
Abstract
Background
New oral anticoagulants may simplify long-term therapy in conditions requiring anticoagulation. Rivaroxaban is a direct factor Xa inhibitor that has been extensively studied and is now approved for the prevention and therapy of a number of thromboembolic conditions.
Objective and methods
This is a multicentre, randomized, open-label, study that will evaluate if Rivaroxaban 20 mg od (or 15 mg od in patients with moderate renal insufficiency) is non-inferior to warfarin (INR target 2.5), for the prevention of thromboembolic events, major bleeding and death in high risk (triple positive) patients with antiphospholipid syndrome. Secondary endpoints will assess the incidence of any individual component of the composite end point. An external adjudication committee will evaluate all suspected outcome events. This will be a unique trial, as it will enrol the biggest homogenous cohort of high risk APS individuals.
Conclusion
The methods and the study design should be appropriate to achieve study results that are both scientifically valid and relevant to clinical practice.
Introduction
Antiphospholipid syndrome (APS) is an acquired autoimmune disease characterized by thrombosis-related clinical disorders or pregnancy morbidity in the presence of antiphospholipid antibodies (aPL). 1 APS has a high socio-economic burden: it affects young individuals, causing thrombosis in virtually every organ, and leads often to pregnancy loss. Clinical features of APS are commonly encountered in clinical practice, thus the diagnosis of APS is totally based on laboratory findings exploring the presence of antiphospholipid antibodies (Lupus anticoagulant (LA), anti-cardiolipin (aCL) antibodies and anti-ß2-Glycoprotein I (aß2GPI) antibodies). 2 Patients at highest risk for thrombosis and recurrence are those displaying triple positivity (triple-aPL patients) in the laboratory tests.3–9 Oral anticoagulant therapy significantly reduces thromboembolic recurrences in thrombotic APS. 9 The mainstay of anticoagulation therapy in APS are vitamin K antagonists, the management of which is challenging. The narrow therapeutic window makes strict monitoring the key to successful therapy particularly in patients with APS, to avoid treatment failure. In one study, 10 half of the recurrences in APS patients occurred when INR was below therapeutic range. Major bleeding is also a concern among APS patients, with an annual occurrence of 1.5%–2%.10,11 An oral anticoagulant that requires no monitoring and has a predictable anticoagulant effect would be of great interest, given the characteristics of APS patients. The new oral anticoagulant rivaroxaban, an inhibitor of factor Xa, is at least as effective as warfarin in preventing venous 12 and arterial thromboembolism,13,14 and displays an even safer profile, significantly reducing cerebral bleeding. 13 With its once a day administration it improves compliance.
The Trial on Rivaroxaban in Thrombotic Antiphospholipid Syndrome (TRAPS) is a phase III randomized trial (ClinicalTrials.gov Identifier: NCT02157272) which will assess the safety and efficacy of rivaroxaban compared with the usual care.
