
Abstract
Background
Musculoskeletal involvement is extremely common in patients with systemic lupus erythematosus (SLE). Continuing the research initiated in patients with inflammatory arthritis, recent studies have shown the potential role of musculoskeletal ultrasound (MSUS) in the evaluation of clinical and subclinical lupus synovitis. The inflammatory process in SLE is traditionally considered to be localized at synovial tissue areas while enthesis is not included among the possible targets of the disease.
Patients and methods
Entheses included in the Glasgow Ultrasound Enthesitis Scoring System were scanned in a cohort of 20 SLE patients serving as disease controls in an MSUS study aimed at assessing enthesitis in patients with psoriatic arthritis. We describe in detail four cases with unexpected and unequivocal expressions of MSUS enthesitis according to the OMERACT definition. Three out of four patients had no predisposing factors for enthesopathy. Case no. 2 was treated with a variable-dose prednisone regimen.
Results
In the four cases MSUS examination revealed relevant grey-scale and power Doppler abnormalities at the entheseal level, most commonly at the distal insertion of the patellar tendon. Signs of clinical enthesitis were detected in only one patient.
Conclusions
This case series shows for the first time the presence of clearly evident MSUS findings indicative of enthesitis in four out of 20 SLE patients (20%), raising the hypothesis that enthesis could be a missing target in the clinical evaluation of SLE patients. Our case series justifies further investigations for a better evaluation of the prevalence, characteristics and clinical relevance of entheseal involvement in SLE.
Introduction
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease characterized by a vast heterogeneity of clinical manifestations due to the wide variety of organ involvement. The musculoskeletal system is one of the most commonly affected in SLE. 1 It is usually involved early in the course of the disease 2 with articular pain representing the initial symptom in more than 50% of patients. 3 Both large and small joints may be affected with the hands, wrists and knees described as the most frequently involved sites. 4 The arthropathy of SLE has a considerable clinical variability. It can range from mild arthralgias without erosions or deformities to a deforming non-erosive arthritis (Jaccoud’s arthritis and a mild deforming arthropathy), or an erosive symmetric polyarthritis resembling rheumatoid arthritis (rhupus arthropathy). 5 As well as arthritis and arthralgia, musculoskeletal pathological features of SLE include osteonecrosis, myositis, tendonitis, tenosynovitis and tendon ruptures. 6 Entheseal involvement appears to be largely ignored in SLE without any mention in textbooks or in reviews.7,8
In recent years, musculoskeletal ultrasound (MSUS) has become an important tool for the rheumatologist for the evaluation of patients with inflammatory arthritis. A growing body of evidence is emerging regarding the capacity of MSUS to detect subclinical inflammation at the joint, tendon and entheseal level. This was initially demonstrated in rheumatoid arthritis 9 and, more recently, in psoriatic arthritis and seronegative spondyloarthropathies.10–14 MSUS has also proven to be a valuable imaging tool in the assessment of SLE patients, as illustrated in studies evaluating tendon and joint involvement of hands and feet.15–18
To the best of our knowledge, there are no MSUS studies aimed at investigating entheseal involvement in patients with SLE with the exception of one study assessing periarticular changes in juvenile SLE. 19 The unexpected observation of unequivocal entheseal abnormalities in a cohort of 20 SLE patients, serving as disease controls in an MSUS study of our group aimed at assessing enthesitis in psoriatic arthritis patients, induced us to describe in detail clinical and MSUS characteristics of this subset of patients. We selected the cases with the most relevant entheseal changes detected by MSUS in patients without other predisposing factors for enthesopathy.
