
Abstract
Background
Systemic lupus erythematosus (SLE) is a life-threatening multisystem autoimmune disease that is more severe in patients of African ancestry and children, yet pediatric SLE on the African continent has been understudied. This study describes a cohort of pediatric SLE (PULSE) patients in South Africa.
Methods
Patients with a diagnosis of SLE (1997 American College of Rheumatology criteria) diagnosed prior to age 19 years in Cape Town, South Africa, were enrolled in this cross-sectional study from September 2013 to December 2014. Information on clinical and serological characteristics was extracted from medical records. Results were compared to a well-described North American pediatric SLE cohort.
Results
Seventy-two South African patients were enrolled in the study; mean age 11.5 years; 82% were girls. The racial distribution was 68% Coloured, 24% Black, 5% White and 3% Asian/Indian. Most patients presented with severe lupus nephritis documented by renal biopsy (61%). Of patients with lupus nephritis, 63% presented with International Society of Nephrology/Renal Pathology Society class III or IV. Patients in the PULSE cohort were more likely to be treated with cyclophosphamide, methotrexate and azathioprine. The PULSE cohort had high disease activity at diagnosis (mean Systemic Lupus Erythematosus Disease Activity Index-2K (SLEDAI-2K) 20.6). The SLEDAI-2K at enrolment in the PULSE cohort (5.0) did not differ from the North American pediatric SLE cohort (4.8). Sixty-three per cent of the PULSE cohort had end organ damage with Systemic Lupus International Collaborating Clinics Damage Index (SLICC-DI) score >0 (mean SLICC-DI 1.9), compared to 23% in a previously reported US cohort. Within the PULSE cohort, nine (13%) developed end-stage renal disease with six (8%) requiring transplant, strikingly higher than North American peers (transplant rate <1%).
Conclusions
The PULSE cohort had highly active multiorgan disease at diagnosis and significant disease damage at enrolment in the South African registry. South African patients have severe lupus nephritis and poor renal outcomes compared to North American peers. Our study revealed a severe disease phenotype in the PULSE cohort resulting in poor outcomes in this high-risk population.
Introduction
Systemic lupus erythematosus (SLE) is a life-threatening multisystem autoimmune disease. In North America and Europe, SLE is more common and more severe with increased mortality risk in people of African extraction compared with Caucasians.1–4 Despite the disproportionate prevalence of SLE among individuals of African descent, literature describing the epidemiology, diagnosis and treatment of SLE among individuals living on the African continent is sparse.5–12 Adult cohort studies from South Africa show poor outcomes, with five year survival rates ranging from 69% to 78%, compared to 88–95% in high-income countries. The only published pediatric SLE studies in sub-Saharan Africa have been reported from South Africa.13–16 The paucity of data has led to perceptions that SLE is rare in Africa,17,18 although more recent studies suggest under-recognition, under-diagnosis, under-reporting and poor access to care rather than rarity of disease.19–21
Children are at higher risk for severe SLE, typically presenting with higher disease activity and continuing with higher activity over time than adults. Presentation in childhood occurs in 15–20% of all SLE patients, with median diagnosis age for pediatric SLE (pSLE) at 12–14 years.22–24 Children are more likely to have serious renal, neurological and hematological involvement than their adult counterparts. 25 Mortality rates are higher in pSLE patients than adults, despite having fewer comorbidities. 26
Lupus nephritis (LN) is a serious complication of SLE, influencing prognosis and life expectancy more than any other organ system involvement.27,28 SLE patients with LN show a 15–24 year decrease in life expectancy compared to SLE patients without nephritis. 29 In high income countries, patients of African ancestry are two to three times more likely to develop LN, with a more severe renal disease course, 30 and those with end-stage renal disease (ESRD) have higher mortality rates than Caucasians with ESRD.31,32 Furthermore, LN is common in children. 33 pSLE patients have higher rates of renal damage and proceed to ESRD more frequently than their adult counterparts. 25 Treatment resistance disproportionately affects African American children. 34 In addition, LN is a major cause of morbidity and mortality for SLE patients in low income nations. 35
Thus, pSLE patients in Africa are potentially at high risk for poor outcomes based on race and age, yet strikingly little research has addressed this population.9,20,21,36 To date, only one cohort study of pSLE in sub-Saharan Africa has been published and there has not been an updated report on pSLE in South Africa over the past 10 years. 16
The aim of the current study is to determine if pSLE patients in South Africa have statistically significant and clinically important differences in disease severity, rates or severity of renal involvement, and disease damage compared to pSLE patients in a well-characterized North American cohort. We initiated a pSLE registry in South Africa and have performed an initial cross-sectional analysis at enrolment of pSLE patients presenting to care since 1988 at several hospitals in Cape Town, South Africa (referred to hereafter as the PULSE cohort). Here, we describe this cohort, compare it to patients in the Childhood Arthritis and Rheumatology Research Alliance (CARRA) Registry, a database that includes over 900 pSLE patients from 60 sites in North America, 37 and attempt to identify modifiable risk factors that could improve treatment and reduce organ damage in this population.
