
Abstract
Objective
To determine reproducibility and validity of an Argentine version of the Lupus Quality of Life questionnaire (LupusQoL) and to determine cut-off values in the questionnaire.
Materials and methods
One hundred and forty-seven systemic lupus erythematosus patients (American College of Rheumatology 1982/1997) were assessed from April 2014 to July 2014. Demographic and socioeconomic variables were collected, as well as SELENA/SLEDAI, Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index Score, comorbidities and treatment data. Patients completed LupusQoL-Argentine version and European Quality of Life Questionnaire (EuroQoL-5D). Internal consistency and reliability were examined. Convergent validity with EuroQoL-5D was assessed through analysis of latent classes, which established homogeneous categories from the responses of each domain of LupusQoL and for the total.
Results
Out of 147 patients, 93.2% were female, mean age 36.4 ± 11.1 years, mean disease duration 2.7 ± 9 years, mean SELENA/SLEDAI 2.7 ± 3 points. The cut-off point that defined good or bad quality of life was 0.739 for EuroQoL 5D and 63 for LupusQoL. Cut-off values for each LupusQoL domain were also defined, creating two classes in each of them. There was moderate to high concordance to classify quality of life (Kappa = 0.74, 95% confidence interval = 0.54, 0.95).
Conclusion
The Argentine version of LupusQoL is a valid, reliable and reproducible instrument to assess quality of life. In this study, cut-off points that allow the classification of patients regarding whether they have good or bad quality of life are established for the first time.
Introduction
Systemic lupus erythematosus (SLE) is a chronic, autoimmune and progressive disease that may affect any organ or system. 1 Better diagnostic tools and new therapeutic strategies have extended life expectancy in these patients.2,3 However, the use of drugs with certain toxicity and natural disease progression may significantly affect health-related quality of life (HRQOL) of patients. 4
There are generic tools designed to assess HRQOL in several chronic diseases, such as the European Quality of Life Questionnaire (EuroQoL-5D)) or the Medical Outcome Survey (SF-36 or SF 20 item), which have already been translated into Spanish. However, these tools lack specific domains for SLE.4-7
Through the EuroQoL-5D, patients classify their health state, first on levels of severity and then on a visual analogue scale (0 = worse quality of life and 100 = best quality of life). Health dimensions include mobility, self-care, usual activities, pain/discomfort, anxiety/depression, and each of them has three levels of severity: 1=no problems, 2 = moderate problems and 3 = severe problems. The questionnaire records the exact day patients answer it. The combination of the values of all dimensions generates a five-digit number, giving 243 possible combinations that can be used as profiles. The reference value index for each health state is obtained through a valoration technique called time trade-off. 8 The index varies from 1 (full health) to 0 (death), although there are negative scores that are valued as worse than death. 9
Questionnaires that evaluate HRQOL in SLE patients, such as the Specific Symptom Checklist, which consists in a symptom scale, do not assess HRQOL in an overall manner. Another questionnaire, the Systemic Lupus Erythematosus-specific Quality-of-Life, assesses less thoroughly the domains of physical function, pain and burden, and does not take into account body image. 7 None of the specific questionnaires presents a validated Spanish version. 10
Lupus Quality of Life (LupusQoL) is a questionnaire developed in the UK in 2007 in order to assess HRQOL in SLE patients, and presents multiple adaptations and validations into different languages and countries. This self-report questionnaire consists of 34 items grouped into eight domains: physical health, pain, planning, intimate relationships, burden to others, emotional health, body image and fatigue. The total score ranges from 0 (worst HRQOL) to 100 (best HRQOL). 7
Although there is a linguistic validation 7 into Argentine Spanish, until now there are no published data that assess LupusQoL reproducibility and validity in our country, and there are no cut-off values to classify good or bad quality of life of patients. Therefore, the purpose of this study was to determine reproducibility and validity of an Argentine version of LupusQoL in SLE patients and to establish the questionnaire’s cut-off points.
Patients and methods
This was a multicenter cross sectional study, including consecutive SLE patients (American College of Rheumatology (ACR) 1982/1997)11,12 that were under observation during April 2014 to July 2014. The study protocol was approved by the local ethics committee. All patients signed an informed consent.
Upon entry to the study, all patients underwent complete physical examination and laboratory, comorbidities and treatment data as well as demographic and socioeconomic variables were collected. The Safety of Estrogens in Lupus Erythematosus National Assessment/Systemic Lupus Erythematosus Disease Activity Index (SELENA/SLEDAI) was used to measure disease activity, and the Systemic Lupus International Collaborating Clinics/ACR Damage Index Score (SDI) assessed cumulative damage.13,14
After clinical examination, patients were given the Argentine version (linguistic validation) of LupusQoL questionnaire and EuroQoL-5D questionnaire to be completed. EuroQoL-5D was used as gold standard.
LupusQoL questions were answered according to the Likert scale response format, where 0 = all the time, 1 = most of the time, 2 = a good bit of the time, 3 = occasionally and 4 = never. Item response scores were totaled for each domain and the total score was divided by the number of items in that domain; the resulting value was divided by 4 and then multiplied by 100.
Transformed domain scores were obtained when at least 50% of the items were answered, and the mean domain score was thus calculated. A non-applicable response was treated as unanswered. The rest of the estimation was applied the same way as if all the items were answered. 15
Reliability and internal consistency
To assess reliability (precision of an instrument), internal consistency was analyzed using Cronbach’s alpha coefficient and test–retest of LupusQoL and EuroQoL-5D was performed 15 to 33 days later, establishing the intraclass correlation coefficient (reproducibility).