Study objectives and hypothesis
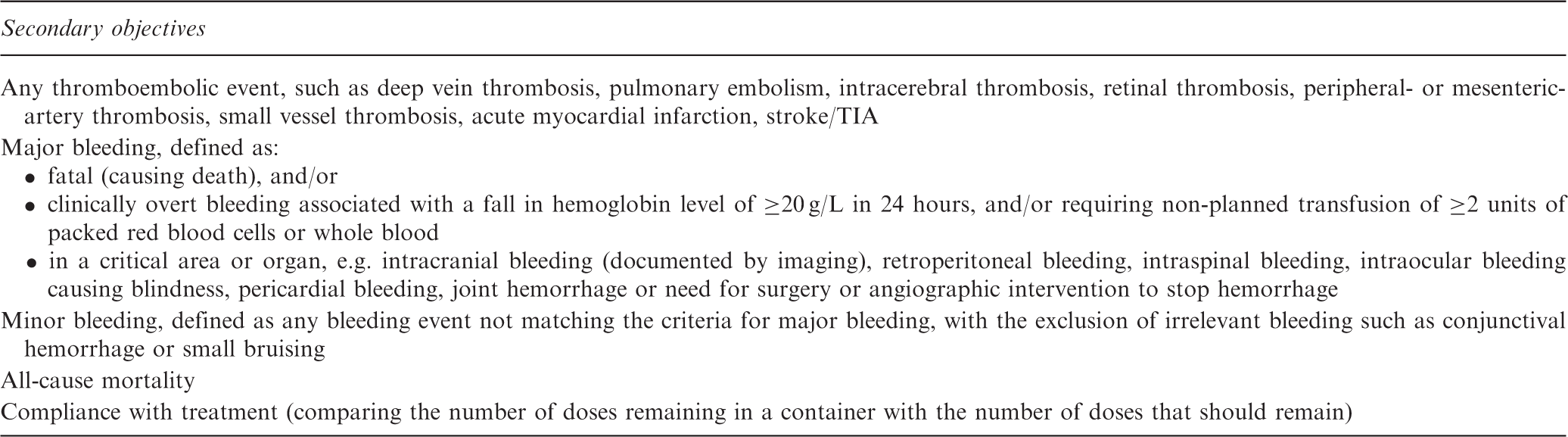
Detailed summary of the secondary objectives of the TRAPS trial
Study design
Overview
This is a multicentre, randomized, controlled, open-label, non-inferiority study. The protocol was reviewed and approved by the Institutional Review Board at each centre. The study is coordinated by a steering management committee. An adjudication committee, whose members are unaware of treatment allocation, reviews all suspected episodes of recurrent thromboembolism, bleeding and death.
Patient population and eligibility
Inclusion and exclusion criteria
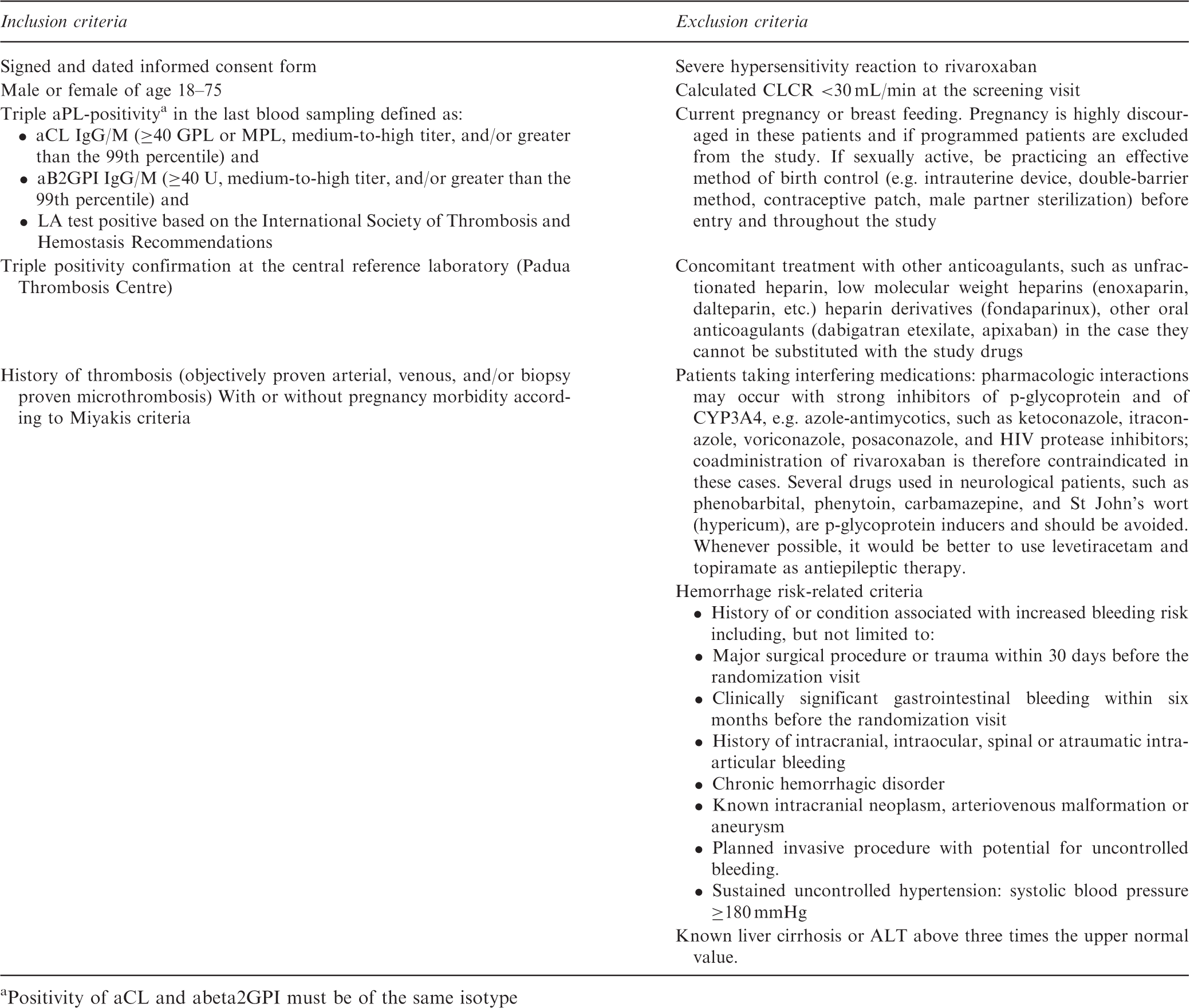
Positivity of aCL and abeta2GPI must be of the same isotype
Stratification and randomization
In each of the participating institutions, after obtaining written informed consent, all potential patients will be screened before enrolment in the study. The screening visit includes patient’s confirmation of triple laboratory positivity for aPL (i.e. positivity for LAC, aCL and B2GPI) and confirmed diagnosis of thrombotic APS. Moreover, a series of laboratory tests are performed during the screening visit. These include complete blood count, renal and liver function and standard coagulation tests. Randomization and study data will be collected and managed using REDCap (Research Electronic Data Capture) 15 electronic data capture tools hosted at the Department of Cardiac Thoracic and Vascular Sciences, Padua University Hospital. Randomization will extend over a two-year period. The investigator will enter the screening information into the web-based management system, which