
Abstract
Objectives
To study the effects of a one-year physical activity programme on aerobic capacity, physical activity and health-related quality of life (HRQL) in patients with systemic lupus erythematosus (SLE) by a randomized control design.
Methods
Thirty-five women with low or moderate disease activity and organ damage were randomized to intervention (I) or control (C) group. The intervention during months 0–3 consisted of education, supervised aerobic exercise at high intensity and individual coaching, as well as self-managed physical activity at low-to-moderate intensity. During months 4–12, the physical activity was self-managed and the coaching was successively reduced over time. Outcome measures included: maximal oxygen uptake (VO2 max) from a bicycle ergometer test, self-reported physical activity and HRQL (SF-36).
Results
VO2 at sub-max. and max. increased, independent of group, during the one-year study period (main effect of time p < 0.0001). VO2 max. increased between baseline and month 3 (p < 0.0001), between months 3 and 6 (p = 0.01) and the increase was sustained at month 12 (ns). Frequency of physical activity at high intensity also increased, independent of group, during the study period. It was increased at months 3, 6 and 12 compared to baseline (p = 0.02, p < 0.001, p = 0.03). Improvement in mental health between baseline and month 6 (p = 0.002) was seen for the I-group, not the C-group (p = 0.03). Disease activity and organ damage did not change.
Conclusions
Physical activity and aerobic capacity increased after supervised exercise and coaching, and the improvement was sustained during the one-year programme. However, no interactions between the group differences were seen, which suggests that repeated measurements could motivate to increased physical activity and thereby to increased aerobic capacity. As sub-max. VO2 increased over time, training-induced changes in VO2 on-kinetics could be another explanation. Little influence on HRQL was seen after the programme. The study indicates that physical activity at high intensity over one year is tolerated by patients with mild to moderate SLE.
Keywords
Introduction
Systemic lupus erythematosus (SLE) increases the risk for cardiovascular diseases (CVD), which has particularly been recognized as a long-term consequence in women with SLE.1–3 Low aerobic capacity and low physical activity are both risk factors for CVD.4–10 Patients with SLE have low physical and aerobic capacity11–15 and a low level of physical activity compared to controls.1,3,16,17 In addition, patients with SLE also have reduced health-related quality of life (HRQL).18,19
Regular physical activity of at least moderate intensity is associated with numerous physical and mental health benefits in the general population. Furthermore, all-cause mortality is delayed by regular physical activity, and so is the risk of developing coronary heart disease.4–10,20–22 Volkman et al. 23 have shown that low physical activity is related to increased atherosclerosis and high-density lipoprotein in patients with SLE. Others have reported that physically active patients with SLE have vascular function as healthy people, and it has been suggested that regularly physical exercise in SLE can influence vascular function through modification of the systemic inflammation.24–27 Aerobic training at moderate to high intensity combined with muscle strength training for three months have been reported to have a positive effect on heart function and to influence the regulation of the heart rate through the autonomic nerve system. 28
Supervised physical exercise for 12 weeks in patients with SLE improved aerobic capacity as reported in a clinical controlled study. 29 A single-subject experimental design supported these results. 30 However, there are few randomized controlled trials (RCTs), and the results concerning the effects on aerobic capacity from physical exercise programmes for 8–12 weeks with little or no supervision are contradictory.31,32 Furthermore, long-term studies on the effects of physical exercise on aerobic capacity in patients with SLE are lacking. Supervised physical exercise for 12 weeks in patients with SLE has also improved HRQL such as fatigue.29,30,33 The effects on HRQL from exercise with little or no supervision are less convincing here.12,31–33
As supervised physical exercise for long time periods is expensive it is an advantage if patients can manage their long-term physical activity and exercise on their own.17,34–37 Optimal methods to stimulate and maintain physical activity with minor or no supervision are therefore important.38–42 Behavioural change-based exercise interventions, supervision by an experienced fitness instructor and performing exercise that is enjoyable can improve adaptation and adherence to prescribed exercise programmes. 6 Coaching has been found effective in supporting people to increase their physical activity, for people in general38,43 as well as in rheumatic conditions.37,39,41 There are few studies that have evaluated ways of how to stimulate and maintain physical activity for longer periods in patients with SLE.32,35
The aim of this study was to evaluate the effects of a one-year physical activity coaching programme, with successively reduced support over time, on aerobic capacity, physical activity and HRQL in patients with SLE.
Patients and methods
Design
This is a single-blinded RCT evaluating the effects of a physical activity programme for patients with SLE. Most measurements were made at baseline, month 0 (after 2–3 weeks) and months 3, 6 and 12.
Participants
Women who were regularly followed at the Department of Rheumatology at Karolinska University Hospital, Solna, Stockholm, Sweden, and who fulfilled at least four of the American College of Rheumatology (ACR) criteria for SLE 44 were invited to participate. Baseline data, inclusion and exclusion criteria have previously been described. 15 In addition, the patients should also have a haemoglobin value ≥100 g/L, s-creatinine ≤ 300 μmol/l, diastolic blood pressure ≤100 mm Hg at rest, stable prednisolone dose ≤15 mg/day, the ability to follow instructions and to perform a maximal bicycle ergometer exercise test, in order to be included. Also, patients who had complications from cerebrovascular disease, arthroplastic complication/surgery or pregnancy during the time of the study were excluded.
Of the 220 patients with SLE who were regularly followed at the time for the study, 128 women fulfilled the criteria and were invited by letter to participate (for more details see our earlier study
15
). Forty women volunteered and were examined by a rheumatologist, performed a bicycle ergometer exercise test and filled out questionnaires at baseline. After examination and performance of the baseline exercise test, five patients were excluded as they did not fulfil the criteria for the study: exercising too much (n = 1), newly discovered atrial fibrillation (n = 1), electrocardiogram (ECG) changes indicating cardiac involvement (n = 1), high blood pressure (n = 1) and a low haemoglobin value (n = 1) (Figure 1).