Methods
This retrospective study enrolled patients diagnosed with SLE prior to age 19 years at two tertiary care, government-funded university hospitals (Red Cross War Memorial Children’s Hospital; Groote Schuur Hospital) and one private medical center (Winelands Rheumatology Centre) in Cape Town, South Africa. The study was conducted as a collaboration between Duke University, USA and the University of Cape Town, South Africa, and approved by the Duke Institutional Review Board and the University of Cape Town Ethics Committee.
Participants
To develop the PULSE cohort, we identified eligible patients by searching the computerized databases of the two hospital centers where the study was conducted using International Classification of Disease version 10 codes for SLE or LN from hospital admissions and clinic visits. In addition, we polled physicians on site to generate a comprehensive list of pSLE patients. To include patients seen in private practice, we presented at national South African rheumatology meetings and sent recruitment flyers to all private rheumatology offices in the Western Cape. Inclusion criteria encompassed patients aged <19 years at SLE diagnosis who met the American College of Rheumatology (ACR) classification criteria for SLE, 38 and who had received care in the Western Cape Province, South Africa.
Once identified, living patients were approached for consent by their physician or study personnel. For patients less than 18 years old, we obtained parental consent; for patients aged 13 to 18 years, child assent was also obtained. Consent was conducted in the patient’s language of choice (Afrikaans, isiXhosa, or English). Deceased pSLE patients meeting enrolment criteria were included in review, for which a waiver of consent was obtained.
The CARRA Registry
For comparison, we used the existing CARRA Registrty. The CARRA Registry is a multicenter collaborative database that collects standardized information from 60 expert centers in North America. 39 Thus, we refer to the North American cohort as the total CARRA cohort. As of July 2012, there were over 900 children with pSLE enrolled. Patients with pSLE were eligible for inclusion in the CARRA Registry if they met at least four of 11 ACR criteria for SLE classification, developed pSLE prior to age 18 years, and were less than 21 years at the time of enrolment. 40
The following demographic features were obtained via chart review: age at disease diagnosis, gender, disease duration and self-reported race. 41 In South Africa, race was reported as one of the five racial groups employed in South African population surveys: Coloured, Black, White, Indian/Asian, and other (see Appendix). As most of the PULSE cohort is of African descent, we compared those patients to the African American subjects of the CARRA cohort (AA CARRA) to match more evenly on race/ethnicity between cohorts.
Clinical features
We measured the presence of organ system involvement at time of enrolment. To measure disease activity, we employed a well-validated SLE disease activity index measure (the Systemic Lupus Erythematosus Disease Activity Index-2K (SLEDAI-2K)). 42 We describe catastrophic clinical presentation in the South African patients. This is a term we created to capture the severe illness with which the majority of the PULSE cohort presented, including stroke, seizure, blindness, pericarditis causing tamponade, or acute renal failure. There are no data available on the frequency of such presentations in CARRA patients for comparison.
Laboratory tests and renal biopsy
We captured rates of positive tests for ANA, anti-Sm and anti-dsDNA antibodies. The anti-Ro, anti-La and anti-RNP antibodies have only recently become part of the routine assessment in South Africa, and were not included in this analysis.
In South Africa, only International Society of Nephrology and Renal Pathology Society (ISN/RPS) 43 histological classification is utilized; we therefore excluded CARRA patients with only World Health Organization biopsy classification from this comparison (n = 148).
Therapy
Inpatient and outpatient records were reviewed for current and prior therapy. All medications are reported as binary variables. The medication was scored as positive if the patient was receiving or had received the medication ever at study enrolment.
Outcomes
Through chart review, we extracted data on ESRD, dialysis, transplant and mortality. To measure chronic disease damage, we calculated Systemic Lupus International Collaborating Clinics/ACR Damage Index for systemic lupus erythematosus (SLICC-DI) scores. 44
Statistical analysis
We compared age of SLE diagnosis, race, presenting features, rate and class of LN, laboratory features, SLEDAI-2K and SLICC-DI scores, treatment and outcomes between the South African and North American patient cohorts. Characterization of the patient population was summarized using descriptive statistics with 95% confidence intervals of means and proportions for cohort comparison.
We evaluated enrolment SLEDAI-2K scores of the PULSE cohort compared to the CARRA cohort. Where appropriate, Kruskall–Wallis, Pearson, χ2 or Fisher’s exact test were used to evaluate differences in both clinical and demographic features and disease scores of the two cohorts. For better comparison of subjects of African ancestry between cohorts, we compared the PULSE cohort to the African American subjects in the CARRA cohort (AA CARRA).
As an exploratory aim, we attempted to identify risk factors for poor outcomes within the PULSE cohort. Unfortunately, the PULSE cohort was not large enough to provide sufficient power for this sub-analysis.
