediatric patients were recruited from outpatient clinics and inpatient wards at Alder Hey Children’s NHS Foundation Trust, Liverpool, UK. Clinical data and laboratory results were blinded to all investigators until final experiments were completed.
Cell preparation
While mature neutrophils typically sediment with the red blood cell fraction in a Ficoll-density gradient, LDGs co-purify in the PMBC fraction. Neutrophils and LDGs were isolated from fresh heparinized blood by one-step centrifugation through Polymorph prep (Axis Shied UK) or Histopaque gradient, respectively (following the manufacturer’s instructions). Contaminating erythrocytes were removed by hypotonic lysis. Purity and morphological analysis were performed of cytospin preparation. Purified neutrophils and lymphocytes were re-suspended at a concentration of 1 × 106 cells/ml in RPMI1640 medium (Sigma Aldrich). Cell populations were assessed using flow cytometry following staining with PerCP-cy5.5 labelled CD15 antibody as a marker for neutrophils.
Light microscopy
Isolated JSLE and control neutrophils and LDGs (5 × 104) were centrifuged onto a microscope slide at 500 g for five minutes and stained using Romansky staining (HD supplies). The morphology was assessed and visualized using light microscopy techniques.
CD15 staining
LDGs can be distinguished from monocytes by flow cytometry by their high expression of CD15. Isolated JSLE and control neutrophils and LDGs were pelleted and re-suspended in 0.5% BSA PBS. The cells were washed using centrifugation and incubated with either 5 µl PerCP-Cy™5.5 Mouse Anti-Human CD15 antibody or 5 µl PerCP-Cy™5.5 Mouse IgM, κ Isotype Control (BD Biosciences) and left on ice for 30 minutes. Cells were washed and analysed by flow cytometry (FC 500 mpl; Beckman Coulter).
Clinical data
Standard clinical data which included disease activity markers/scores were collected for each patient. This data included Erythrocyte Sedimentation Rate (ESR), C-reactive protein (CRP), complement C3 and C4 levels, dsDNA titres, Childhood health assessment questionnaire score and physician’s global score and British Isles Lupus Assessment Group (BILAG) score.
Measurements
Statistical analysis was performed using the Friedman nonparametric test for multiple-related groups. If a significant value was obtained (p < 0.05), further statistical analysis was carried out on the data. For unrelated groups, the Mann–Whitney test was performed. Spearman’s rank correlation coefficient was used to assess any correlations between disease activity markers and LDG expression.
Results
Patient demographics
Thirteen JSLE patients were studied at a mean age of 15 (range 7–17) years old; 12 (92%) were female. Nine were white British, one Pakistani, one Asian and two Arab. Twelve paediatric non-inflammatory controls were studied with mean age of 12.9 (range 7–17) years old of whom seven (58%) were female and all were white British. Patients had a range of disease activity at the time of sampling (British Isles lupus activity group (BILAG) 2004 score, mean 4.7 (range 0–19); SLE disease activity index (SLEDAI) score, mean 6.81 (range 0–25)), and were on a range of standard disease-modifying agents used to treat them, which included nine (69%) on hydroxychloroquine, eleven (84%) on either Azathioprine or Mycophenolate and four (31%) on steroids.
Significantly increased LDG expression in JSLE patients
LDGs were isolated directly from fresh heparinized blood, stained with CD15 and assessed using flow cytometery (Figure 1(a)–(c)). The neutrophil population were assessed first, and location on the forward and side scattered noted. Any CD15+ cells isolated using histopaque within this gated region were considered LDGs. Increased LDG expression (%mean ± SEM, range) was observed in JSLE patients (10.4 ± 3.26, 3.41–36.3) compared to controls (2.4 ± 0.44, 0.36–5.27; Figure 1(d): p = 0.005). A cytospin was prepared for each population of cells isolated, and images taken using a light microscope following Romanowsky staining (Figure 1(e)). Cells that displayed a neutrophil morphology were clearly visible.