Material and methods
The high-resolution MSUS assessment was performed using a MyLab Class C (Esaote Spa) ultrasound system, equipped with a 6–18 MHz linear probe, working at a Doppler frequency of 9.1 MHz. The scanned entheses were those included in the Glasgow Ultrasound Enthesitis Scoring System: 11 the patellar insertion of the quadriceps tendon, the patellar insertion (proximal) of the patellar tendon, the tibial insertion (distal) of the patellar tendon, the calcaneal insertion of the Achilles tendon and the calcaneal insertion of the plantar fascia. The anatomical sites were scanned bilaterally, both in longitudinal and transverse plane, in grey-scale (GS) and power Doppler (PD) mode. Multiplanar MSUS examination of the knee entheses was carried out with the patient in a neutral position (i.e. supine position with extended lower limbs). The Achilles enthesis and the calcaneal insertion of the plantar fascia were scanned with the patient lying prone with the feet in a neutral position hanging over the edge of the examination table. During MSUS examination particular attention was paid to avoid the compression of the soft tissues which could generate false-negative PD findings. 20 Entheseal involvement was assessed by detecting the presence/absence of GS changes (hypoechogenicity, entheseal thickening, calcifications, enthesophytes, erosions) and PD signal, as defined by the Delphi process aimed to classify enthesitis by ultrasound in spondyloarthritis carried out by the Outcome Measures in Rheumatology (OMERACT) Ultrasound Task Force. 21 We also scored the degree of PD signal according to the MAdrid Sonographic Enthesitis Index. 22 In order to differentiate the origin of the pathological process and to exclude metabolic, degenerative, or traumatic causes, we carefully evaluated all factors that may affect the MSUS findings at the entheseal level. These included lipid profile, body mass index, history of trauma, sport activity (regular, recent or agonistic) and corticosteroid therapy.23,24 We did not include patients with psoriasis (current, personal or with family history), inflammatory bowel disease or presenting with clinical findings indicative of a possible overlap with seronegative spondyloarthropathies.
Results
Demographic, clinical and laboratory characteristics of the four patients
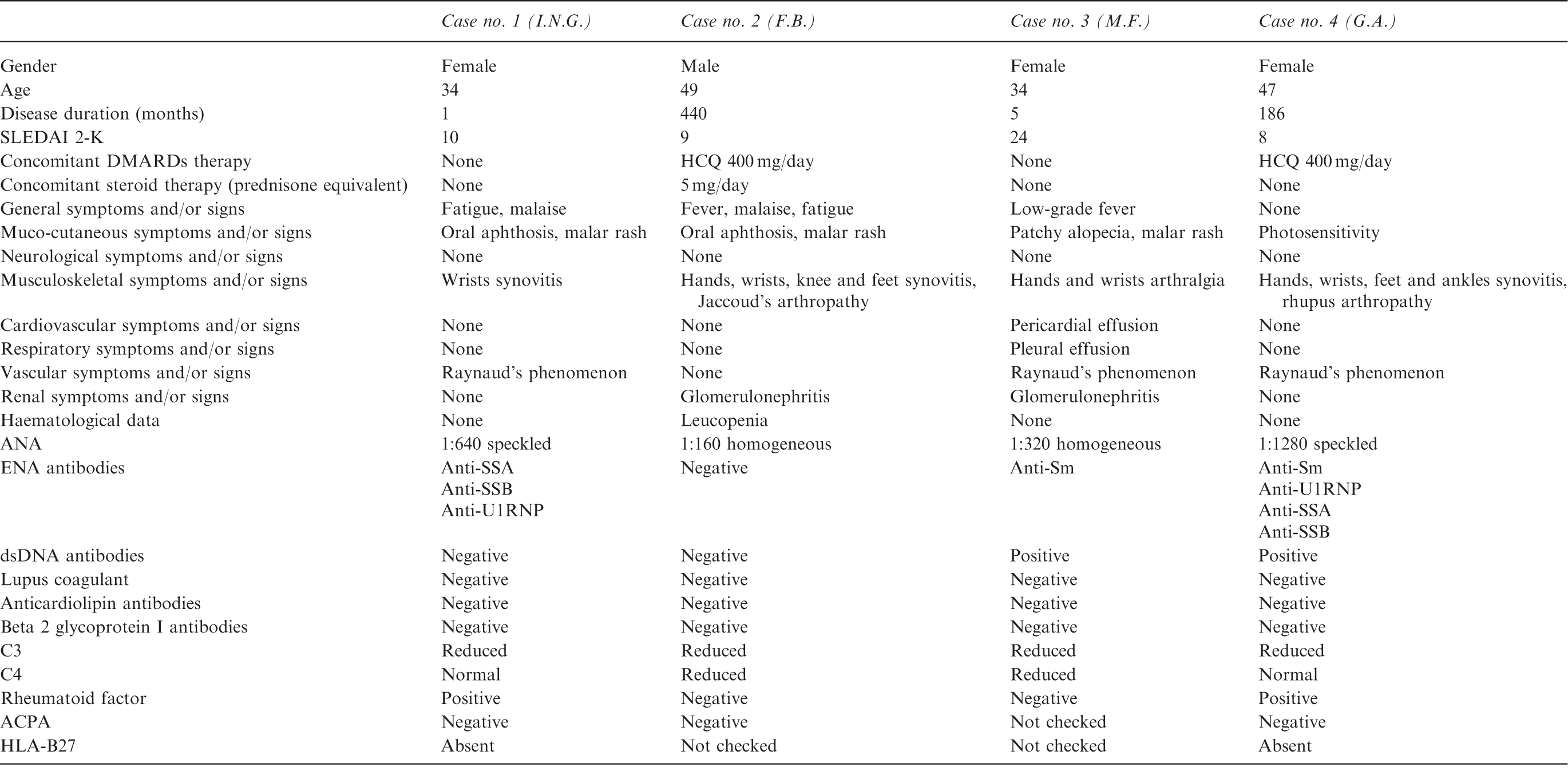