All calculations were performed using STATA statistical software (Stata Corp., College Station, TX, USA).
Results
Demographic features at enrolment
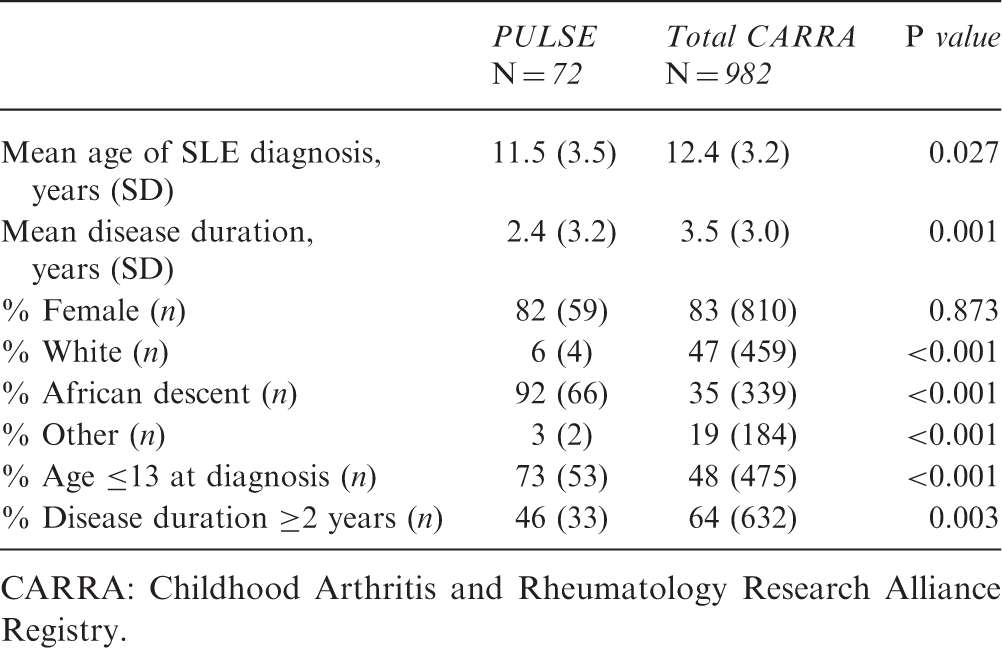
CARRA: Childhood Arthritis and Rheumatology Research Alliance Registry.
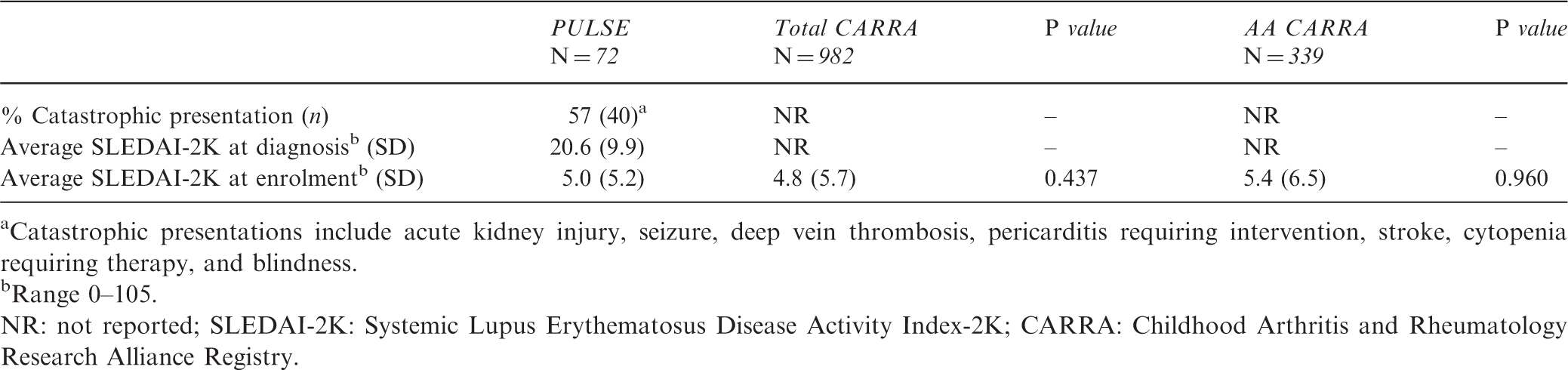
There are important differences in clinical and serological features of the cohorts (Figure 1, Table 2). Notably, a much higher percentage of the PULSE cohort had LN at enrolment compared to the AA CARRA group (61% vs. 42%, P < 0.001). The PULSE cohort demonstrated high disease activity at the time of diagnosis, represented by an average SLEDAI-2K score of 20.5; however, the score was recorded for only 44 of 72 PULSE subjects, and must be interpreted with caution due to the large amount of missing data. The CARRA Registry does not capture the SLEDAI-2K score at time of diagnosis. On chart review of the PULSE subjects, we noted that more than half of the patients (57%) presented with emergencies, such as acute renal failure, pericarditis causing tamponade, or stroke. There were 51 catastrophic events recorded among 72 patients. Seven patients (10%) had a severe disease manifestation in more than one category (i.e. presenting with stroke and acute renal failure). More than one third of patients in the PULSE cohort (37%) had acute kidney injury with decreased renal function at the time of diagnosis, 5% stroke, 4% deep vein thrombosis, 5% pericarditis requiring intervention and 3% seizure. At time of enrolment, the average SLEDAI-2K score of the PULSE cohort was not different from that of the total CARRA subjects or the AA CARRA subjects.