Predictive validity
To determine the predictive validity of LupusQoL with SELENA/SLEDAI and SDI, receiver operating characteristic (ROC) curves were used with LupusQoL scores and cut-off points of SELENA/SLEDAI (< or ≥4 points) and SDI (0 or ≥1). LupusQoL correlates to SELENA-SLEDAI and SDI also using Spearman’s rank correlation coefficient.
Latent class analysis – cut-off points
Latent class analysis (LCA) was applied to determine HRQOL classes, for both LupusQoL and EuroQoL-5D questionnaires, establishing homogeneity of classes and excluding classes for each individual.16,17 Using values of Bayesian Information Criterion as optimal criterion, it was determined that with both questionnaires two classes (quality of life categories) were defined. Then, from the probability values of each individual on each category, the class to which each patient belonged was determined. Based on these classes, cut-off points of each domain’s scores and of the total in LupusQoL, as well as for EuroQoL-5D scores through ROC curves, were established. Cut-off points allowed the classification of patients into good or bad quality of life.
LCA provides objective criteria, based on the authenticity of the model, to determine the number of groups (classes) present in the population. LCA allows modeling the relationship among the observed variables, supposing that the underlying structure of relationships is explained by a latent categorical variable (unobserved). It is based on the estimation of conditional probabilities, which allows the analysis of variables measured through different metrics, especially categorical data.16,17 Mutually exclusive classes of individuals can be identified with this technique, each individual with its own set of probabilities to belong to a class. In terms of LCA, the solution is optimal when classes are as homogeneous as possible, and the difference among them is as large as possible.
Convergent validity – discriminant validity
To correlate LupusQoL with EuroQoL-5D (convergent validity) Spearman’s rank correlation was applied. Correlation coefficients greater than 0.50, between 0.35 and 0.50 and less than 0.35 were considered strong, moderate and weak, respectively
For convergent validity of LupusQoL and EuroQoL-5D, LCA was first performed to establish homogeneous categories from the responses, for each LupusQoL domain, for the total and for EuroQoL-5D scores. Using those categories, and through ROC curve analysis, cut-off points for both questionnaires’ scores were established as well as the discriminant validity of the latent classes. Convergent validity between both questionnaires, using the established categories for latent classes analysis, was determined through Kappa concordance coefficient.
To evaluate association between comorbidities and good/bad quality of life using LupusQoL, the χ2 test was applied.
For statistical analysis, software R, Stata 10 and SPSS 19 were used. A value of p < 0.05 was considered statistically significant.
Results
Demographic and clinical features
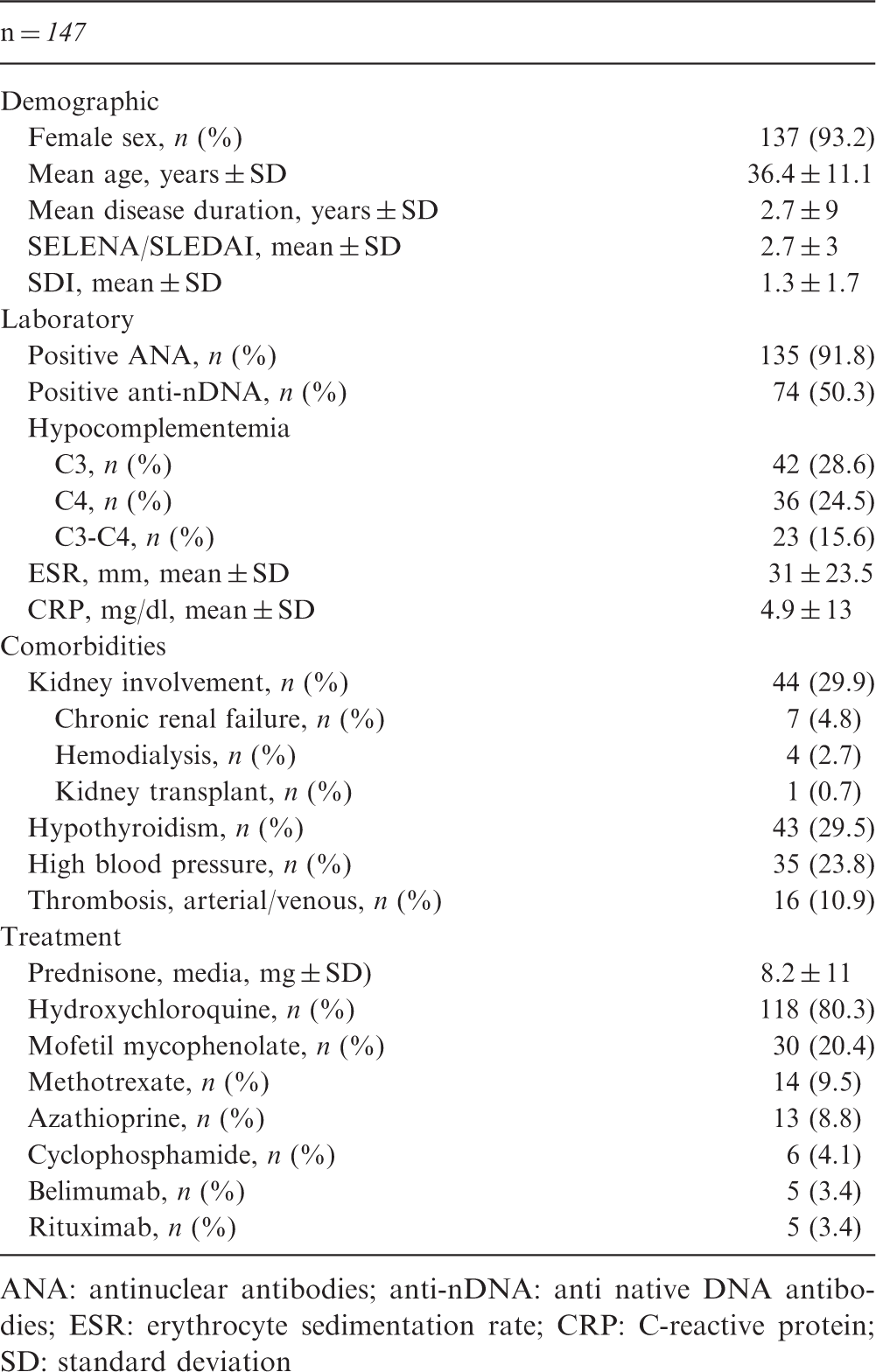
ANA: antinuclear antibodies; anti-nDNA: anti native DNA antibodies; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; SD: standard deviation
Reliability
Cronbach’s α coefficient was used to test for internal consistency, with a result of 0.9, showing an optimal consistency. The test–retest performed on 30 patients 15 to 33 days later had an intraclass correlation coefficient with excellent reproducibility (0.9).