Low density granulocytes (LDGs) were isolated directly from fresh heparinized blood, stained with CD15 and assessed using flow cytometery (a–c). The neutrophil population were assessed first, and the population of cells gated (a). Any CD15+ cells isolated using histopaque within this gated region were considered LDGs ((b,c) grey filled; unstimulated, dotted line; isotype control, light grey line; cells isolated with histopaque, dark grey line; neutrophils). Increased LDG expression (%mean ± SEM) was observed in JSLE patients compared to controls, (d); p = 0.005. A cytospin was prepared for each population of cells isolated and images taken using a light microscope following Romanowsky staining (e). Cells that displayed a neutrophil morphology were clearly visible (white arrows).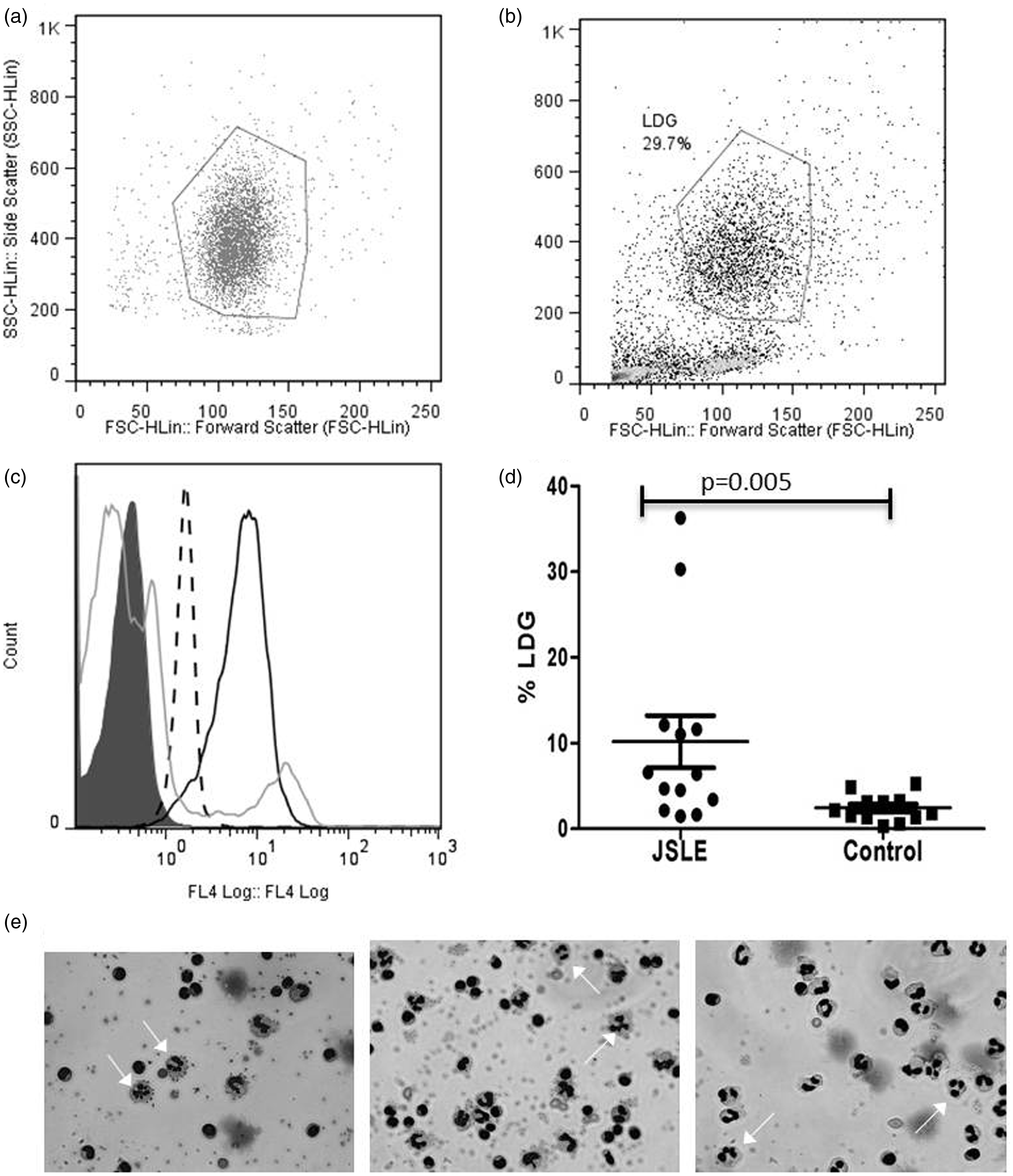
LDG expression correlates positively with disease activity scores
A statistically significant positive correlation was observed between LDG expression and disease activity indices BILAG (correlation coefficient 0.685; p = 0.010) and SLEDAI (correlation coefficient 0.567; p = 0.043) and the biomarker of dsDNA-antibodies (correlation coefficient 0.590; p = 0.043; Figure 2(a)).