Clinical Features at Enrollment. Catastrophic presentation and SLEDAI at enrolment Catastrophic presentations include acute kidney injury, seizure, deep vein thrombosis, pericarditis requiring intervention, stroke, cytopenia requiring therapy, and blindness. Range 0–105. NR: not reported; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index-2K; CARRA: Childhood Arthritis and Rheumatology Research Alliance Registry.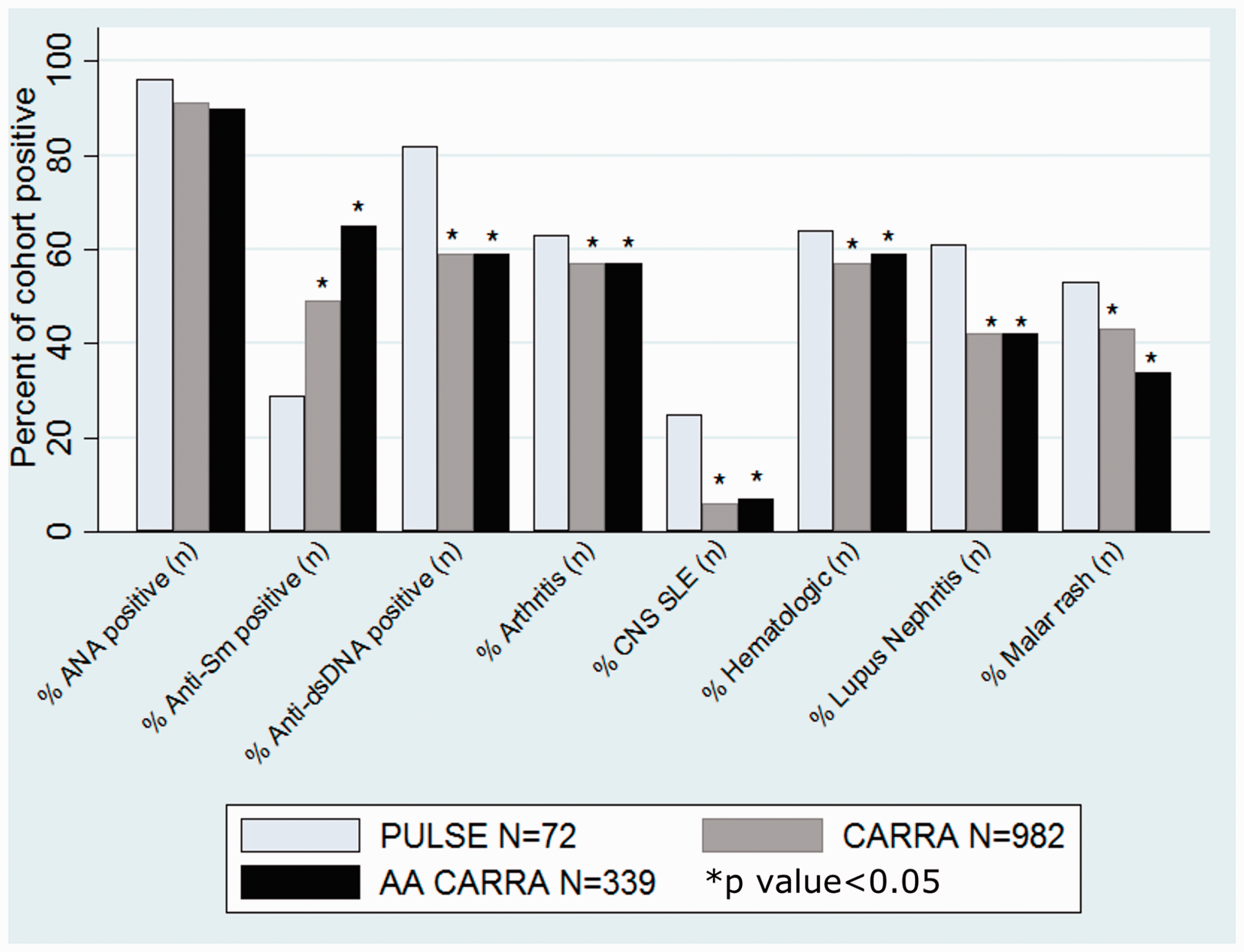
PULSE patients displayed an increased rate of severe renal disease compared to North American peers (Figures 1 and 2). The rate of biopsy confirmed LN (61%) in the PULSE cohort is higher than the CARRA cohort (42%). In comparison with CARRA, nearly all biopsied patients in the PULSE cohort (93%) had ISN/RPS class III, IV, V, or VI LN. Notably, 63% of those biopsied in the PULSE cohort had class III or IV LN, while only 48% of the CARRA cohort had these findings on biopsy. Moreover, 7% of the PULSE cohort had class VI LN on renal biopsy at enrolment, while none of the total or AA CARRA cohort demonstrated advanced sclerosis.