Flow diagram of the patients with SLE in the intervention and control groups during the one-year study period.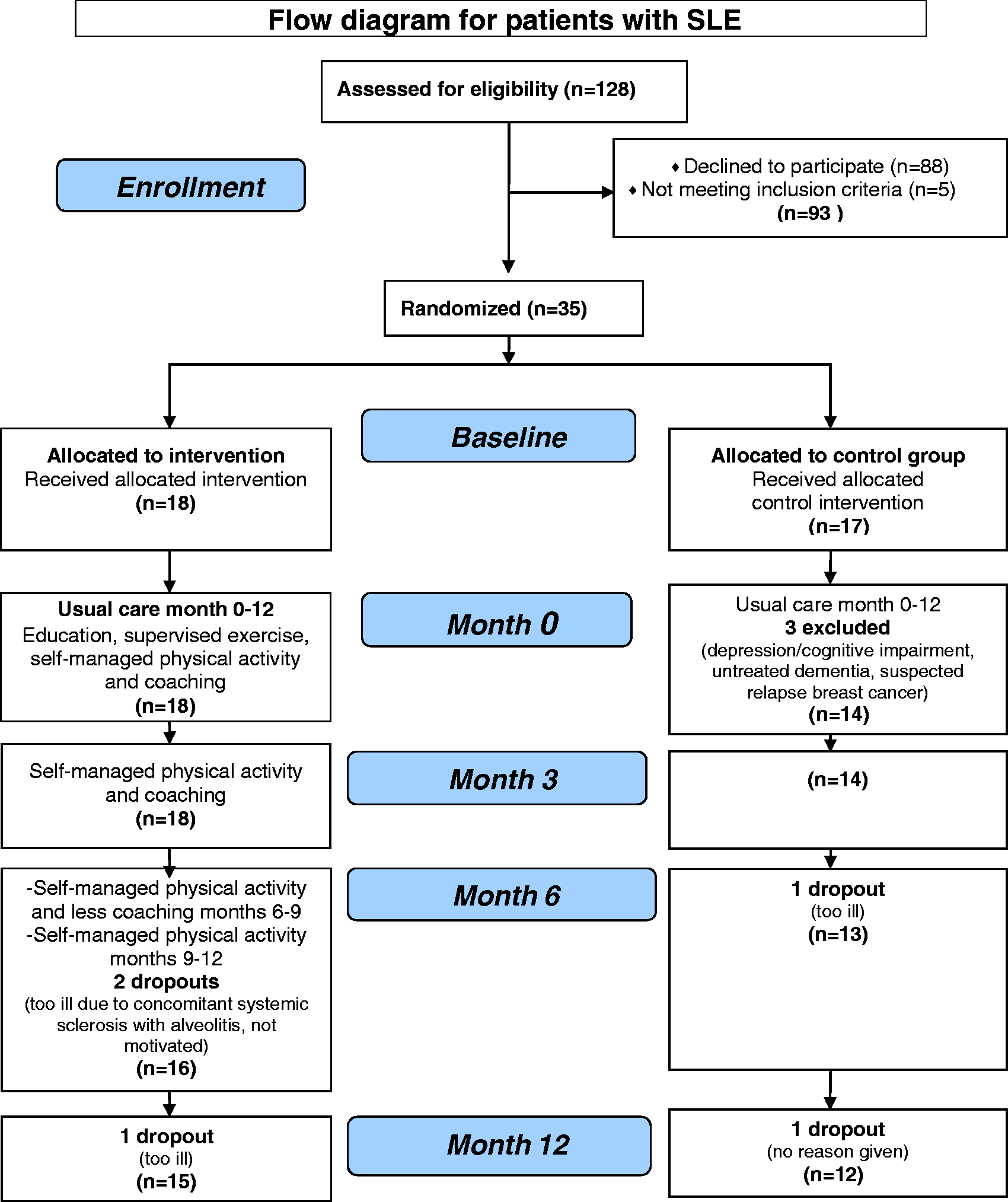
The remaining 35 patients were block-randomized, by a statistician not involved in the study otherwise, into an intervention group (I-group, n = 18) or a control group (C-group, n = 17) (Figure 1). The stratified computer-based randomization procedure distributed patients equally into the two groups with respect to maximal oxygen uptake (VO2 max), from the exercise test. The result of the randomization was concealed until interventions were assigned. The mean age at baseline in the I-group was 52 (SD 10) years and in the C-group 53 (SD 9) years. The disease duration was 15 (SD 9) years in the I-group and 21 (SD 14) years in the C-group, and the number of ACR-criteria was mean 5.5 (SD 1.6) in the I-group and 5.4 (SD 1.2) in the C-group. The patients in the I-group had the following comorbidities: Sjögren's syndrome (n = 9), hypertension (n = 6), antiphospholipid syndrome (n = 2), systemic sclerosis (n = 1), pulmonary fibrosis (n = 1) (no symptoms the previous six months), hip joint prosthesis (n = 1) and polyneuropathy (n = 1). The corresponding data for the C-group were: Sjögren's syndrome (n = 6), hypertension (n = 3), antiphospholipid syndrome (n = 4), diabetes mellitus (n = 2), mixed connective tissue disease (n = 1), previous heart valve surgery (n = 1), hip joint prosthesis (n = 1) and asthma bronchiale (n = 2).
Intervention and control group
Patients in both the I-group and the C-group received their usual care at the rheumatology clinic during the study. The rheumatologists and other professionals involved in the usual care of the patients were not informed about which group the patients were assigned to. All patients were informed about the aim of the study, and that physical exercise might have positive effects on physical fitness and health for patients with SLE.
The patients in the C-group were asked not to change their physical activity lifestyle during the study period. Otherwise they were not given any specific information related to the study.
Physical activity programme for the intervention group
The physical activity programme had an approach inspired by social cognitive theory.45–47 However, the programme was not based on any single existing behaviour theory or model, and coaching was pragmatically defined. 48 Similar programmes in patients with rheumatoid arthritis (RA) have been evaluated in Sweden.48,49 The programme was organized into two periods, months 0–3 (more supervised); and months 4–12 (less supervised), to initiate and support self-managed physical activity (Figure 1). The first three months of the programme consisted of: education, supervised aerobic exercise, individual coaching of physical activity, loan and use of heart rate monitor and the use of a physical activity diary. Between months 4 and 9 the programme consisted of individual coaching of physical activity, use of heart rate monitor and the use of the physical activity diary, and finally between months 9 and 12 the programme included only the use of the heart rate monitor and the use of the physical activity diary. It was one and the same care provider (CB) for the I-group during the whole study.
The patients were to successively increase their physical activity during the programme to achieve: (1) high intensity, ≥30 min per session, 2–3 days per week and (2) low-to-moderate intensity, ≥30 min per session, 4–5 days per week. 6 High intensity was defined as scoring 13–16 on the Ratings of Perceived Exertion (RPE) scale, 6–20 (RPE scale), 50 corresponding to 65%–80% of maximal heart rate, 6 and low-to-moderate defined as scoring 9–12 on the RPE scale, corresponding to 45%–60% of maximal heart rate. 6 The patients were asked, for physical activity at high intensity, to strive for 16 on the RPE scale and for low-to-moderate intensity to strive for 12.
Months 0–3
At the beginning of the first three months the patients were informed about the disease, the risk for cardiovascular disease, the treatment of the disease and the importance of, and how to perform, physical activity and exercise. A one-hour education session was held on one occasion each by a rheumatologist (IEL) and a physiotherapist (CB), respectively. The physiotherapist also informed the patients how to use a heart rate monitor, to assess intensity according to RPE-scale and how to document physical activity in a physical activity diary. The patients were informed how to document the modes, the frequencies, the durations and the intensities of their physical activity and also their experiences from being physically active. Each patient had access to a heart rate monitor during the whole study period.
Participation in a supervised aerobic exercise group at high intensity, for 60 min, two days per week was offered. The group exercise consisted of mainly aerobic exercises (approximately 20 min) and muscle strength and endurance training (approximately 15 min). The patients could alternatively choose any preferred self-managed high-intensity physical activity, as some of the patients lived far from the hospital. The physical activity at low-to-moderate intensity was self-managed and consisted of any type of preferred physical activity. One of the goals of the exercise group was to successively get started with the high-intensity physical activity and to be encouraged to continue exercising, throughout the year, possibly together in small groups.