Cut-off points
Through ROC curves, it was established that the highest percentage of patients correctly classified (95.2%) corresponded to a value of 0.739 for EuroQoL-5D. That is, those patients with EuroQoL-5D values equal to or higher than 0.739 presented good quality of life according to this questionnaire (Figure 1).
European Quality of Life Questionnaire (EuroQoL-5D) receiver operating characteristic (ROC) curve. Cut-off point to establish the highest percentage of patients correctly classified for EQ 5D.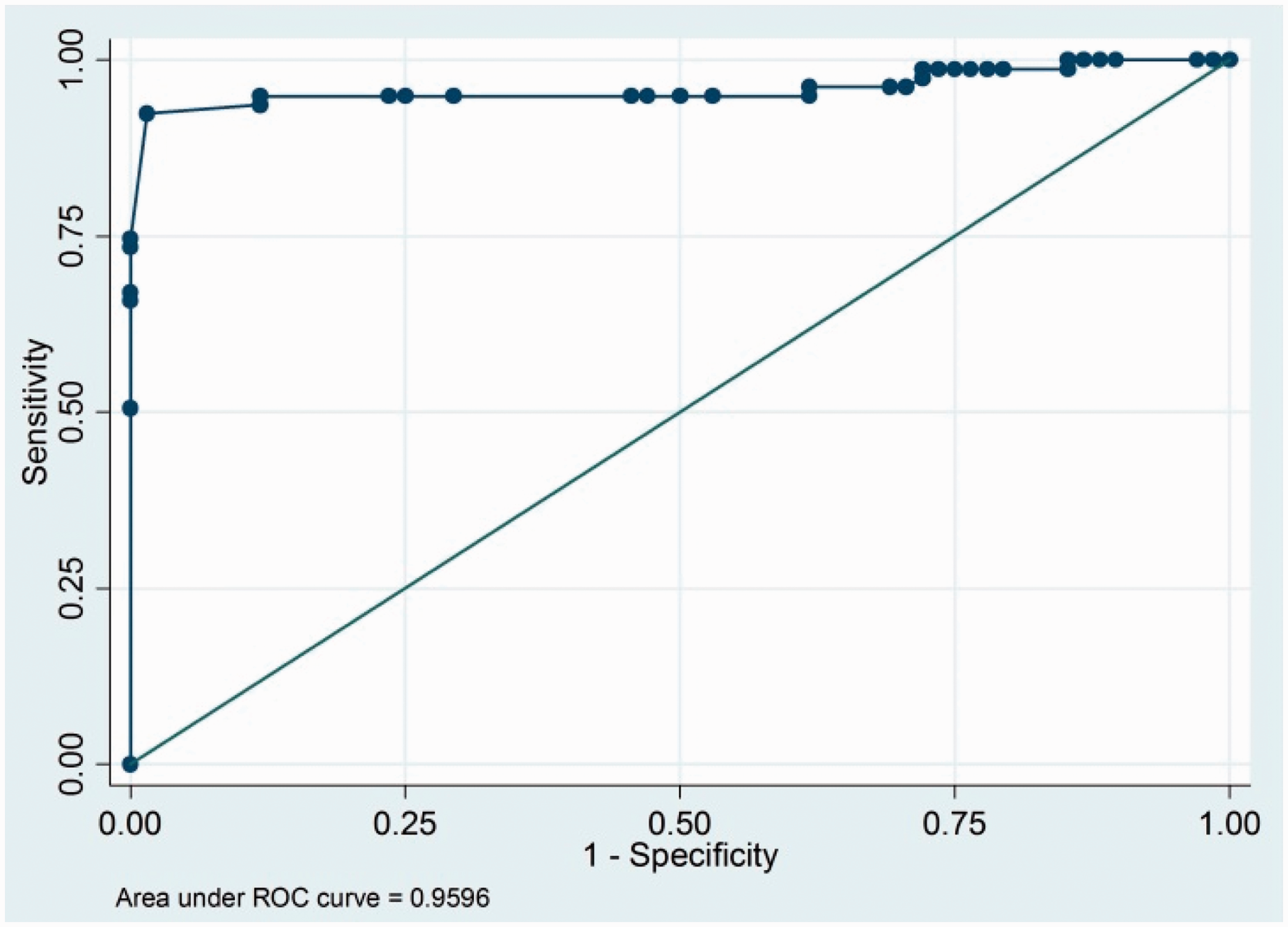
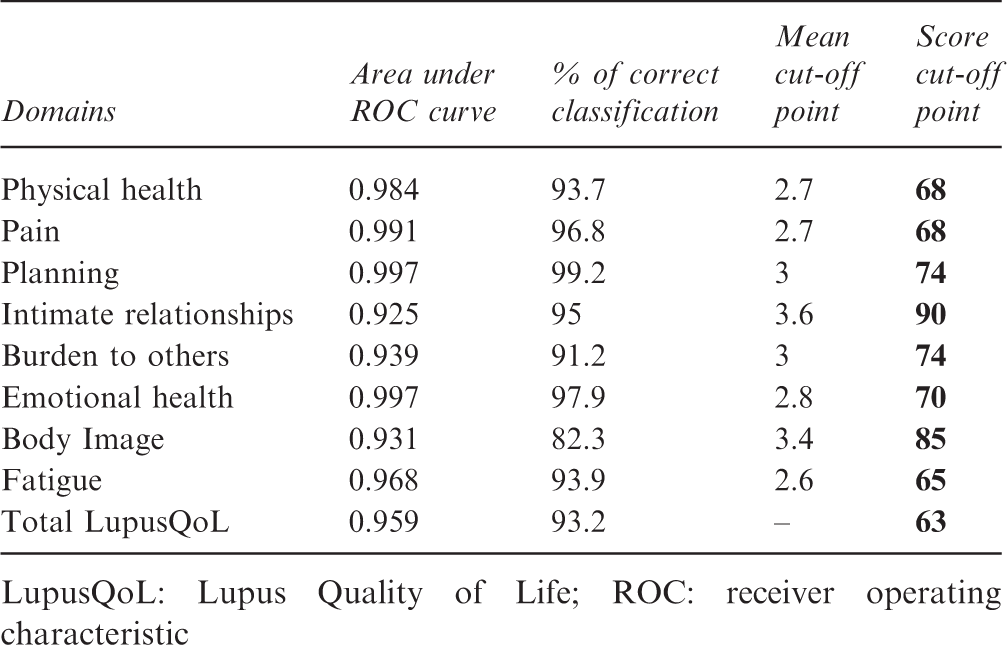
Likewise, LupusQoL cut-off point was determined, allowing the classification of patients between good or bad quality of life, and establishing that the highest percentage of patients correctly classified (93.2%) corresponded to a value of 63 points for LupusQoL. That is, those patients with LupusQoL values equal to or higher than 63 