Standard clinical data was collected for each patient. Spearman’s rank correlation coefficient was used to assess any correlations between disease activity markers and low density granulocyte (LDG) expression. A positive correlation was observed between LDG expression and disease activity indices BILAG, ((a); p = 0.010) and SLEDAI ((a); p = 0.043) and the biomarker of dsDNA-antibodies ((a); p = 0.043). LDG expression was measured in a JSLE patient (10064) before (10064a) and after treatment (10064b; (b)). A reduction of LDG expression was observed as well as a decrease in disease activity indices BILAG, SLEDAI, dsDNA-antibodies and global assessment score (GA).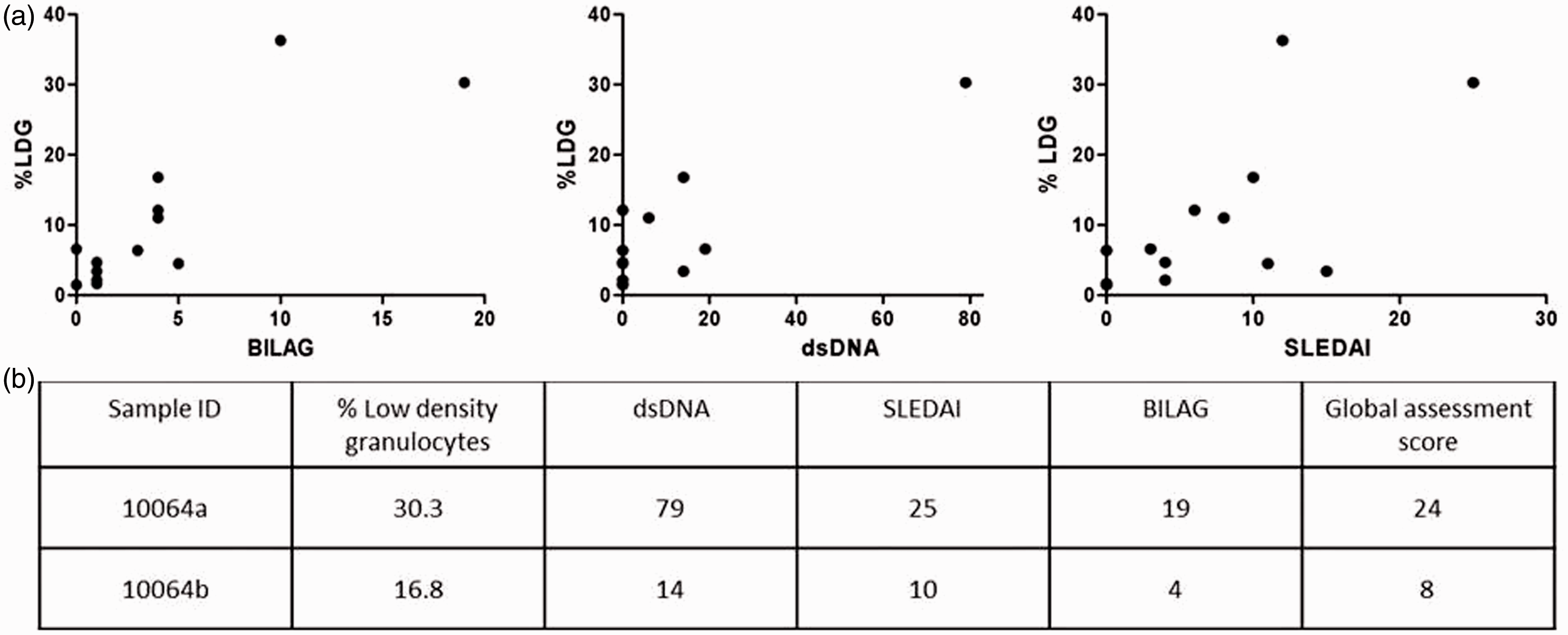
The percentage of LDG expression decreases after treatment
LDG expression was measured in a JSLE patient (10064) before and after treatment (Table 1, Figure 2(b)). A reduction of LDG expression was observed, as well as a decrease in disease activity indices such as BILAG, SLEDAI, dsDNA-antibodies and global assessment score (GA).