Half an hour of individual coaching for physical activity was given at the study start and after 6 and 12 weeks. The support comprised a discussion between the physiotherapist and the patient, and consisted of guidance about how to increase and stay physically active. The results from the exercise tests were focused on, as were the patient's self-reported motivation, possibilities and barriers to physical activity. Pros and cons with physical activity and self-efficacy to increase physical activity were included in the discussion. Furthermore, how to cope with risk situations for not being physically active according to the goals, like bad weather, possible negative consequences from being physically active, like pain and fatigue, and low motivation, was discussed. Individual physical activity goals were set up for the next support occasion, which were later evaluated and adjusted if necessary. Documentation in the physical activity diary was also discussed.
Months 4–12
During this period the physical activity was self-managed with the help of videotapes and/or sound cassettes from the high-intensity aerobic group exercise programme performed during the first three months. As an alternative, any physical activity at high intensity could be chosen. This was also the case for physical activity on low-to-moderate intensity. Individual coaching, with almost the same structure as during the first three months, was offered for half an hour, at months 6 and 9. Focus lay on the results from the exercise tests, notes in the physical activity diary and evaluating and adjusting individual goals. The patients also received telephone support, for approximately 10 min, and the frequency of this was successively reduced during the 4–12 months period, as follows: months 4–6, every third week; months 7–9, once per month; 10–12, no support.
Measurements
The assessments throughout the study were performed by professionals who were blinded to which group the patient had been randomized to. The outcome variables aerobic capacity, physical activity and HRQL were measured at baseline (more details in Boström et al. 15 ) at month 0 (2–3 weeks after baseline when the intervention started) and after 3, 6 and 12 months. To control for any adverse effects of increased physical activity, disease activity and organ damage were registered as well as pharmacological treatment.
Aerobic capacity
Aerobic capacity, measured as maximal oxygen uptake (VO2 max), was the primary outcome variable. To measure VO2 max. is the most accurate way to estimate aerobic capacity. Each patient was to perform a maximal symptom-limited, bicycle ergometer exercise test with online measurement of oxygen uptake (VO2) and carbon dioxide elimination (VCO2).51,52 The patients were encouraged to continue to maximal exertion, but the test was discontinued when they indicated exhaustion. In addition to VO2 max, VO2 at a submaximal load corresponding to 60% and 80% of the maximal work load (max. watt) that each individual reached at baseline (VO2 at 60% and 80% of max. watt) was measured. VO2 and VCO2 during the exercise test were measured with the Oxycon gas analyser (Alpha version 4.5, Jaeger, KFA-2028-01), including mouth-piece and nose-clip. The VO2 variables were expressed as litres per minute (L/min) and millilitres per kilogram body weight per minute (mL/kg/min).
Max. watt and exercise test duration, max. time, were also registered from the exercise test. ECG was continuously monitored, heart rate was recorded and blood pressure was measured 10 minutes before, during and up to 10 minutes after the exercise test. During the test, systolic blood pressure was measured at the end of every second minute, maximal heart rate was registered and maximal systolic blood pressure was measured on termination of the exercise test.
To estimate the voluntary effort during exercise, test exertion was assessed according to the RPE-scale at the end of the exercise test, and age-expected maximal heart rate (220-age) 51 and maximal respiratory exchange ratio (RER) was calculated. RER describes the quotient between VO2 and VCO2 and is frequently used in maximal exercise tests as a marker to identify voluntary effort. RER ≥ 1.1 is considered as maximal effort. 51
Physical activity
Physical activity was a secondary outcome variable defined as all kinds of activities such as housework, gardening, walking, dancing or regular physical exercise that increase heart rate and exertion levels.6,53 Two self-reported questions concerning previous frequency of physical activity were used. The question for high intensity was as follow: How often have you been physically active at high intensity, at least 30 minutes? 15 The question concerning low-to-moderate intensity was similar. The five answer alternatives for both questions were: ‘never or irregularly’; ‘once a week’; ‘2–3 times per week’;’ 4–5 times per week’; and ‘6–7 times per week’. The patients answered the same questions at all measurement occasions; however, for baseline and month 0 the time interval was ‘the past 6 months’ and for months 3, 6 and 12 the time interval was the ‘past 3 months’. Similar questions concerning physical activity in patients with SLE have been found to have satisfactory to good test–test reliability and content validity. 54
Health related quality of life
Measurement of HRQL was another secondary outcome variable. The Swedish version of the Medical Outcomes Study 36-Item Short-Form Health-Survey (SF 36),55,56 the ‘standard’ version, was used to measure HRQL at baseline, month 0 and at month 12, while the ‘acute’ version was used at months 3 and 6. The two versions differ in how far backwards in time the patients have to take into consideration when answering the questions (one week and four weeks, respectively). There is no problem concerning validity in comparing the different versions according to the developers of SF-36. 56 The possible score for each of the eight subscales is 0–100; the higher the score, the better the function. Aspects of the reliability and validity of SF-36 on patients with SLE have been presented by several authors. 57
Disease activity, organ damage and pharmacological treatment
Disease activity was measured at baseline and month 0 and months 3, 6 and 12. Overall disease activity was assessed according to a modified version of Systemic Lupus Erythematosus Disease Activity Index (SLEDAI), 58 from which levels of complement and anti-DNA antibodies were excluded. This gave a score range 0–101, and the higher the score, the higher the overall disease activity. The Systemic Lupus International Collaborating Clinics/ACR-Damage Index (SLICC) was used to assess overall organ damage at months 0, 6 and 12. 58 Its score range is 0–46, where 0 indicates no damage and 46 worst damage. The dose for prednisolone or equipotent glucocorticoid was registered at all measurement occasions.
Procedures
One rheumatologist (BD) examined the patients, assessed disease activity and organ damage and recorded the pharmacological treatment. 15 A nurse took blood tests, collected urine samples (for assessment of SLEDAI and SLICC), measured weight and height and administered the questionnaires. The blood tests included erythrocyte sedimentation rate, C-reactive protein, full-blood count and serum creatinine level. The majority of the patients completed the two physical activity questions and SF-36 the same day or within one week of the visit to the rheumatologist. The exercise tests were administered by biomedical technologists. A physician analysed and interpreted the results of the tests. The majority of the patients did the exercise test the same day or within one week of the visit to the rheumatologist.
Ethics
The study was approved by the local ethics committee at the Karolinska Institute Research Ethical Committee North at Karolinska Hospital, Stockholm, Sweden and informed consent was obtained from each study participant.
Statistics
Before statistical analysis, the five answer alternatives for physical activity were merged into three categories for high intensity (answer alternatives 2–3, 4–5 and 6–7 times/week merged), and four categories for low-to-moderate intensity (4–5 and 6–7 times/week merged) in order to more easily describe how many patients that reached the goal of each intensity, that is, ≥2–3 times/week for high intensity and ≥4–5 times/week for low-to-moderate intensity. Each of the questions in the subscales in SF-36 was divided into three or four categories, based on quartiles, tertiles or the classes possible in the subscale (emotional role function and physical role function).