SLEDAI 2-K: Systemic Lupus Erythematosus Disease Activity Index 2000; DMARDs: disease-modifying antirheumatic drugs; HCQ: hydroxychloroquine; ANA: antinuclear antibodies; ENA: extractable nuclear antigen; dsDNA: double-stranded DNA; ACPA: anti-citrullinated protein; HLA-B27: human leucocyte antigen B27; Anti-Sm: anti-Smith; Anti-U1RNP: anti-ribonucleoprotein U1.
Case No. 1 (Patient I.N.G.)
The first patient is a 34-year-old female with no significant past medical history, no personal or family history of rheumatic/autoimmune disease and no previous miscarriage.
In winter 2014 she developed Raynaud’s phenomenon without telangiectasia or digital ulcerations. In summer 2015 she was admitted to our department with the onset of malar rash (‘butterfly’ rash) occurring after sun exposure, wrist synovitis, oral aphthosis, malaise and fatigue. The autoantibody profile revealed positivity of antinuclear antibodies (ANA) (1:640, speckled pattern), anti-Sjögren’s syndrome-related antigen SS-A (833 U/ml, normal value (n.v.) <7) and anti-SS-B (98 U/ml, n.v. <7), anti-ribonucleoprotein U1 (U1RNP) (46 U/ml, n.v. <5) and rheumatoid factor (RF) (46.2 UI/ml, n.v. <20). Anti-double-stranded deoxyribonucleic acid (dsDNA), antiphospholipid and anti-citrullinated protein (ACPA) antibodies were negative. Human leucocyte antigen B-27 (HLA B-27) was absent. Erythrocyte sedimentation rate (ESR) was slightly increased (25 mm/h, n.v. <20), C-reactive protein (CRP) was negative and C3 mildly reduced (86 mg/dl, n.v. 88–200). Renal function, liver function, full blood count and urinalysis were normal. The patient underwent an echocardiogram and a high-resolution chest computed tomography (CT) which did not show any pathological findings. Pulmonary function test, nailfold capillaroscopic exam and Schirmer test were negative.
X-rays and MSUS of hands and wrists showed bilateral severe reduction of the radiocarpal joint space and radiocarpal proliferative synovitis with grade 2 PD signal, respectively. The clinical examination of entheses did not show any soft tissue swelling or tenderness, whereas MSUS revealed bilateral GS and PD abnormalities at the patellar tendon tibial insertion. These findings consisted of entheseal thickening with hypoechoic areas and grade 2 PD signal (Figure 1). No pathological findings were found in the other entheses examined.