Features of Lupus Nephritis at Enrollment.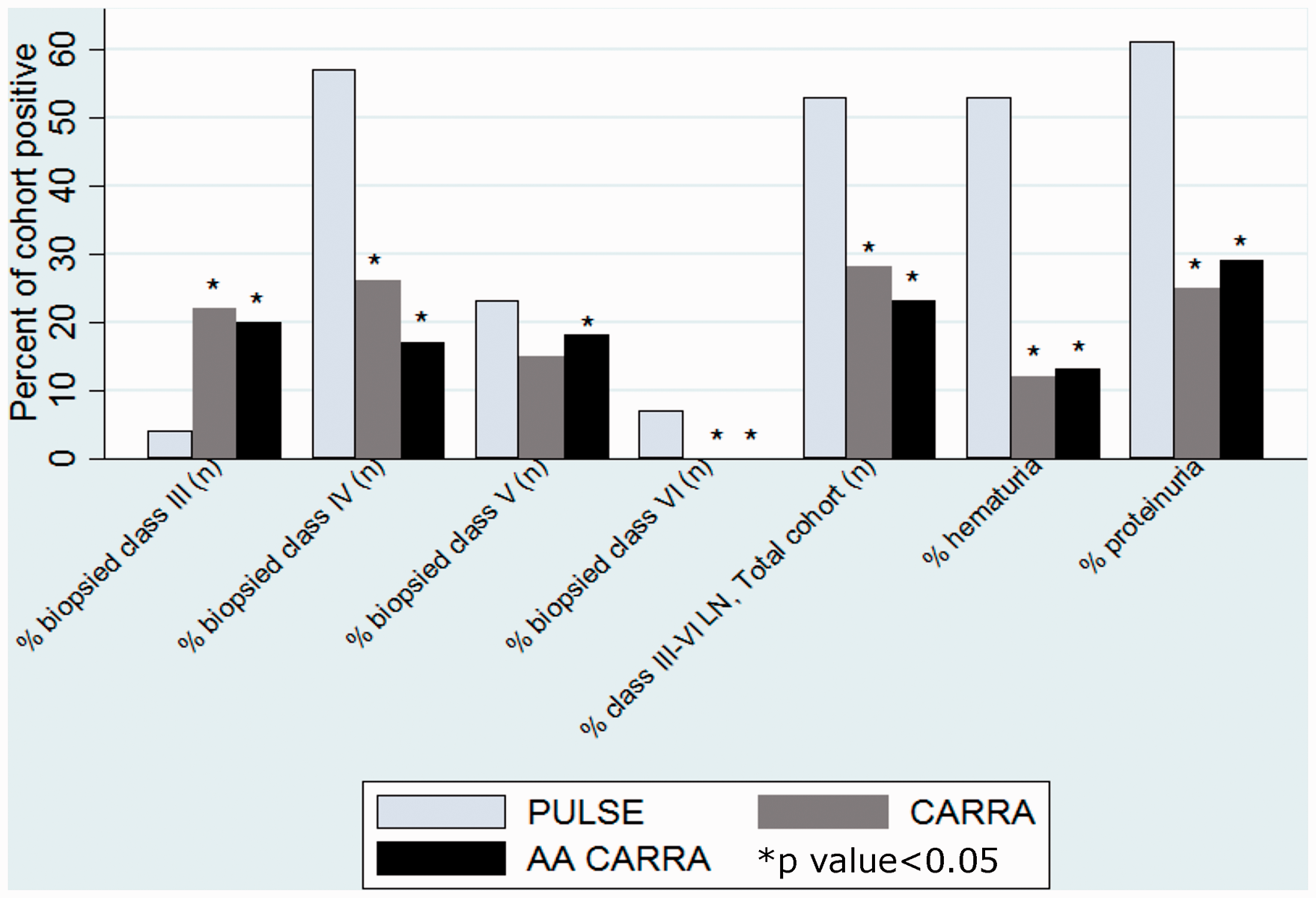
Treatment history at enrolment
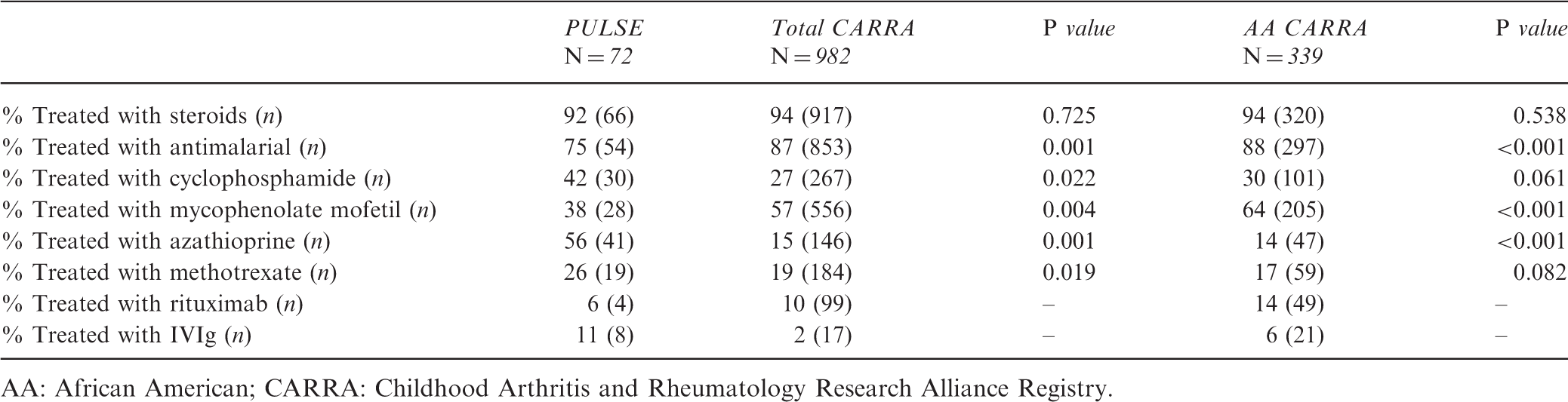
AA: African American; CARRA: Childhood Arthritis and Rheumatology Research Alliance Registry.
Measures of disease damage and renal outcomes