In order to analyse the ordinal data between baseline and months 0, 3, 6 and 12, the variables physical activity, SF-36, SLEDAI and SLICC (months 0, 6 and 12) were fitted to a generalized estimating equations (GEE) model with the Genmod procedure in SAS®. Exertion according to RPE-6-20 scale and the dose of prednisolone (three classes of dose) were also analysed with this model. The model was set up with the within-groups factor ‘time’ (five or three time points) and the between-groups factor ‘group’ (intervention, control) and the interaction ‘group × time’.
The interval and ratio data VO2 max, VO2 at 60% and 80% of max. watt, max. watt and max. time were analysed using the procedure Mixed in SAS®. Heart rate, blood pressure, RER, body weight and BMI (no values from month 12), were also analysed using this procedure. Repeated measurements were analysed with data from five visits (baseline and month 0, 3, 6 and 12) for body weight and BMI four visits (baseline and month 0, 3 and 6). The within groups factor in the model was ‘time’ (five or four time points) and the between groups factor was ‘group’ (intervention, control) and the interaction ‘group × time’.
The group × time interaction in the GEE and mixed model refers to the statistical test of whether the response profile for one group is the same as for the other group. In case of a significant interaction, simple effects were tested, that is, effects of one factor holding the other factor fixed. The parameter estimates from the GEE models are presented as odds ratios (OR) and 95% confidence interval (95% CI) for SF-36, and χ 2 for physical activity. Estimated means and 95% CI from the mixed model are presented for oxygen uptake, max. watt, max. time and heart rate. The GEE and mixed model strategy is a useful approach for repeated measurements analysis of outcomes in a longitudinal study. All patients who had data from at least one sampling time point measurement were included in the statistical analyses. Problems caused by missing data for one or more time points do not arise when fitting models in Mixed- and Genmode procedures, provided that the missing data can be assumed missing at random. All patients were analysed in their randomized groups according to the intention-to-treat principle.
Statistical comparisons between baseline and month 0 were performed for all outcome variables (data not shown), except for SLICC. No significant differences were found. Only baseline values, not values from month 0, are presented in the results. p ≤ 0.05 was considered statistically significant. The software used: SAS® System 9.1, SAS Institute Inc., Cary, USA for Mixed- and Genmode Procedures and Statistica 7.1, StatSoft®, Inc. Tulsa, USA.
Results
Participants
Descriptive data from the exercise test at baseline in patients with SLE in the intervention and control groups
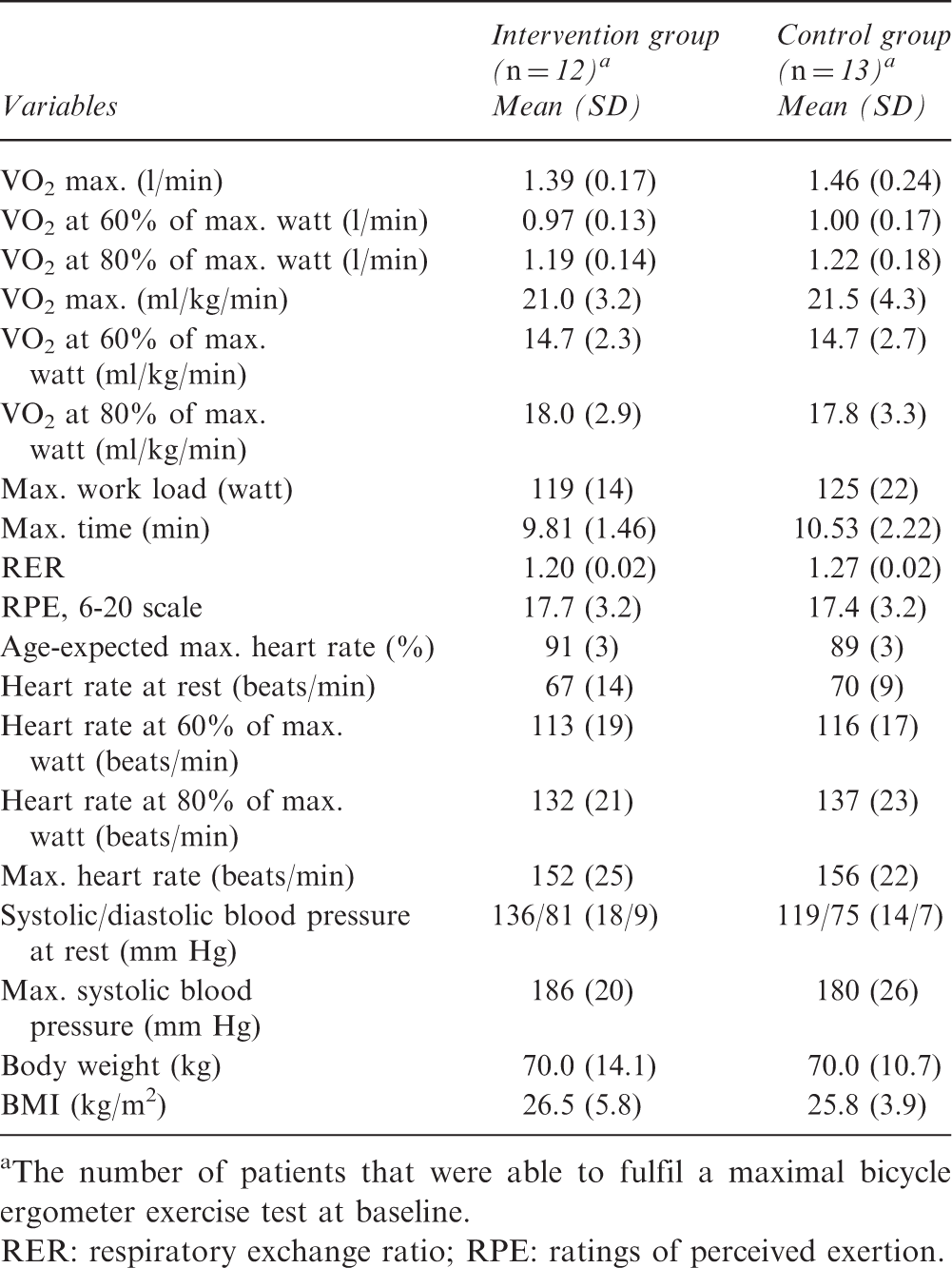
The number of patients that were able to fulfil a maximal bicycle ergometer exercise test at baseline.
RER: respiratory exchange ratio; RPE: ratings of perceived exertion.
Aerobic capacity
At baseline, 12 patients in the I-group and 13 in the C-group could perform a maximal ergometer exercise test with recorded oxygen uptake (Table 1). During the study period, three patients in the I-group at 1–4 test occasions did not fulfil all maximal exercise tests, and in one patient oxygen uptake could not be registered at 3/5 occasions. In the C-group, four patients at 1–2 test occasions did not fulfil all maximal exercise tests.
VO2 max. (l/min) increased independent of group (main effect of time p < 0.0001) during the study period (Table 2, Figure 2). There were no significant differences in VO2 max. (l/min) between the groups at baseline and during the one year study period (interaction group × time, p = 0.20) (Table 2). Post-hoc analysis showed that VO2 max. increased between baseline and month 3 (p < 0.0001) and between months 3 and 6 (p = 0.01). Between months 6 and 12 the values were sustained (p = 0.83). Expressed in per cent (calculated from estimated means from mixed model) VO2 max. (l/min) increased 16% in the I-group and 9% in the C-group between baseline and month 3; between baseline and month 6 the increase was 21% in the I-group and 17% in the C-group; and between baseline and month 12 the increase was 21% and 16 %, respectively (Table 2, Figure 2). A similar pattern was also seen for changes in max. VO2 related to body weight (ml/kg/min) (Table 2). For max. watt and max. time there were no significant main effects of time or group and no interactions group × time (Table 2).