presented good quality of life (Figure 2). Additionally, cut-off points for each LupusQoL domain were established, from which, if patients present a higher or equal value, they have good quality of life for the assessed domain (Table 2).
Lupus Quality of Life (LupusQoL) receiver operating characteristic (ROC) curve. Cut-off point to establish the highest percentage of patients correctly classified for LupusQoL. LupusQoL cut-off points according to domains LupusQoL: Lupus Quality of Life; ROC: receiver operating characteristic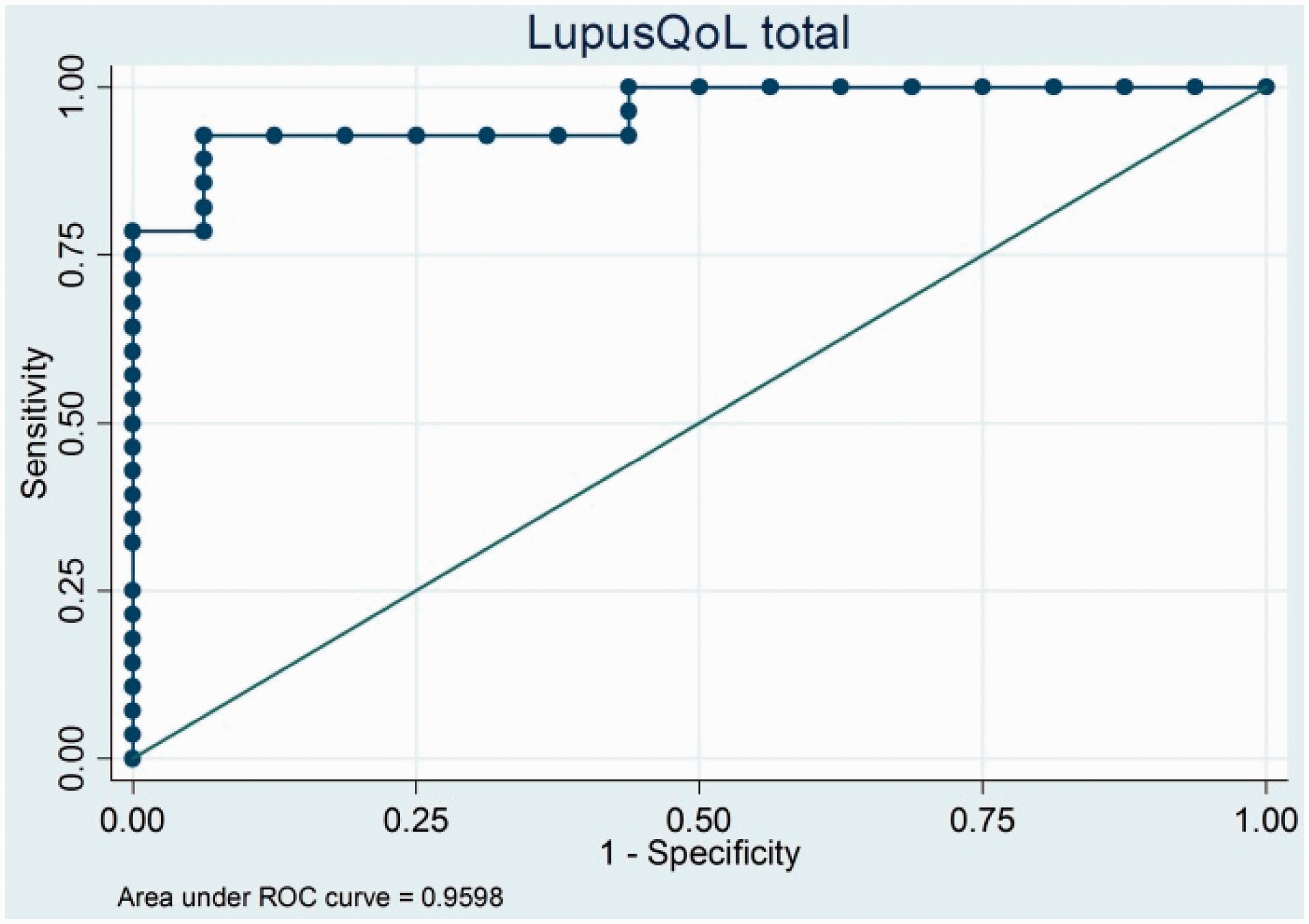
Convergent validity
LupusQoL and EuroQoL-5D were moderately correlated (rho=0.59, p<0.0001). Once cut-off points were established, patients were classified under good or bad HRQOL, and the degree of concordance between both questionnaires was determined, resulting in moderate to high concordance (Kappa coefficient 0.74, 95% confidence interval (CI) =0.54, 0.95).
