
Abstract
Complement activation is a key feature of systemic lupus erythematosus (SLE). Detection of cell-bound complement activation products (CB-CAPS) occurs more frequently than serum hypocomplementemia in definite lupus. We describe a patient with normocomplementemic probable SLE who did not fulfill ACR classification criteria for lupus, but the diagnosis was supported by the presence of CB-CAPS.
Keywords
Introduction
The diagnosis of systemic lupus erythematosus (SLE) is generally made by the presence of a combination of clinical features and laboratory evidence of autoimmunity, especially a positive test for antinuclear antibodies (ANA), antibodies to native DNA, antibodies to Smith and/or low levels of serum complement (C3, C4). 1 There are no validated diagnostic guidelines for SLE but there are criteria for the classification of SLE devised and revised by the American College of Rheumatology (ACR). 2 Some patients do not fulfill the four criteria required to be classified as SLE and yet are considered by experienced rheumatologists to have that diagnosis, and are often designated as latent lupus erythematosus, incomplete lupus or probable lupus.3–5 Recently, the Systemic Lupus International Collaborating Clinics (SLICC) has devised criteria for the classification of SLE that are more sensitive than the ACR criteria but somewhat less specific. 6
Complement activation is a hallmark of the pathogenesis of immune-mediated tissue injury in SLE and yet the majority of SLE patients do not show serum hypocomplementemia, even during active disease. 7 Furthermore, plasma levels of complement activation products, while a more accurate measure of disease activity, are evanescent in plasma. On the other hand, cell-bound complement activation products (CB-CAPS), especially C3d and C4d on hematopoietic cells, are covalently bound and therefore have half-lives as long as the cells themselves. 8 CB-CAPS, measured as C4d on erythrocytes (EC4d) and B-cells (BC4d), have been shown to be present in most patients with SLE and to be more sensitive than low serum complement and positive anti-DNA for lupus diagnosis.9,10 This is a report of a patient who was considered to have probable lupus on the basis of clinical features and a positive ANA test but who fulfilled only three ACR classification criteria. The presence of a positive CB-CAPS test despite negative anti-DNA and anti-Smith antibodies, and normal C3 and C4 levels, support the diagnosis of SLE in this patient.
Case description
This is a 55-year-old African American female who was referred because of recent documented myelitis, a history of autoimmune thrombocytopenia, and a positive ANA test. She had been followed since 2012 for chronic thrombocytopenia that was first diagnosed in 2009. Platelet counts fluctuated from lows below 20,000/µl to highs of 140,000/µl but were generally below normal. When levels dropped below 50,000/µl, she was treated with moderate to high doses of oral corticosteroids with a good response. She had not received intravenous immunoglobulin, rituximab or other immunosuppressive agents. She was not taking hydroxychloroquine.
Three months before the referral, she was hospitalized for bilateral leg numbness without weakness; magnetic resonance imaging (MRI) with contrast showed enhancing hyperintensity of the spinal cord from T3 to T8. She was treated with high-dose methylprednisolone (SoluMedrol) for five days and discharged.
She was known to have a positive ANA (titer 1:1280, nucleolar pattern) and a positive lupus anticoagulant test (prolonged partial thromboplastin time (PTT) uncorrected with a 1:1 dilution with normal plasma, prolonged Russell Viper Venom time, abnormal platelet neutralization test) since 2012. Recent prior laboratory testing indicated a normal blood chemistry profile and normal levels of antibodies to double-stranded DNA (dsDNA), Smith antigen, SS-A, SS-B, ribonucleoprotein (RNP) and cardiolipin. Serum complement proteins C3 and C4 were both within the normal range.
She had a past history of endometrial cancer six years ago for which she underwent salpingo-oophorectomy. She had four pregnancies with four live births.
Her major complaints were persistent lower extremity numbness with tingling of varying severity and a band-like tightness across the lower abdomen. She denied Raynaud’s phenomenon, sicca symptoms, arthralgia and arthritis, skin rash, alopecia, renal involvement, chest pain, seizures, digital sores, and mouth sores. There was no history of major bleeding episodes. There was no history of peripheral arterial or venous clotting.
Physical examination revealed no rashes, livedo, or vasculitic lesions. There was no synovitis or muscle weakness, and gait was normal. There was decreased pinprick sensation below the abdomen and areflexia of the lower extremities.
Based on her clinical history and the laboratory results, treatment for SLE was begun with hydroxychloroquine and rituximab (for thrombocytopenia, myelitis).