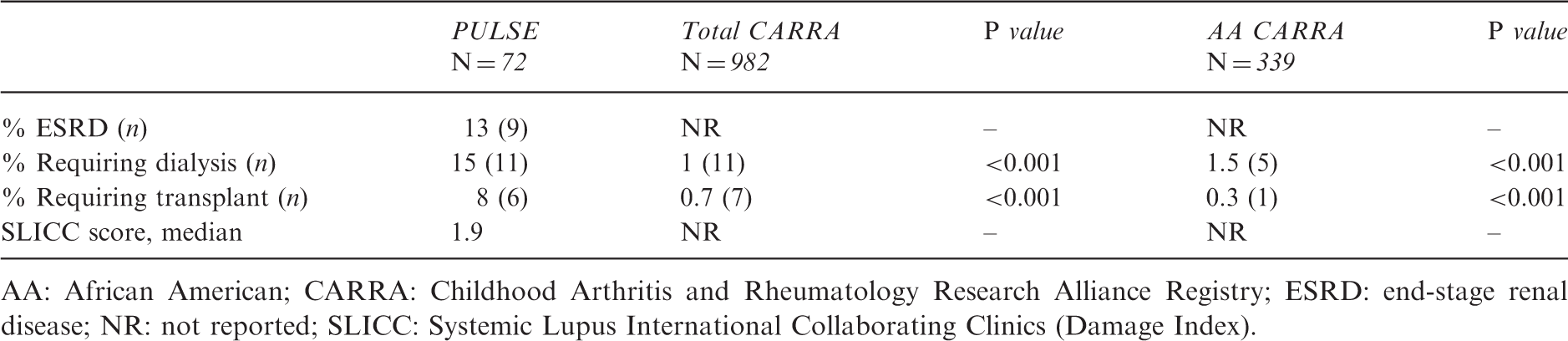
AA: African American; CARRA: Childhood Arthritis and Rheumatology Research Alliance Registry; ESRD: end-stage renal disease; NR: not reported; SLICC: Systemic Lupus International Collaborating Clinics (Damage Index).