Discriminant validity
LupusQoL was not correlated with disease activity (rho –0.39, p 0.637) and cumulative damage (rho –0.079, p 0.341) assessed through Spearman’s correlation coefficient (Figure 3).
Correlation between Lupus Quality of Life and SELENA/SLEDAI.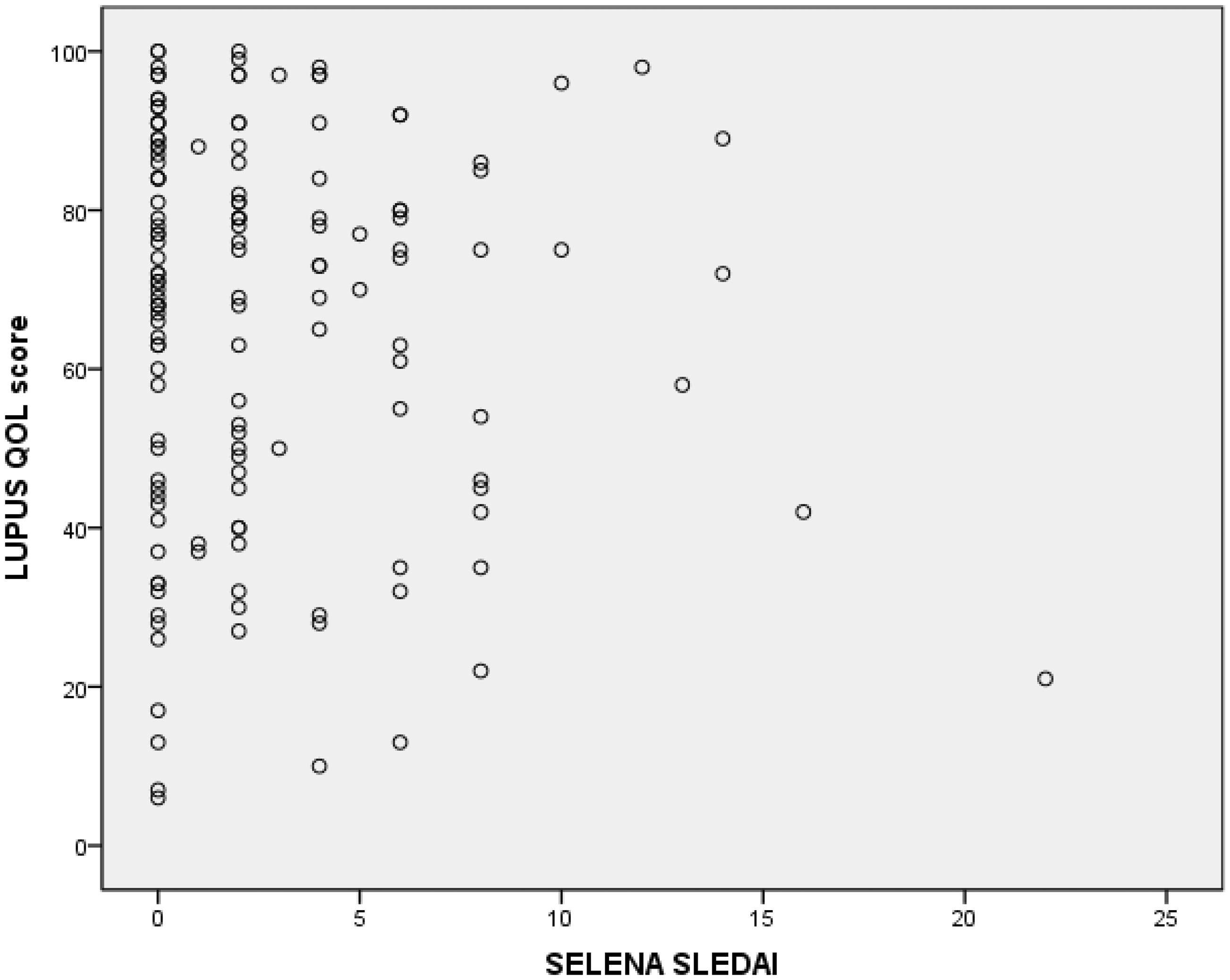
Predictive validity
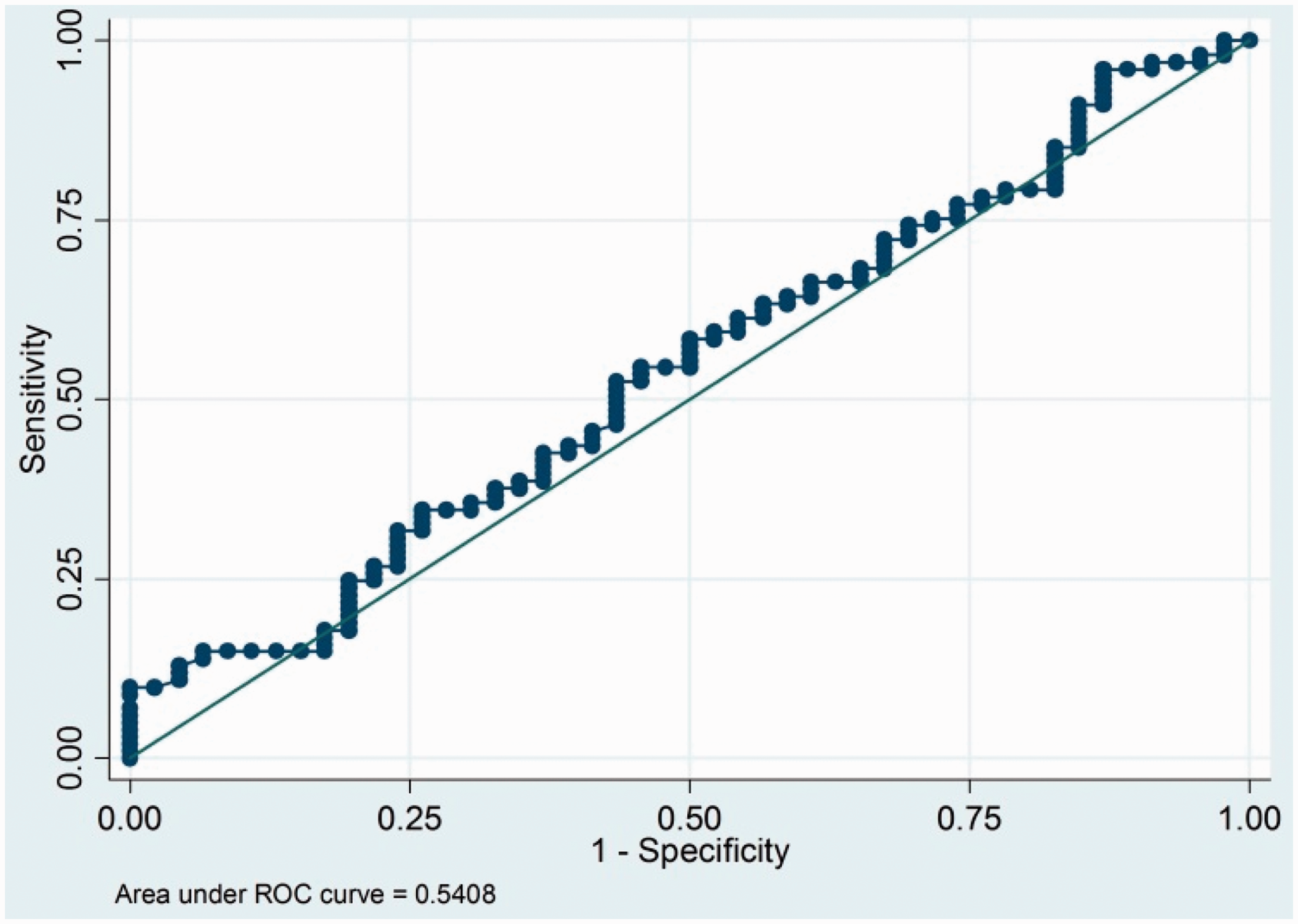
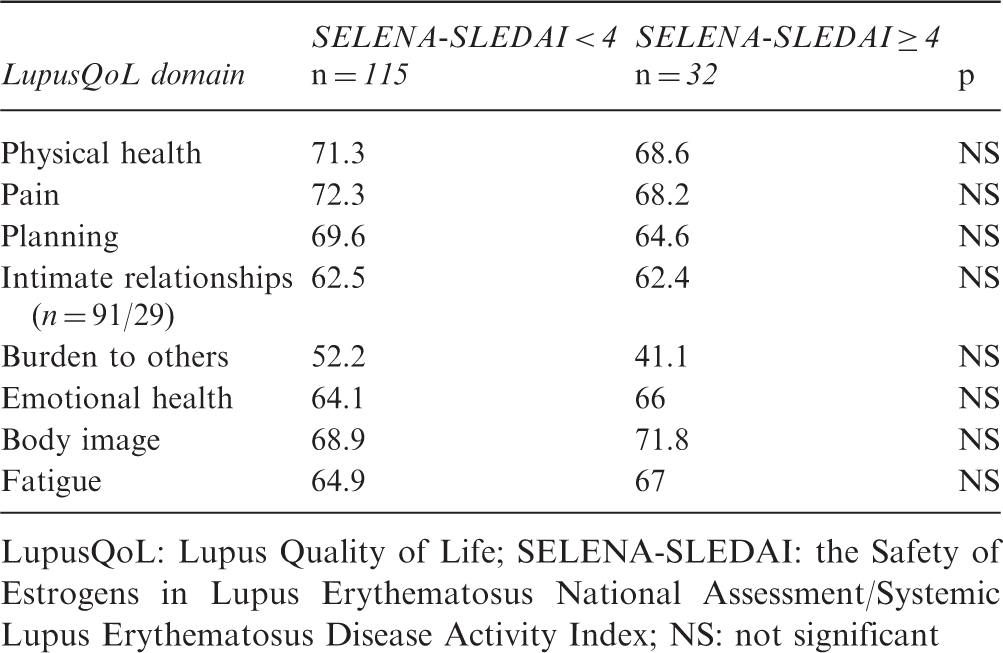
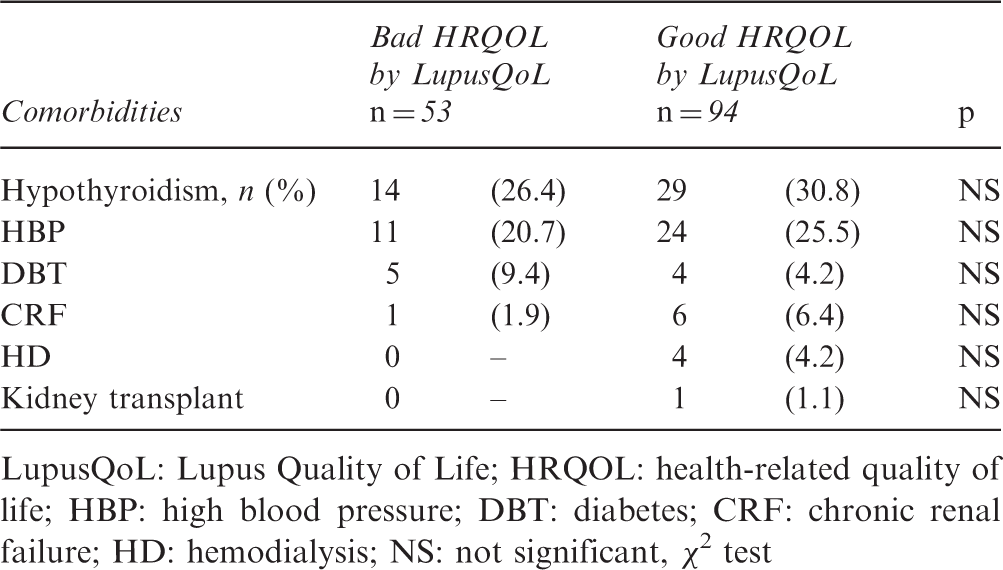
ROC curves and LupusQoL scores showed that this questionnaire is not adequate to predict disease activity (SELENA/SLEDAI ≥ 4) or cumulative damage (SDI ≥ 4) (Figures 4 and 5). Mean scores of each domain for each group were also compared (SELENA/SLEDAI < 4 and SELENA/SLEDAI ≥ 4; Table 3), and there were no significant differences in any domain. LupusQoL was not different according to the assessed comorbidities, such as arterial hypertension, diabetes, hypothyroidism and chronic renal failure (Table 4).
Lupus Quality of Life and Systemic Lupus International Collaborating Clinics/ACR Damage Index Score receiver operating characteristic (ROC) curve. The area under the curve shows the incapacity of LupusQoL to predict cumulated damage. Lupus Quality of Life and SELENA/SLEDAI receiver operating characteristic (ROC) curve. The area under the curve shows the incapacity of LupusQoL to predict disease activity. Comparison of LupusQoL domains’ scores according to disease activity by SELENA/SLEDAI LupusQoL: Lupus Quality of Life; SELENA-SLEDAI: the Safety of Estrogens in Lupus Erythematosus