Maximal oxygen uptake (VO2 max., l/min), and oxygen uptake (VO2) at 60% and 80% of max. watt from the baseline values, in the intervention and control groups over the one-year study period. The number of participants at baseline that could perform a maximal exercise test was n = 12 in the intervention group and n = 13 in the control group. The number of subjects varied during the different time points, but all individuals included were analysed by Procedure Mixed statistical analysis. Estimated means and 95% confidence intervals from the Mixed Model analysis are shown. Outcome variables from the exercise test at baseline, months 3, 6 and 12 in patients with SLE in the intervention (I) and control (C) groups, expressed as estimated values
a
, and statistical outcomes for the changes over the one-year study period Estimated means and SE=standard errors from Mixed Procedure. The number of subjects varied during the different time points, but all individuals included were analysed by Procedure Mixed statistical analysis. VO2 max.: Maximal oxygen uptake; max=maximal.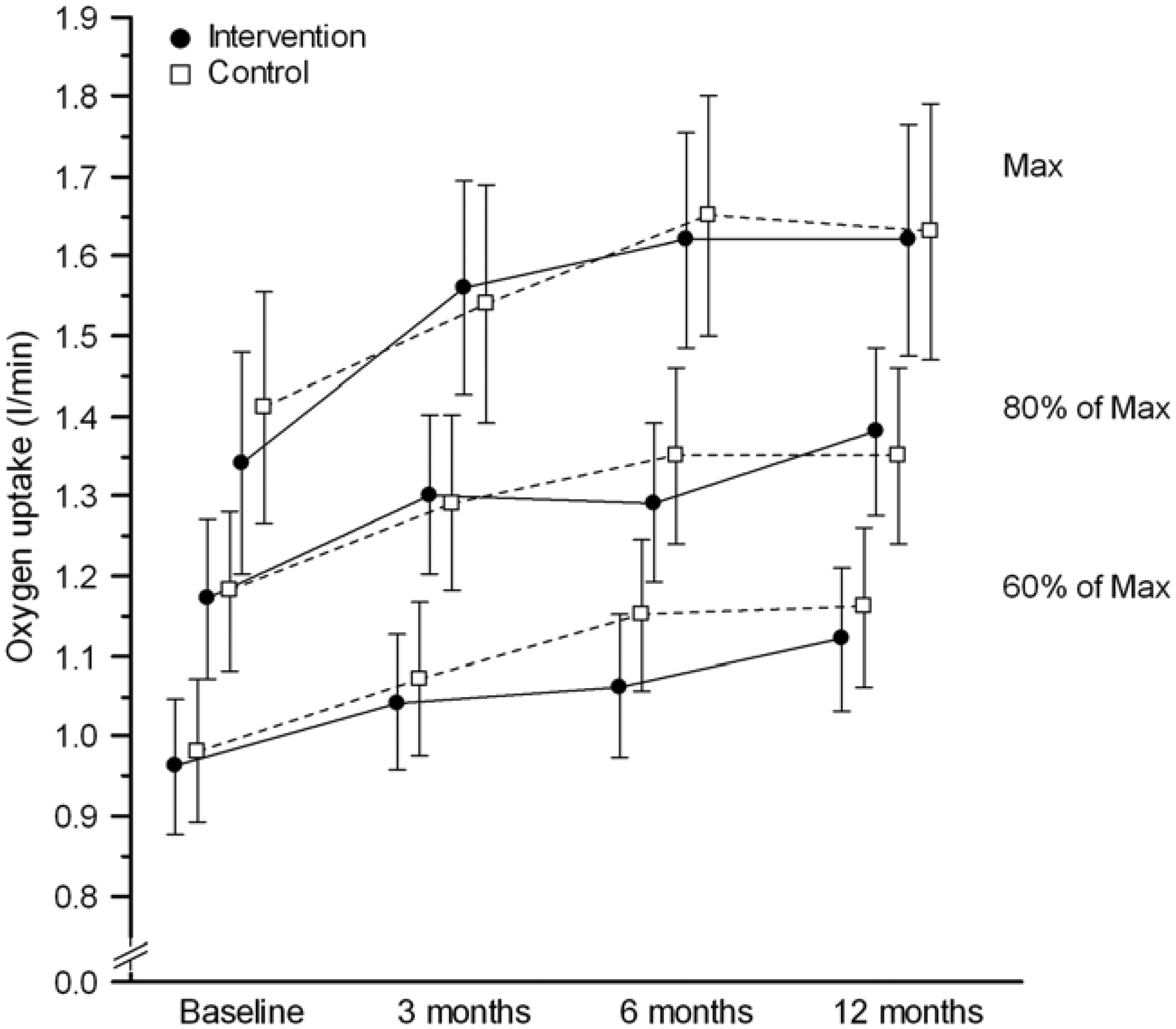
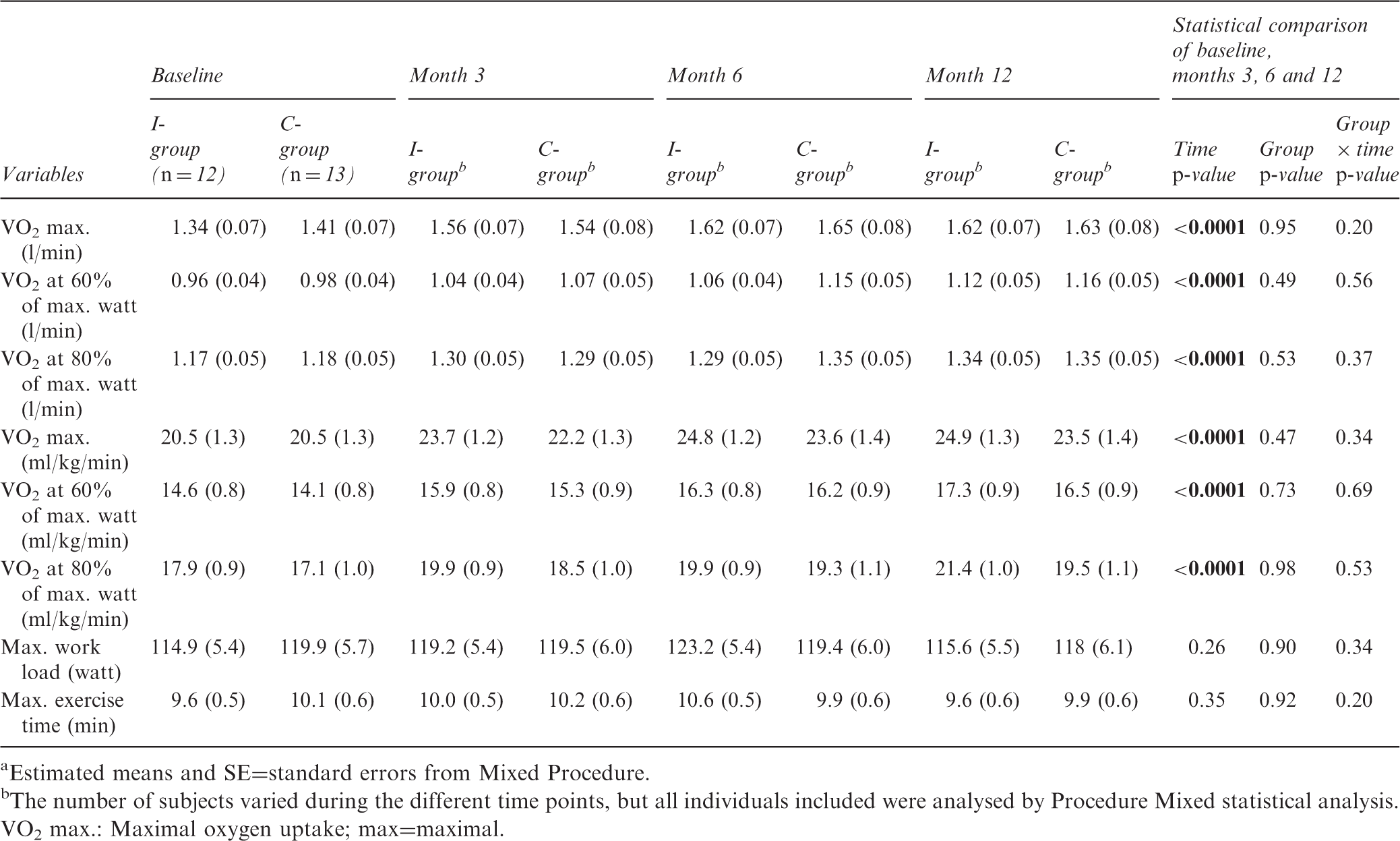
There were no significant differences between the groups concerning submaximal VO2 (l/min) at 60% and 80% of max. watt at baseline and during the one year study. However, during the study period, the submaximal VO2 (l/min) at 60% and 80% of max. watt increased, independent of group (main effect of time, p < 0.0001) (Table 2, Figure 2). Expressed in percent the increase during the study period was between 10% and 15%. A similar pattern for submaximal VO2 related to body weight (ml/kg/min) was seen (Table 2).
There were no significant differences between the groups at baseline and during the one-year study period concerning maximal heart rate (main effect of time p = 0.68). However, independent of group, an increase over the study period was found for heart rate at rest (main effect of time p = 0.04), heart rate at 60% of max. watt (main effect of time p = 0.002), and heart rate at 80% of max. watt (main effect of time p = 0.0004) (Figure 3). For blood pressure at rest and maximal systolic blood pressure there were no significant main effects of time or group or interactions group × time. Calculations without the four patients with beta-blockers showed similar results for both heart rate and blood pressure as when they were included (data not shown).