Case no. 1 (Patient I.N.G). Right patellar tendon, distal insertion ((a) longitudinal scan – GS and PD image; (b) transverse scan – GS and PD image) and left patellar tendon, distal insertion ((c) longitudinal scan – GS image; (d) longitudinal scan – PD image). The pictures show focal hypoechoic areas (asterisks) with grade 2 PD signal (red spots). Callipers indicate thickened distal enthesis of the left patellar tendon. GS: grey-scale; PD: power Doppler; pt: patellar tendon; t: tibia.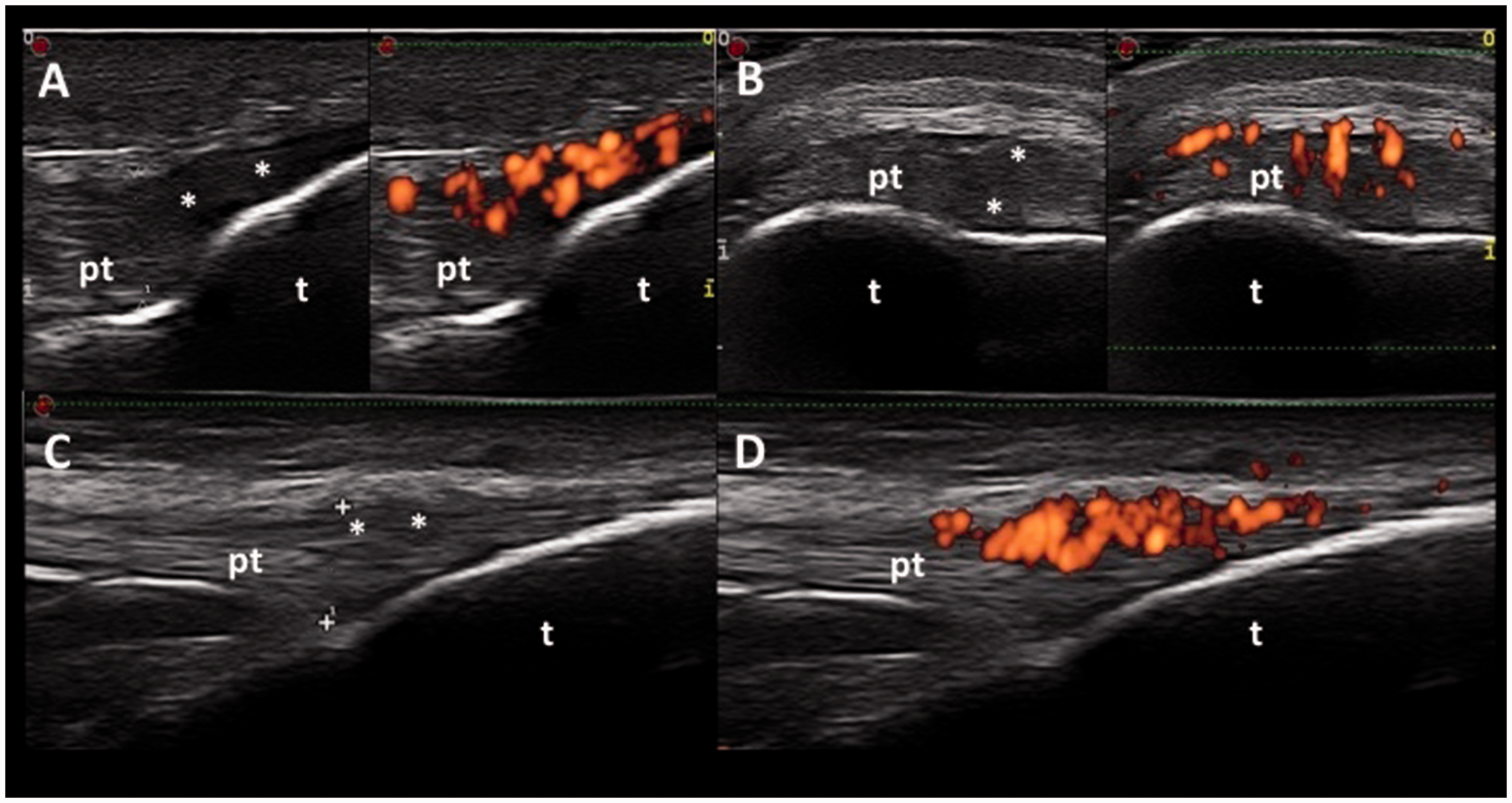
A diagnosis of SLE was established. Given the clinical manifestations and the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) score of 10, we started treatment with methotrexate (MTX) 10 mg/week subcutaneously, hydroxychloroquine (HCQ) 400 mg/day orally and oral prednisone 2.5 mg/day.