National Assessment/Systemic Lupus Erythematosus Disease Activity Index; NS: not significant Comorbidities and quality of life by LupusQoL LupusQoL: Lupus Quality of Life; HRQOL: health-related quality of life; HBP: high blood pressure; DBT: diabetes; CRF: chronic renal failure; HD: hemodialysis; NS: not significant, χ2 test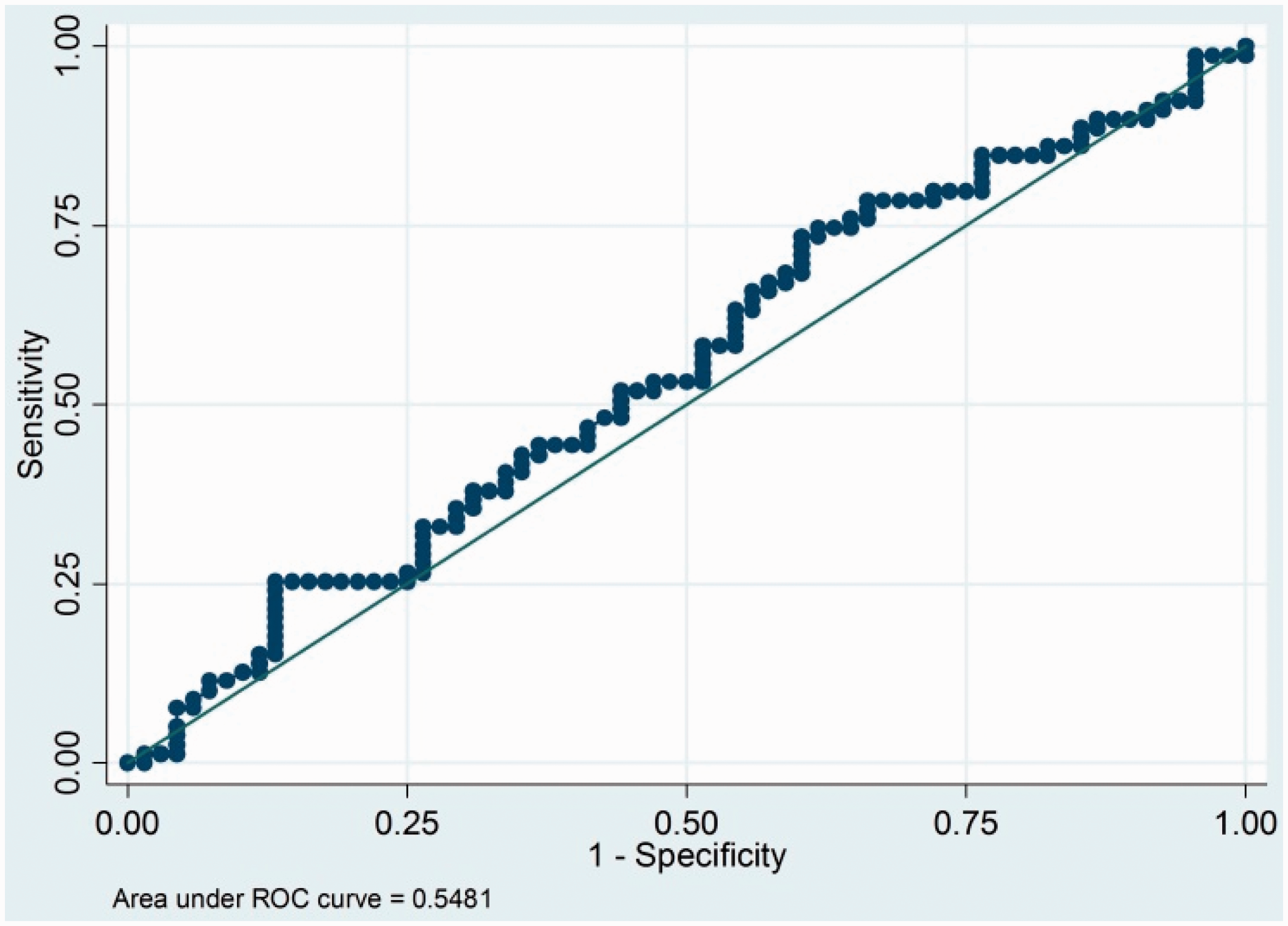
Discussion
Patients’ HRQOL is defined as a sense of well-being related to the disease or treatment and the perception of the disease’s impact on physical, mental and social functioning. In the assessment of lupus patients, which includes disease activity and cumulative damage, quality of life is gaining great interest. 18
This is the first study that determines reproducibility and validity of an Argentine version of the HRQOL questionnaire, Lupus Quality of Life, in SLE patients. And it is the first to establish cut-off points that allow the classification of patients between good and bad quality of life.
Although there are numerous generic questionnaires to assess quality of life in SLE, 18 EuroQoL-5D has been used in multiple studies,19–22 hence, it was used as gold standard for comparison.19–22
Results are different regarding usefulness of generic quality of life questionnaires in rheumatic diseases, especially in SLE, in which it is said that they lack disease specific domain evaluation (such as sleep and sexual functioning).4,8,18,23,24