Laboratory test values at first visit
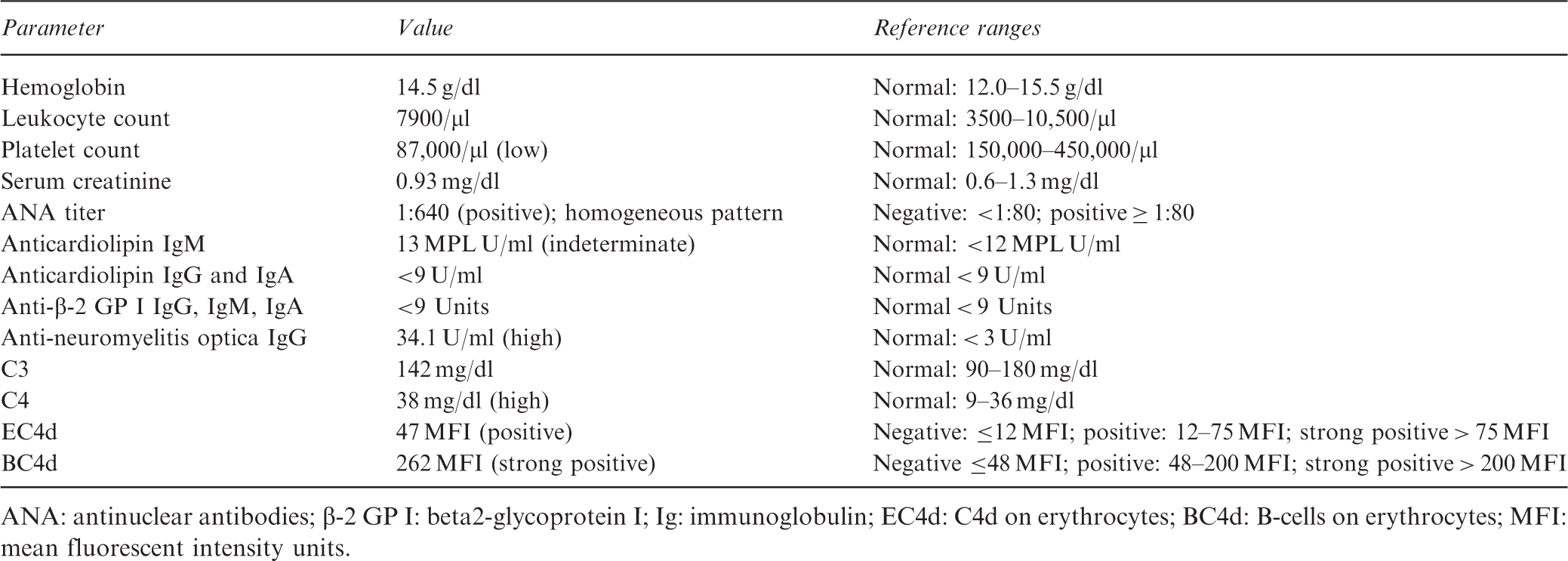
ANA: antinuclear antibodies; β-2 GP I: beta2-glycoprotein I; Ig: immunoglobulin; EC4d: C4d on erythrocytes; BC4d: B-cells on erythrocytes; MFI: mean fluorescent intensity units.
Discussion
For many years, this patient was not recognized as having SLE because of the lack of typical symptomatology and the negative testing for lupus-related autoantibodies. The positive ANA pointed to an autoimmune disease, which eventually resulted in her referral to Rheumatology after the development of spinal cord inflammation. She fulfilled only 3 of the 11 ACR criteria for the classification of SLE: thrombocytopenia, positive ANA, and positive lupus anticoagulant. The new SLICC criteria have expanded the neurological manifestations to include myelitis and thus four SLICC criteria are fulfilled for lupus classification. 6 In this patient, however, the strongly positive test for CB-CAPS also supported the diagnosis as well as classification of definite lupus, and appropriate therapy was instituted with hydroxychloroquine, rituximab, and subsequently enoxaparin.
The spectrum of SLE has expanded over the years to include patients with antiphospholipid syndromes, a broad variety of neurological complications, and unusual skin rashes as well as cardiac and hematological features.5,11–13 The ACR criteria were developed from typical cases and were meant to function as classification criteria for clinical research studies and therapeutic trials, and not for the diagnosis of an individual patient. However, because of the lack of published diagnostic guidelines, clinicians often use these criteria for diagnostic support. The SLICC criteria were developed to account for a greater spectrum of clinical features of SLE. However, they have not been used as widely as the ACR criteria. Even more helpful diagnostically are the presence of the more specific lupus biomarkers—anti-DNA antibodies, anti-Smith antibodies, and/or low complement levels. However, these markers may be absent, and none was present in this patient, even at the time of myelitis.
On the other hand, CB-CAPS have been shown to be very specific for lupus (80%–90% specificity8–10) and are present in the majority of lupus patients, even in those with milder disease.9,10 Furthermore, a recent study showed a high frequency of positive CB-CAPS in patients with pre-SLE, similar to those patients with definite SLE. 14 These patients had fewer than four ACR Classification criteria (two or three) and some did not fulfill SLICC criteria. However, they were considered to have SLE by very experienced lupus clinicians. This finding is not surprising since complement activation is considered to be a main mechanism of tissue injury in SLE, and activated complement products would be expected to be generated even if serum complement levels remain normal. Since these activated complement products such as C3d and C4d are evanescent in plasma but bind covalently to cells, the measurement of CB-CAPS provides an important biomarker both of lupus pathophysiology and diagnosis. 8 It is thus reassuring that this patient with probable lupus who fulfilled SLICC criteria but not ACR criteria demonstrated evidence of complement activation as is found in patients with more classical disease. Some studies have suggested that CB-CAPS levels fluctuate with disease activity.15,16 However, no large prospective study has as yet definitively demonstrated its value as a biomarker to predict lupus flares.
This patient had anti-neuromyelitis optica (NMO) antibodies. It is known that patients with probable lupus, definite lupus, and other connective tissue disorders can develop myelopathies, some of which are associated with antibodies to aquaporin-4, the antibody found in NMO. 17 Furthermore, complement-mediated injury may be important in the pathophysiology of autoimmune myelitis, and measurement of CB-CAPS might be of interest in these patients. 18 Anti-NMO is not one of the autoantibodies included in either the ACR or SLICC criteria but could be a useful biomarker in atypical SLE with myelopathies. The prevalence of CB-CAPS in these patients has not been studied.
This case suggests that CB-CAPS may have value as a diagnostic biomarker in patients with probable lupus, including those with normal serum complement levels.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Weinstein is on the board of directors of Exagen Diagnostics, Inc. Dr Lamichhane has no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.