Discussion
This study describes a cohort of 72 pSLE patients diagnosed before the age of 19 years in two medical centers and one office practice in Cape Town, South Africa (PULSE). This is the largest cohort of pSLE patients described in Africa to date. The only previous study of pSLE from sub-Saharan Africa was a retrospective cohort of 36 patients who presented to a Johannesburg hospital between 1974 and 2000. 16 The previous report had a much higher proportion of white patients (42%) than the current PULSE cohort, probably reflecting shifts in recognition, diagnosis and access to subspecialty care for black and coloured patients in South Africa since the end of apartheid in 1994. 45 The PULSE cohort reflects the racial composition of Western Cape Province (32% Black, 49% Coloured, 16% White, 1% Indian/Asian, 2% other) but is different from South Africa as a whole (80% Black, 9% Coloured, 2.5% Indian/Asian, 8.5% White). 46
The PULSE cohort is similar to the CARRA cohort in gender distribution, but differs in important measures of race, age, specific antibody profile and disease duration. Previous work suggests that young age and black race 37 predispose to increased disease activity in pSLE patients, and may contribute to the severe disease phenotype seen in our PULSE cohort. We compared the PULSE cohort to the African American patients in the CARRA cohort for a comparison based on self-reported race. Although the CARRA registry uses the eligibility criterion of SLE diagnosed prior to age 18 years, the present study includes all South African patients diagnosed prior to age 19 years. We extended the cut-off age to include those diagnosed at age 18 years to accommodate South African physician opinion that diagnosis was often delayed (C. Scott, June 2013; personal communication).
We observed increased clinical severity at presentation, higher rates of LN, and worse outcomes, as measured by SLICC-DI and the need for renal dialysis and transplant, among pSLE patients in South Africa. The PULSE cohort had higher rates of every disease manifestation examined, but the largest differences were seen in rates of renal and central nervous system involvement, which have the most impact on patient health and prognosis,34,47,48 and heavily influence treatment choice in pSLE.49,50 The high SLEDAI-2K score at diagnosis in the PULSE cohort indicates high disease activity at the time of presentation. The CARRA cohort study does not capture the SLEDAI-2K score at presentation, and data on SLEDAI-2K at presentation among diverse races/ethnicities are limited. One previous study of a well-described cohort of North American patients reports a mean SLEDAI-2K score of 13.8 in Caucasian patients and 12.6 in non-Caucasians at diagnosis, although black patients comprised only 15% of patients in that study. 51 The high SLEDAI-2K score and increased rates of all disease manifestations suggest a more severe phenotype in the PULSE cohort. Notably, the majority of South African patients had a catastrophic presentation, presenting with severe life-threatening manifestations such as acute renal failure requiring dialysis, blindness, or hemorrhagic stroke. These findings add to the evidence that South African patients have severe active SLE at diagnosis. It is not possible to determine if barriers to diagnosis and care influence the severity of disease on presentation in this cross-sectional cohort study; however, in-depth interviews with patient families suggest that this is likely to be a contributing factor (unpublished data). The SLEDAI-2K score at diagnosis was missing for more than half of PULSE subjects. For those in South Africa who had an enrolment SLEDAI score recorded, it did not differ from that of the CARRA cohort. Although we cannot infer causality in this retrospective study, this finding suggests that PULSE patients respond to therapy despite high activity at presentation.
The reported rate of LN in children with SLE is high (ranging from 50% to 67%) and patients of African descent in high income nations are two to three times more likely to develop lupus, more likely to have severe disease, and more likely to progress to ESRD than Caucasian counterparts.31,32,47 We found the rate of biopsy confirmed LN to be 61% in the PULSE cohort. The majority of biopsied patients in the PULSE cohort had class III–IV LN on biopsy at enrolment, while fewer than half of biopsied CARRA patients had class III or IV LN. Also, a percentage of biopsied patients in the PULSE cohort had advanced sclerosis, while no one in the CARRA cohort demonstrated this at the time of enrolment. One third of the PULSE cohort had acute kidney injury (AKI) at diagnosis. There is no information from the CARRA cohort on AKI for comparison.
The severity of LN in the PULSE cohort directly translates into poor outcomes. The PULSE cohort had high rates of ESRD, dialysis use and renal transplant at enrolment, in stark contrast to the much lower rate requiring dialysis and transplant in the AA CARRA cohort. Higher rates of dialysis and transplant in the PULSE cohort are not surprising given the higher rates of LN. However, the South African medical system is resource-limited with renal replacement and transplant therapy tightly rationed, requiring application and approval. 52 In context of the hurdles for access to these treatments, the increased rate in the PULSE cohort is especially striking.
Disease management differs between the PULSE and CARRA cohorts. Although antimalarial therapy is standard care worldwide, the PULSE cohort demonstrated lower use than the AA CARRA cohort. Antimalarial therapy is associated with higher rates of remission, fewer relapses and reduced organ damage. 53 It is unclear if this difference is due to lack of provider knowledge, drug cost, or adherence. The PULSE cohort was more frequently treated with cyclophosphamide, methotrexate and azathioprine, and less often with mycophenolate mofetil than the North American comparators. Treatment differences are impacted by medication rationing practices in South Africa. Therefore, the increased use of IVIg is surprising. However, 20% of the PULSE cohort initially presented with severe idiopathic thrombocytopenic purpura (ITP), which is commonly managed with IVIg in both North America and South Africa. It is not possible to determine if medication management differences resulted in differences in disease damage or outcomes in this cross-sectional study.