Curry et al. noted that sexual dysfunction affect in a higher rate quality of life of patients. 25 Body image has also been reported to be impaired in SLE patients and is a major concern for the patients, and it is not included in the major generic measures used in SLE.18,26 Even more, sleep disturbances and depressed mood are frequent in SLE patients and may impact on fatigue, which in turn can affect HRQOL. 27
All of this field is related to instrument validity. Face validity refers to the degree to which a questionnaire measures what it is intended to measure according to the opinion of experts and the subjects themselves. Content validity is the extent to which the measurement covers the number of aspects of the concept under study. The construct validity ensures that measurements resulting from the questionnaire responses can be considered and used as a measure of the studied phenomenon and is defined as the ability of an instrument to accurately measure a theoretical construct. 28 Based on these definitions and knowing that both questionnaires measure different parameters of the quality of life of patients, we can understand why the generic questionnaires have a modest convergence with specific questionnaires.
Even more, SLE specific questionnaires also present dissimilar results, 29 hence, they are still trying to be improved. 30
When LupusQoL’s capacity to discriminate disease activity measured by SELENA/SLEDAI and cumulative damage measured by SDI is assessed, series of the United States, France, Italy, China and Spain, among others, present each LupusQoL domain’s results, since they are not equivalent among them and they present no significant differences in all domains.4,10,15,31,32
In our study, predictive validity in each domain was assessed with LupusQoL total score and for each domain. ROC curves with total scores (Figure 3 and 4) show how inadequate those scores are to predict disease activity and cumulative damage. Moreover, there was no significant difference between scores for each domain of LupusQoL according to good or bad HRQOL. This can be explained because quality of life of an individual depends not only on disease activity but also on other multiple factors such as ethnicity, health service coverage, social status, family life and therapeutic strategies, among others.
LCA allowed for the first time to divide patients into two well-defined categories, either for each LupusQoL domain or for the total result. Although the different series average the results for each questionnaire’s domain, none of them establishes categories that categorically define good and bad quality of life.15,32 Through this analysis it is intended to evaluate quality of life at a specific time of the disease and to compare it over time with subsequent results.
However, additional, larger, studies are still required to further assess the utility of the questionnaire.
In summary, LupusQoL is a valid instrument to assess HRQOL in SLE patients in Argentina. In this study, cut-off points that allow the classification of good and bad quality of life of patients are established for the first time.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.