Case No. 2 (Patient F.B.)
The second patient is a 49-year-old male with no family history of rheumatic/autoimmune disease.
He was diagnosed with SLE in 1979, at aged 13. At that time the clinical picture included hands, wrists and knee synovitis, butterfly rash, leucopenia and ANA positivity (pattern not available). He was started on HCQ 400 mg/day orally and a variable dose of oral methylprednisolone depending on disease activity. In 1993, aged 27, he was admitted to the Cardiology Department due to persistent hypertension, proteinuria (1.5–2.0 g/day), macrohaematuria and raised creatinine. The patient was diagnosed with SLE glomerulonephritis (renal biopsy was not performed), and treated with oral methylprednisolone 0.75 mg/kg/day for four weeks with progressive renal function recovery. The methylprednisolone dose was gradually tapered to 4 mg/day and prescribed as a maintenance dose as was anti-hypertensive therapy (angiotensin-converting enzyme (ACE)-inhibitor and calcium channel blockers).
In February 2015, he was admitted to our department due to a severe lupus ‘flare’. This consisted of hands and feet arthritis, fever (body temperature over 38℃), oral aphthosis, malaise and extreme fatigue. Infection was fully excluded. Clinical examination of the hands revealed features of Jaccoud’s arthropathy: subluxation of several metacarpophalangeal (MCP) joints and Z-shaped deformity of both thumbs. Autoantibody profile confirmed ANA positivity (1:160, homogeneous pattern). Anti-dsDNA, anti-extractable nuclear antigen (anti-ENA), antiphospholipid antibodies, RF and ACPA results were negative. Complement proteins were reduced (C3 78 mg/dl, n.v. 88–200, C4 12.5 mg/dl, n.v. 16–47), ESR slightly increased (24 mm/h, n.v. < 15). Renal function, liver function and urinalysis were normal.
Hand and wrist X-rays did not show bone erosions. Hand, wrist, knee and ankle MSUS revealed bilateral wrists and second MCP joint synovitis (PD grade 3) other than bilateral third and fourth extensor tendon compartment tenosynovitis (PD grade 3). Signs of clinical enthesitis were not detected in the patellar, quadriceps, Achilles tendon or in the plantar fascia. Entheses MSUS revealed bilateral GS pathologic changes – areas of hypoechogenicity and entheseal thickening – and PD signal (grade 3) at the distal insertion of both patellar tendons. Entheseal thickening, hypoechoic areas and grade 2 PD signal were present at the right proximal patellar tendon insertion. Moreover, PD signal was found in the left deep patellar bursa (Figure 2). No MSUS abnormalities were detected in the other entheses.