Heart rate at rest, at 60% and 80% of max. watt from the baseline values, and maximal heart rate in the intervention and control groups over the one-year study period. The number of participants at baseline that could perform a maximal exercise test was n = 12 in the intervention group and n = 13 in the control group. The number of subjects varied during the different time points, but all individuals included were analysed by Procedure Mixed statistical analysis. Estimated means and 95% confidence intervals from the Mixed Model analysis are shown.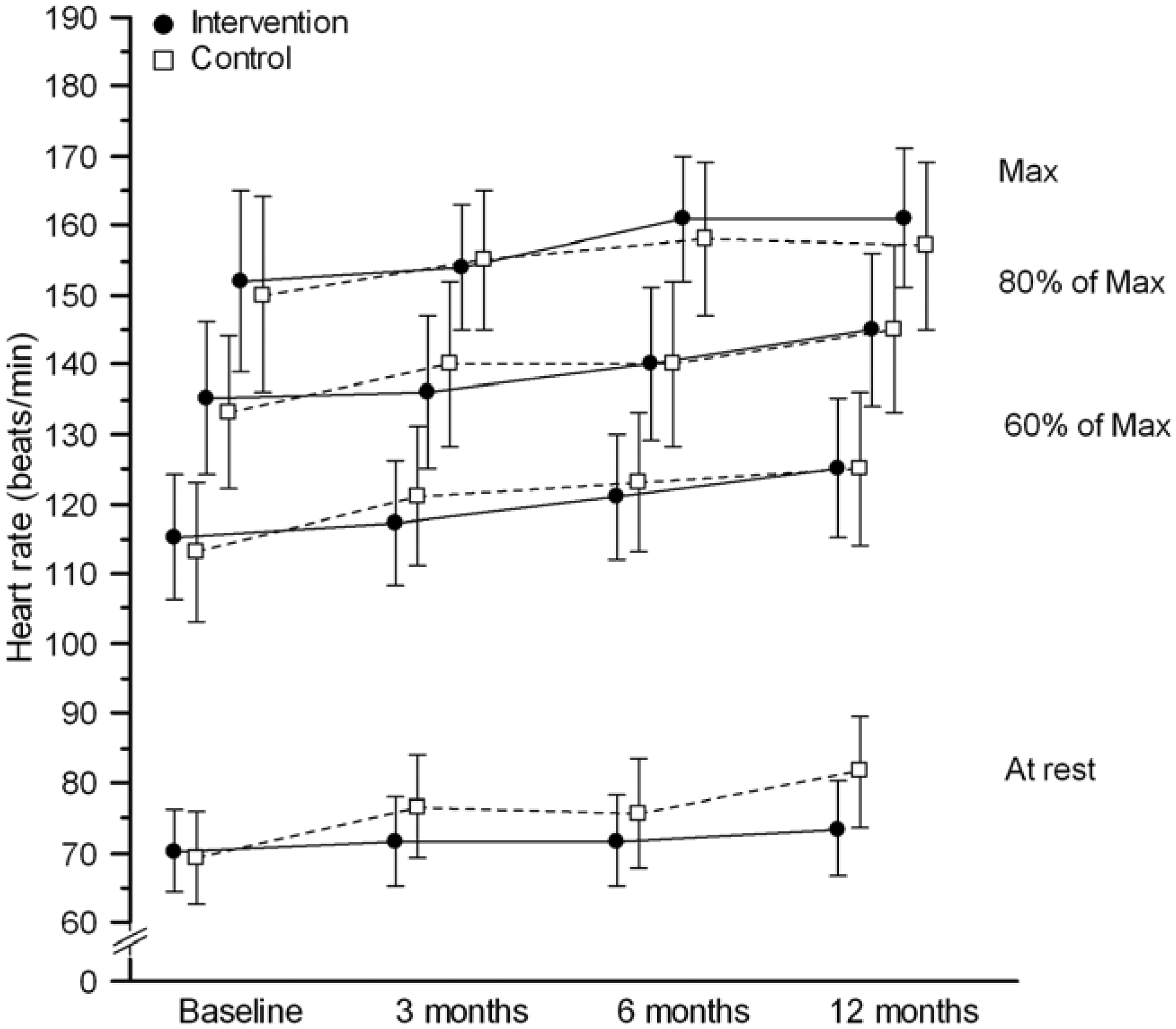
The estimation of voluntary effort during the bicycle test, that is, the RPE 6-20 scale, showed mean values between 16 and 17.7 during the study period, where 17 is rated as ‘very hard’.6,50,51 There were no significant differences between the groups at baseline and during the one year study period (interaction group × time, p = 0.45), however a main effect of time (p < 0.05) was seen. Post hoc test showed a significant decrease in RPE between baseline and month 3. The RER mean values were between 1.14 and 1.27 for both groups during all test occasions, where values above 1.1 are considered high effort.6,51 There were no interaction group × time (p = 0.38), however the C-group had significantly higher RER-values than the I-group on all occasions (main effect of group, p = 0.05). Independent of group, a significant decrease in RER by time (main effect of time, p < 0.0004) was seen. There was an increase in % of age-expected maximal heart rate, during the study period, independent of group (main effect of time p = 0.04). Expressed in percent, the increase was from around 90% at baseline to 95% at month 12. Taken together, there was no comprehensive support for the increase in maximal oxygen uptake by time being due to altered voluntary effort of the subjects.