Discussion
Here we observe increased expression in an abnormal subset of neutrophils in JSLE patients, which correlate with dsDNA antibody concentration and scores of disease activity. A study in adults with SLE showed that, compared to control neutrophils or to autologous, normal-density lupus neutrophils, LDGs show enhanced capacity to express type I IFNs following stimulation. 8 IFN-α is well recognized to be a key player in SLE pathogenesis. As already mentioned, gene expression profiling of PBMCs from JSLE patients have been analysed, and, as well as having a transcriptional signature corresponding to neutrophil-specific genes, a type I IFN genetic signature has also been observed. 5 Increased IFN-α has been observed in the serum of SLE patients, which correlates with disease activity; 9 this increase could in part be due to increased expression of LDGs in SLE patients, as observed in this study. Understanding the pathways leading to enhanced type I IFN production by LDGs is still an important area of research which needs to be further characterized.
Elimination of microbes by neutrophils can occur through a number of regulated processes, one of which is the formation of NETs. 10 NETs are composed of granule and nuclear constituents such as DNA and histones. In addition to their antimicrobial role, recent evidence suggests that NETs may also have a potential role in externalizing auto-antigens and activating the adaptive immune system. 11 LDGs have been shown to have an enhanced capacity to form NETs, 11 and netting neutrophils have been proposed as strong inducers of IFN-α synthesis by pDCs,11,12 thereby supporting the role of LDGs in the pathogenesis of SLE. As a group we have observed increased NET formation in neutrophils isolated from our paediatric lupus patients compared to controls, which is increased following incubation with JSLE serum. 13
Interestingly, a study from a cohort of adult SLE patients has shown that SLE serum in a subset of patients had an impaired capacity to degrade NETs, and that impaired NET clearance was associated with lupus nephritis. 14 The presence, therefore, of LDGs in patients that have a reduction in their ability to clear NET material could result in prolonged exposure of nuclear self antigens, which could lead to the development of autoantibodies that correlate closely with disease activity. 4
As well as other systemic autoimmune diseases,6,9 low density granulocytes have also been documented in other conditions such as HIV infections 15 and, more recently, asthma. 16 Although there are increasing studies looking at LDGs, the developmental stage of LDGs and the mechanisms driving their synthesis in SLE remains unclear. Thus, investigating the morphology and characteristics of LDGs will help determine whether LDGs represent a distinct population of neutrophils with specific disruptions in neutrophil development, or a more activated subset.
In conclusion, future characterization and identification of specific LDG markers may prove useful in assessing their roles in tissue damage in lupus and other diseases. This study supports the presence of a distinct subset of neutrophils in JSLE patients, and that their expression correlates with disease activity. Further longitudinal studies are needed to assess if LDGs could potentially be used as biomarkers or predictors of disease activity in patients with JSLE. These investigations would further elucidate the role of the innate immune system in the pathogenesis of autoimmune diseases, and may also give insight into novel therapeutic strategies or drug targets.
Footnotes
Acknowledgments
We are thankful to all those who participated in this study. We would like to also thank Olivia Lloyd, Dr Eileen Baildam, Dr Gavin Cleary, Dr Liza McCann and Dr Claire Pain, as well as all others who helped to recruit paediatric patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Alder Hey Children’s NHS Foundation Trust, Lupus UK, Arthritis Research UK, Alder Hey Children’s Charity and the NIHR CRN: Children’s Theme.