randomly assigns the patient to warfarin or rivaroxaban, with a 1:1 allocation using random block sizes of two, four and six, and stratified on the basis of gender and the presence/absence of previous diagnosis of an autoimmune disease. When in warfarin, patients will be switched to rivaroxaban when INR is below 3.
Rivaroxaban regimen and rationale
Rivaroxaban is a direct oral factor Xa inhibitor with a high oral bioavailability (≥80%) and predictable pharmacokinetics and pharmacodynamics, that does not require routine coagulation monitoring. It has a fast on–off anticoagulation effect and is associated with few drug–drug or drug–food interactions. 16 Rivaroxaban is approved for the treatment of DVT/PE and secondary prevention of VTE. This approval is backed by the results of the EINSTEIN phase III clinical programme that investigated the use of rivaroxaban as a single-drug approach in contrast to the current dual-drug paradigm of enoxaparin/VKAs.12,17 In EINSTEIN DVT, not only rivaroxaban was shown to be non-inferior to enoxaparin/VKA, but also was associated with a reduction in major bleeding (EINSTEIN PE) and a significantly improved net clinical benefit. Rivaroxaban is also approved for primary and secondary stroke prevention13,18 in nonvalvular atrial fibrillation. The ROCKET-AF trial showed non-inferiority to VKA treatment, and there were significantly fewer intracranial bleeds. 13
Based on these results, rivaroxaban 20 mg once daily was approved for the treatment of all patients with Cockroft–Gault determined creatinine clearance (CrCl) >50 ml/min. For CrCl of 30–50 ml/min rivaroxaban 15 mg should be administered.