Physical activity
The number of participants that answered the questions concerning physical activity at baseline was 17 in the intervention group and 14 in the control group. The number of subjects varied over the different time points, but all individuals included were analysed by Genmod statistical analysis. Frequency of physical activity at high intensity (times/week) increased, independent of group, during the one-year study (main effect of time,
Independent of time, the I-group was more physically active at low to moderate intensity (times/week) compared to the C-group (
HRQL
Health related quality of life, SF-36, at baseline, months 3, 6 and 12 in patients with SLE in the intervention (I) and the control (C) groups. Medians and quartiles (Q1–Q3) (non-estimated values) and the statistical outcome for the changes in the groups over the one-year study period

The higher the value, the better the function (scale 0–100).
The number of subjects varied during the different time points, but all individuals included were analysed by Genmod Procedure statistical analysis, which gives estimated values not presented here.
Disease activity, organ damage and pharmacological treatment
Descriptive data (non-estimated values) at baseline in patients with SLE in the intervention and control groups, and statistical outcomes for the changes in the groups over the one-year study period
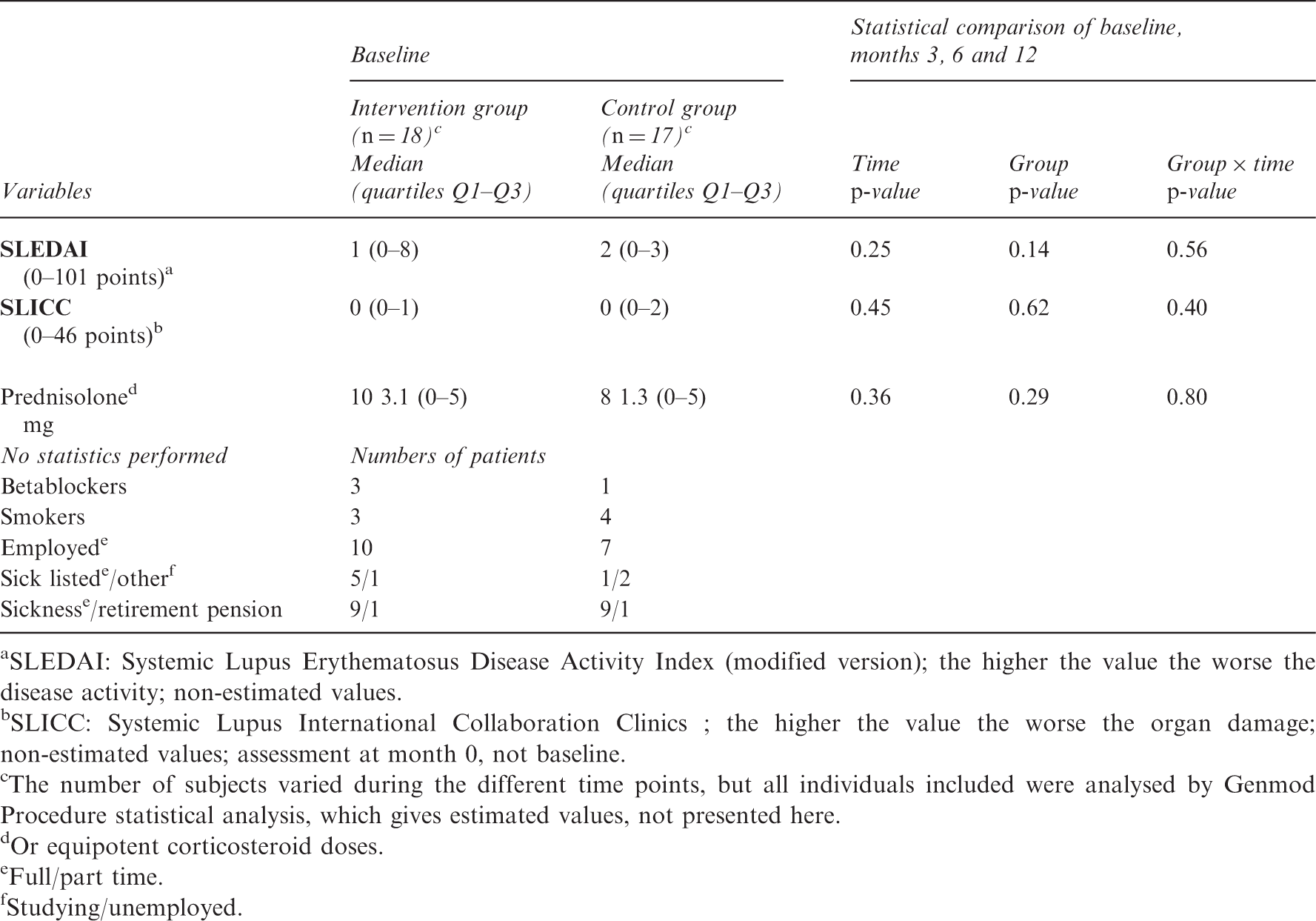
SLEDAI: Systemic Lupus Erythematosus Disease Activity Index (modified version); the higher the value the worse the disease activity; non-estimated values.
SLICC: Systemic Lupus International Collaboration Clinics ; the higher the value the worse the organ damage; non-estimated values; assessment at month 0, not baseline.
The number of subjects varied during the different time points, but all individuals included were analysed by Genmod Procedure statistical analysis, which gives estimated values, not presented here.
Or equipotent corticosteroid doses.
Full/part time.
Studying/unemployed.
Discussion
A physical activity programme for one year including supervised exercise and coaching for three months increased the frequency of physical activity at high intensity and aerobic capacity in patients with SLE. The improvement was sustained during the year. The programme also increased mental health between baseline and month 6. However, as there were no differences in physical activity and aerobic capacity compared to the control group, one explanation for the results could be that repeated measurements and exercise tests motivated increased physical activity and thereby increased aerobic capacity. This study also indicates that physical activity at high intensity for one year was tolerated by patients with mild-to-moderate SLE.