Case No. 2 (Patient F.B). Left patellar tendon, distal insertion ((a) longitudinal scan – GS image; (b) longitudinal scan – PD image) and right patellar tendon, proximal insertion ((c) longitudinal scan – GS image; (d) longitudinal scan – PD image). The pictures show entheseal thickening (grey arrowheads and callipers), hypoechoic areas (asterisks) with loss of fibrillar echotexture and PD signal (grade 3 at left patellar tendon distal insertion, grade 2 at right patellar tendon proximal insertion). Bursitis of the left deep infrapatellar bursa (white arrowheads) is seen as a small amount of fluid filling the bursa with surrounding PD signal (red spots). GS: grey-scale; PD: power Doppler; pt: patellar tendon; t: tibia; p: patella.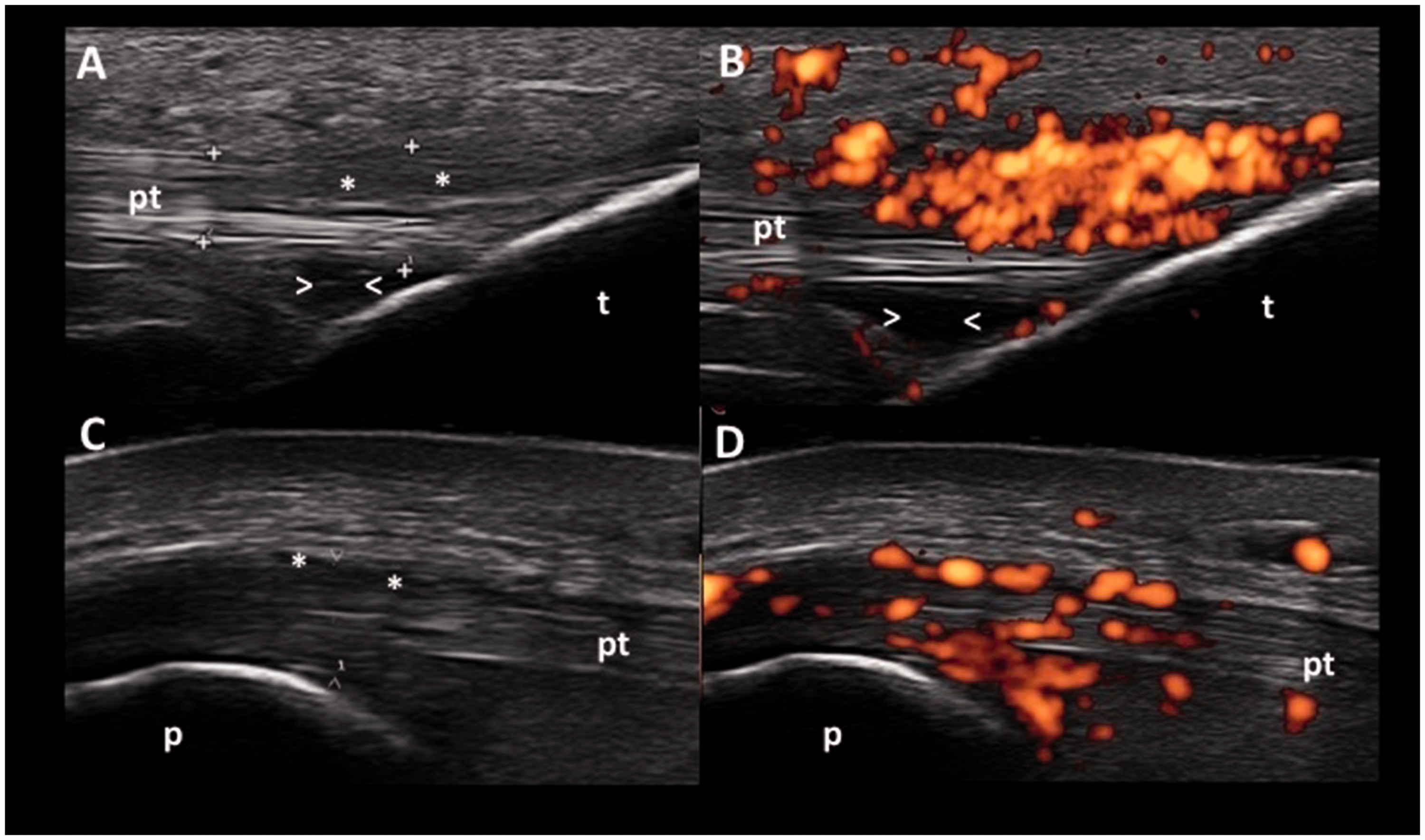
Considering the clinical features and the SLEDAI-2 K score of 9, we started treatment with MTX 15 mg/week subcutaneously, HCQ 400 mg/day orally and oral methylprednisolone (8 mg/day gradually tapered to the dose of 2 mg/day).
Case No. 3 (Patient M.F.)
The third patient is a 34-year-old female with no significant past medical history, no previous miscarriage and no family history of rheumatic disease.
In winter 2014, aged 33, she developed bilateral Raynaud’s phenomenon with painless hand and finger swelling and patchy alopecia. In July 2015 she was admitted to the Nephrology Department due to sudden onset of bilateral lower limb oedema. Other clinical features were dyspnoea, low-grade fever, malar rash, hand and wrist arthralgia, chest X-ray evidence of bilateral basal pleural effusions, pericardial effusion documented by echocardiogram, persistent proteinuria (24-hour urine collection proteinuria: 7500 mg/24 h, n.v. < 150 mg/24 h) with active urinary sediment (high number of red blood cells and white blood cells) and raised creatinine (1.9 mg/dl, n.v. 0.7–1.2 mg/dl). A renal biopsy was performed which confirmed glomerulonephritis (stage 4, activity index: 12, chronicity index: 2). ESR and CRP were slightly elevated. The autoantibody profile revealed increased anti-dsDNA (287 UI/ml, n.v. <10 UI/ml) and high-titre positivity of anti-Smith antibodies (anti-Sm).