Warfarin regimen
Warfarin is the mainstay of therapy for the prevention of thromboembolism (arterial or venous) in APS. 19 The real challenge is to maintain the appropriate anticoagulation intensity. Based on a retrospective study, higher intensity anticoagulation (target INR of 3.5) was initially considered. 20 However, two subsequent prospective randomized trials10,11 have demonstrated that high-intensity was not superior to moderate-intensity anticoagulation (target INR 2.5). Thus, currently APS patients are treated with moderate intensity anticoagulation, and these patients will be included in the TRAPS trial. The initial warfarin dose is determined using the protocol 21 endorsed by the Italian Federation of Anticoagulation Clinics (FCSA). The subsequent warfarin doses are adjusted to maintain the INR within the range of 2.0–3.0, aiming for a target of 2.5. INR is checked at least every four weeks, or more frequently if needed, at the investigator's discretion.
Duration of study treatment
End of treatment is set after four years from the start of the trial, or when 88 events have occurred. Every effort will be made to avoid loss of follow up to patients. Study treatment may be temporarily stopped if clinically needed, and anticoagulation will be managed according to published guidelines.16,22 The treatment will be resumed as soon as possible, when deemed clinically appropriate.
In the case of study drug discontinuation, follow-up, including assessment of any clinical event, will be pursued. The reasons for premature discontinuation of investigational products will be recorded. The use of aspirin is allowed according to physician discretion, in both arms.
Primary outcomes
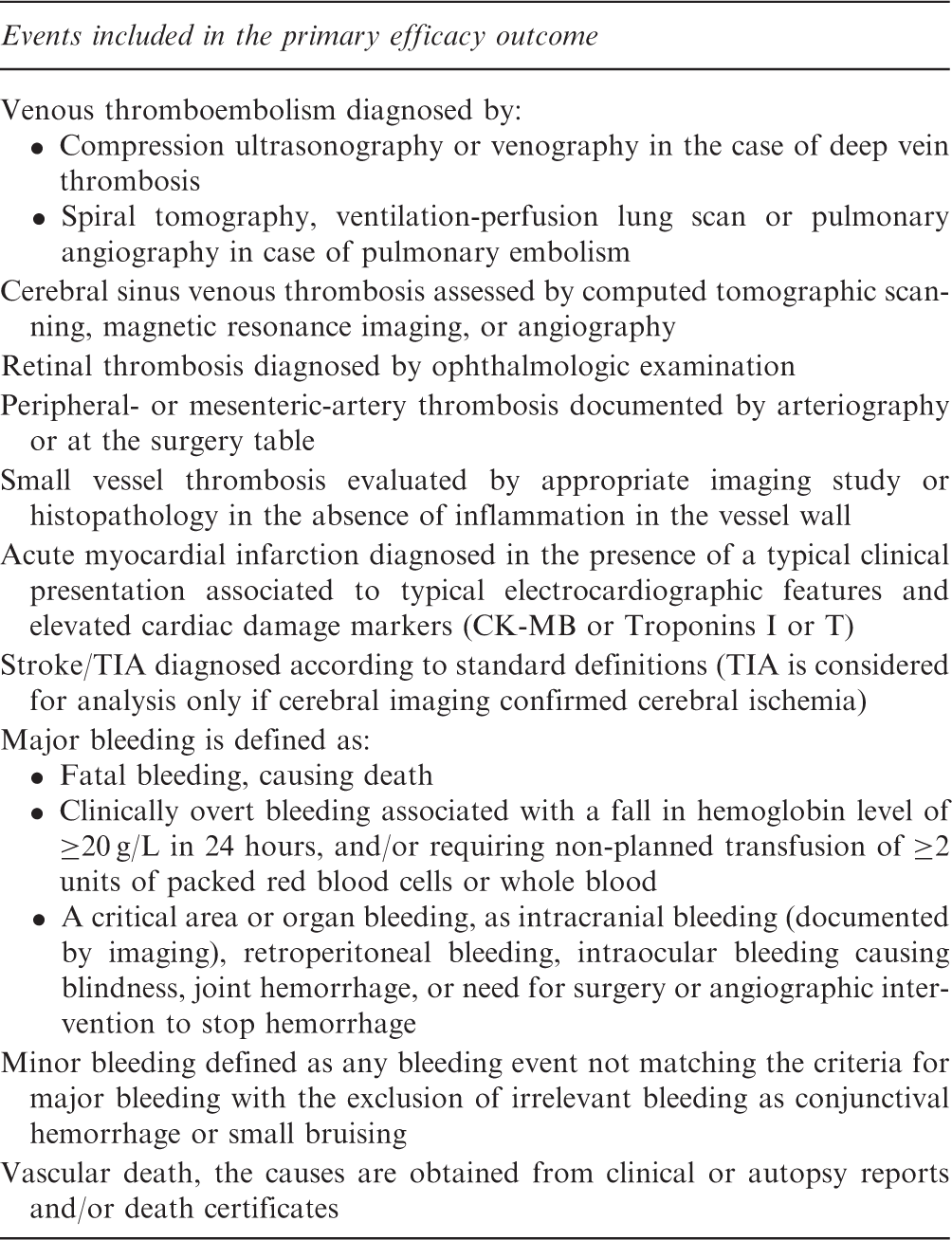
Detailed summary of the primary outcomes of the TRAPS trial
Secondary outcomes
The secondary outcomes are divided into efficacy and safety endpoints. The secondary efficacy endpoint will be any single type of thromboembolic event taken separately and all causes of mortality. The secondary safety outcome will be major bleeding; minor bleeding will also be assessed as a secondary endpoint. The definitions of the outcomes are provided in Table 3.