Our results are in line with studies in other patient populations, in which the outcome physical activity increased after counselling combined with heart rate monitor, physical activity diary and/or goal discussion.5,6,59–61 However, the effects of a physical activity programme in RCT design have to take into account the possible changes in spontaneous leisure time physical activity in the non-exercising control group. 62 The effects of a similar programme to ours in patients with rheumatic diseases vary.48,49,63 Van den Berg et al. 64 evaluated similar intervention as ours in patients with RA and found no differences between the intervention and control groups concerning the total amount of physical activity as measured by an activity monitor. A similar outcome was found in our study, that is, independent of group, the level of physical activity at high intensity was increased. It is possible that the repeated maximal bicycle ergometer exercise tests, including direct online registration of oxygen uptake and the assessments of disease activity and organ damage, might have motivated the control group to increase their self-initiated physical activity. It has been suggested 65 that measurement of, for example, physical activity is an intervention in itself, which may explain an increased physical activity level found in control groups. 65 Moreover, this non-intended change of behaviour in the control group is difficult to prevent in exercise studies with human participants, as the controls cannot be blinded for the aim of the study. In addition, performing RCTs of physical activity and exercise, in which the control group does not receive any intervention, is both a scientific and ethical dilemma. One cannot prevent the patients in the control group from increasing their physical activity.
The 16% increased aerobic capacity (VO2 max) in the I-group during the first three months in our study is comparable with earlier studies in patients with SLE, in which self-managed exercise with some supervision for eight weeks was employed, 31 but larger than the 7% increase reported in a clinical controlled study evaluating 12 weeks' supervised exercise by De Carvalho. 29 There may be several reasons for variations in adaptive response to physical exercise, such as age, genetic components, earlier experience of training, training status and disease severity.6,51,66 A longer disease duration and a more severe disease in our patients may explain differences between our results and those of De Carvalho et al. 29
The most likely explanation for the improved VO2 max. in our study is the increased physical activity at high intensity, which is in line with studies in healthy people 67 and in patients with SLE.29,30 Another explanation for the improved VO2 max. could be a familiarization effect, 51 as both the I- and the C-group increased their VO2 max. in a similar way over the study period. However, the fact that VO2 max. did not increase between baseline and month 0, a period of 2–3 weeks with no intervention, speaks against a familiarization effect.
In our study, there was a discrepancy between the increase in VO2 max. and the non-significant increase in maximal work load during the intervention. Therefore, increased work load cannot fully explain the increased VO2 max. One explanation might be related to training-induced changes in VO2 on-kinetics, that is, the rapidity with which the aerobic system adapts to an increased oxygen demand at a higher work load. 51 In our study VO2 sub-max. increased over time, and in healthy subjects it is known that training induces an acceleration of the VO2 on-kinetics at the same absolute work load. 68 Furthermore, Keyser et al. 69 demonstrated that VO2 on-kinetics was slower in women with SLE. However, whether or not a physical activity intervention could normalize such an abnormality in patients with SLE has not yet been tested.
One unexpected finding in the present study was the atypical heart rate response to physical activity, that is, the increase in heart rate at rest and more so during submaximal and maximal workloads (Figure 3). In healthy subjects, a training-induced decrease in heart rate is expected at rest and submaximal workloads, together with no change in maximal heart rate.6,51,70 A similar finding to ours was recently demonstrated by Miossi et al., 28 who found that patients with SLE basically had a reduced chronotropic reserve (difference between maximal and resting heart rate), which was increased (normalized) by training due to an increased (normalized) maximal heart rate. In other words, it seems as if exercise in SLE can induce improvement in the autonomic nervous system regulation, as reflected by an increase in chronotropic reserve and heart rate response.
One positive effect of the physical activity programme was the improvement in mental health according to SF-36, for example, lower feelings of nervousness and depression, between baseline and month 6. Similar effects have been recorded after physical exercise in patients with SLE29,32,33 and in patients with RA evaluating a similar physical activity programme to ours. 48 However, the change in our study was small, and we cannot determine if the improved mental function was a result of increased physical activity, improved aerobic capacity, individual coaching or a combination of these. The lack of improvement in other aspects of HRQL, such as fatigue (here vitality), might be explained by the extended time devoted to physical activity, and that this change in behaviour took energy from the patients and interfered with other activities. Also, more aspects of HRQL might have been affected if the programme had followed a theory-based model. 6
There are limitations in our study. One limitation is the presence of drop-outs, which is not unexpected during a one-year intervention programme. The drop-outs did not differ concerning age, disease duration and aerobic capacity from those who completed the whole study. Another limitation is the missing values in aerobic capacity, since not all patients were able to perform a maximal exercise test at all measurement times. However, problems caused by missing data were handled by using Mixed- and Genmode procedures in the statistical analysis. Still, low statistical power could be a reason for the lack of statistically significant interactions between group and time, and there could be a risk of type II error. Power calculations of none or up to 5% increase in VO2 max. in the C-group, including a few alternatives in the expected size of the SD of the difference, showed that between six and 16 subjects in each group were needed to reach 80% power, p < 0.05. However, the actual increase in VO2 max. became higher in the C-group than was expected. This may explain why only non-significant interactions between the groups were found. To increase the number of participants in physical activity studies in the future, multi-centre studies are needed.
Another limitation is that the care provider for the I-group was not blinded, which is, however, not possible to do in physical activity and exercise studies. There is also a risk of under- or overestimation and recall bias of self-reported physical activity questionnaires.71,72 Light and moderate intensity activities, which are more habitual in nature, are more difficult to recall than vigorous and strenuous physical activities.71,72 Similar physical activity questions to those that we used have, however, been related to cardiovascular risk, which contributes to the validity of our self-reported questionnaires.7,10
One further limitation is that we cannot draw any conclusions about patients with SLE with high disease activity and more severe organ damage. Our study did not include men and thus we cannot draw any conclusions concerning men with SLE. The patients who volunteered for this study might have been more interested in physical activity than those who declined to participate. However, among those who declined to participate in the study, around one third declared that they were already physically active. 15
In patients with SLE, aerobic capacity and the frequency of physical activity at high intensity was increased by a physical activity programme for one year, including supervised exercise for three months and coaching for six months. This improvement was sustained during the year. Our results concerning increased aerobic capacity are supported by other physical exercise studies in patients with SLE with low to moderate disease activity and organ damage.28–30 Since there were no interactions between the groups, the results also suggest that repeated measurements of physical capacity and physical activity could motivate to increase physical activity and thereby to increase aerobic capacity. As submaximal VO2 and heart rate increased over time, training-induced changes in VO2 on-kinetics or in chronotrophic reserve could contribute to the training-induced increase in aerobic capacity. Little influence on HRQL was seen after the programme. However, the study indicates that physical activity at high intensity for one year was tolerated by patients with mild to moderate SLE, since disease activity and organ damage did not deteriorate.
Footnotes
Acknowledgements
We specially thank the patients who participated in the study. We also thank the staff and the nurses Pia Tengvar and Rose-Mari Rönnquist at the Department of Rheumatology, Karolinska University Hospital, Solna, and nurse Maria Rosenqvist, Vasa, Finland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from The Swedish Rheumatism Association, the Vardal Foundation, the Board of Research and Postgraduate Education and the Centre for Health Care Science, Karolinska Institutet, Sweden.