The PULSE cohort had significant organ damage, as reflected in SLICC-DI scores. The SLICC-DI score was not recorded in the CARRA database, so direct comparison between the two cohorts is not possible. Instead, we compared the PULSE SLICC-DI scores to those published in the Atherosclerosis Prevention in Pediatric Lupus Erythematosus (APPLE) cohort study, in which 25% of the 221 patients had a SLICC-DI score greater than zero. 54 This is vastly less than the 63% of the PULSE cohort with a SLICC-DI score greater than zero at enrolment. Higher SLICC-DI scores correlate with mortality in populations in high and low income nations. 55 Thus, high SLICC-DI scores indicate high morbidity and predict high mortality risk in the PULSE cohort.
The mortality rate in the PULSE cohort was 9.7%. Five year survival for pSLE patients has been reported as greater than 95%; 33 however, reports from other lower income nations show a poorer prognosis.56,57 Most deaths (six/seven) in the PULSE cohort were related to renal disease, whereas in the USA, SLE deaths are most commonly due to infections. 58 This contrast reinforces the importance of LN and poor access to RRT and transplant on prognosis in South Africa.
This study is limited by the relatively small number of patients enrolled in the PULSE cohort. Although it is the largest cohort in South Africa to date, the small total number of patients does not provide statistical power to look for meaningful subgroup differences within the cohort. The study is cross-sectional and limited by the documented medical chart. In addition, the study is restricted to one city in South Africa, and most patients were recruited from two major academic medical centers. This may limit generalizability, although the majority of CARRA participants are recruited from academic centers as well. The study uses standard local definitions of self-reported race; however, race is a social, not a biological construct, and patients are not readily separated into distinct categories. Our study included patients of African ancestry from two continents. The admixture of Africans, Caucasians and patients of other ancestry is arbitrary and inexact, 59 therefore comparison between populations is difficult. The specific racial contributions of South African black and coloured patients are different from African Americans. The South African black population is derived from Bantu tribes and the coloured population has indigenous Khoisan roots, with an admixture of Dutch, British and Asian ancestry. 60 The majority of African Americans have ancestral links to West Africa 61 and the genetic diversity of Africa is reportedly vast. 62 Nevertheless, SLE research has shown race to be a risk factor for severe disease.3,4,32,37,47 The only pediatric rheumatologists in sub-Saharan Africa are in South Africa; therefore, we rely on these data for the first glimpse into pSLE in the larger region. 20
In summary, the PULSE cohort demonstrates high disease activity at diagnosis and increased rates of LN, ESRD and organ damage at enrolment compared to North American cohorts. The high percentage of patients presenting with AKI suggests delayed diagnosis may play a role in the poorer outcomes seen in the PULSE cohort. The differences in outcome may be due to racial/ethnic predisposition to severe disease, late presentation due to barriers to health care access, or a combination of these and other factors. These differences were apparent even when compared to a North American cohort of African descent. Improving early recognition, diagnosis and access to treatment for pSLE patients in South Africa may lead to reduced organ damage. In addition, early aggressive therapy of LN may lower rates of ESRD requiring either RRT or renal transplant. Given the limited resource of dialysis and transplant, preventing primary damage in this cohort is especially important.
Further prospective research is necessary to gain a better understanding of the burden of pSLE in South Africa. A larger, prospective study is necessary to increase the cohort of patients with pSLE, determine management, and identify risk factors for poor outcomes. Translational research investigating biomarkers of lupus severity or genetic markers for increased disease severity may help to identify patients at high risk for severe disease in both low and high income nations. Future qualitative studies examining this population could help determine the role of barriers to care, which may in part explain disease severity at onset. Identifying risk factors and barriers to care is necessary to inform interventions to improve outcomes in this high-risk pediatric population.
Footnotes
Acknowledgements
The authors thank Melissa Watt and Coleen Cunningham for their thoughtful review of this work. Larry Park and Joseph Egger of Duke Global Health Institute assisted with statistical analysis. CARRA provided access to the North American SLE database. The authors would like to acknowledge the research team at Red Cross War Memorial Children’s Hospital, including Dr Kate Webb, Dr Lawrence O’kongo, Dr Nicola Brice, Sr Dorothy Brown, Sr Caroline and Zodwa Sam. Bradley Otterson, biomedical librarian/informationist, NIH Library at National Institutes of Health provided critical reading of this manuscript. This article was prepared while Laura B. Lewandowski was employed at Duke University Medical Center. The opinions expressed in this article are the author's own and do not reflect the view of the National Institutes of Health, the Department of Health and Human Services, or the United States government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LL was funded by the Lupus Foundation of America Early Career Award, T32 Training grant 5T32 AI0007217-31, Duke Global Health Institute Fieldwork grant and the Fogarty International Center of the NIH R25TW009337. The CARRA Registry was supported by grants from NIAMS RC2AR058934, Friends of CARRA and the Arthritis Foundation.