Assessment of outcomes and follow-up
All patients will have regularly-scheduled hospital visits at one and three months after enrollment, and every six months thereafter. Extra visits will occur in the event of thromboembolic events or major bleeding. Compliance and vital signs will be checked by phone contact every three months until the end of treatment. Hospital visits will check CrCl (every six months), liver function, complete blood count, PT-INR, adverse events, compliance with the treatment and incidence of end-points, and will re-supply medication. The trough determination of anti Xa activity in rivaroxaban group will be performed at steady state in each patient.
Sample size and statistical analysis
The primary analysis was designed to test whether rivaroxaban is non-inferior to warfarin. The non-inferiority margin is set to correspond to the preservation of 50% of the warfarin effect, as adopted in the other rivaroxaban registration trials. The non-inferiority margin is derived from the only observational study considering VKAs versus control in triple positive APS patients. 9 This study suggests a rate of composite events (thrombosis, major bleeding and death) among APS patients receiving warfarin of approximating 6% per year. On the other hand, the incidence of events in untreated patients is 13%per year. The hazard ratio margin corresponding to preservation of 50% of the warfarin effect is 1.7. To satisfy the non-inferiority hypothesis, the upper bound of the one-sided 95% confidence interval for the hazard ratio of an outcome with rivaroxaban as compared to warfarin must fall below 1.7. A non-inferiority log-rank test with an overall 88 events and sample size of 536 subjects (268 in the reference group and 268 in the treatment group) achieves 80% power at a 0.05 one tail significance level to detect an equivalence hazard ratio of 1.7. The study will last four years, with recruitment limited to the first two years and follow up extended to four years.
Discussion
Most if not all studies in APS patients have included patients with different laboratory profiles, providing cohorts of poor homogeneity.10,11,20,23 The present trial promises to be the biggest trial assessing a homogenous cohort of APS patients. Triple positive APS patients are at high risk of recurrent thromboembolic events 9 with a stable aPL pattern. 24 Patients with APS receive indefinite anticoagulation based on VKAs. Given the characteristics of APS, patients an alternative to VKAs that is safe, effective and does not require monitoring would be of great benefit.
To this end, rivaroxaban has been approved for the prevention and treatment of DVT and PE, with an excellent efficacy profile. On the other hand it was non-inferior to warfarin in the setting of stroke prevention in non-valvular atrial fibrillation in patients at high thromboembolic risk (CHADSVASc > 3). It was also approved for the secondary prevention of acute coronary syndrome. 14 Under these premises, rivaroxaban should be a suitable agent for the prevention of thrombotic recurrences in APS.
In conclusion, TRAPS will be the biggest randomized controlled trial assessing the efficacy and safety of a novel anticoagulant, rivaroxaban, in the setting of APS. It will include a laboratory homogenous cohort of high-risk APS patients. The results from this study may indicate the standard care and improve our understanding on APS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.