Wrist, hand, knee and ankle MSUS revealed grade 2 PD signal tenosynovitis of the left fourth extensor tendon compartment. Clinical examination of patellar, quadriceps, Achilles tendons and plantar fascia enthesis did not elicit tenderness by pressure, mobilization or contraction against resistance and no soft tissue swelling was detected. Entheses MSUS revealed bilateral grade 2 PD signal and entheseal thickening with hypoechoic areas at the patellar tendon distal insertion and at the calcaneal insertion of the right Achilles tendon (Figure 3). No signs of inflammation (both in GS and PD mode) were found in the other entheses examined.
Case no. 3 (Patient M.F.). Right Achilles tendon, calcaneal insertion ((a) longitudinal scan – GS and PD image), left patellar tendon, distal insertion ((b) longitudinal scan – PD image) and right patellar tendon, distal insertion ((c) longitudinal scan – GS and PD image). The pictures show entheseal thickening, hypoechoic areas (asterisks) and grade 2 PD signal (red spots). GS: grey-scale; PD: power Doppler; at: Achilles tendon; c: calcaneus; pt: patellar tendon; t: tibia.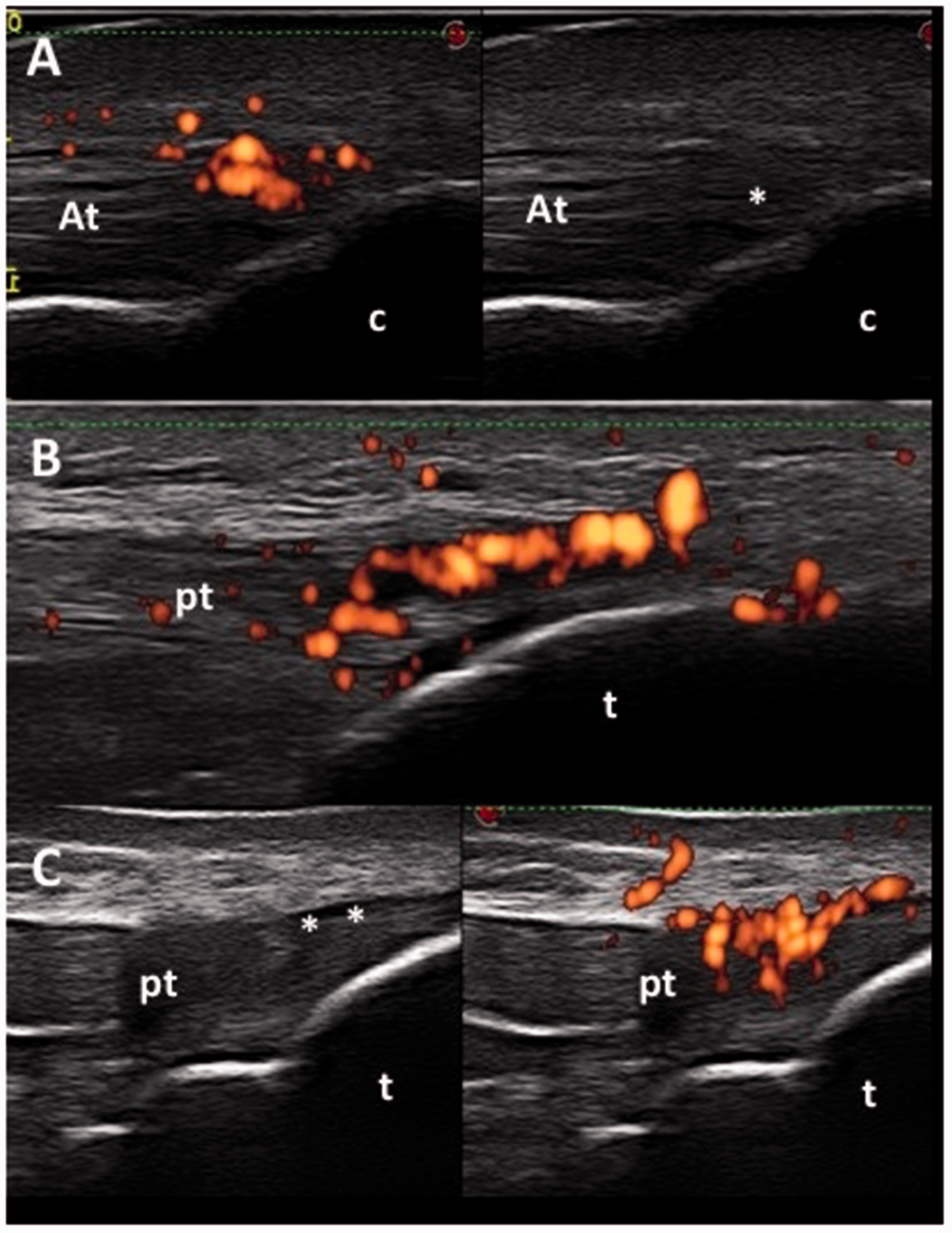
A diagnosis of SLE was established. SLEDAI-2K score was 24. She was started on mycophenolate (2 g/day orally), antihypertensive therapy (ACE-inhibitor and diuretic), pulsed intravenous methylprednisolone (500 mg/day for three days) switched to oral formulation and gradually tapered to a dose of 4 mg/day.
Case No. 4 (Patient G.A.)
The fourth patient is a 47-year-old female affected by autoimmune thyroiditis.
In winter 2000 she was evaluated in another Rheumatology Department because of the onset of Raynaud’s phenomenon associated with photosensitivity and hand, wrist and ankle synovitis. Autoantibody profile revealed: ANA 1:640 (speckled pattern), anti-U1RNP 120 U/ml (n.v, 0–10), anti-Sm 120 U/ml (n.v. 0–10), anti-SSA/Ro 75 U/ml (n.v. 0–5), RF 54.7 UI/ml (n.v. <30), Coombs test positive. HLA B-27 was absent. The nailfold capillaroscopic exam showed a ‘scleroderma pattern slow’. Chest high-resolution CT scan did not show any evidence of interstitial lung disease. The patient was diagnosed with undifferentiated connective-tissue disease (UCTD) and treated with HCQ (400 mg/day orally), nonsteroidal anti-inflammatory drugs and calcium channel blocker, with benefit for the next nine years. Although Raynaud’s phenomenon persisted, mainly in the winter seasons, she did not develop digital ulceration or skin thickening.
In September 2014 the clinical picture was characterized by wrist, hand and feet synovitis, Raynaud’s phenomenon and hypertension. Haematological investigations showed: ANA 1:1280 (specked pattern), anti-dsDNA 49 IU/ml (n.v. <15), anti-Sm 145 U/ml (n.v. 0–10), anti-U1RNP 724 U/ml (n.v. < 10), anti-SSA/Ro 722 U/ml (n. v. <10), anti-SSB/La 55 U/ml (n.v. <10), ACPA 0.9 U/ml (n.v. < 10), RF 47.4 UI/ml (n.v. <20). Complete blood cell count, renal function, liver function and urinalysis were normal. ESR and CRP were slightly elevated and C3 was reduced (67 mg/dl, n.v. 88–200). The nailfold capillaroscopic exam revealed non-specific abnormalities. The cause of the hypertension was related to a massive but benign liver haemangioma (15 cm × 13 cm) compressing the right kidney, which was documented by ultrasound, CT scan and magnetic resonance imaging.
Hand and feet X-rays showed bilateral bone erosions of the second MCP and fifth metatarsophalangeal (MTP) joints. Bilateral synovitis of the second, third and fourth MCP joints and of the third, fourth and fifth right interphalangeal (PIP) joints was revealed by MSUS. Tenderness by contracting against resistance was elicited at the tibial insertion of the right patellar tendon. The patient, moreover, reported previous episodes of pain at the right knee level without specific distribution. MSUS of entheses revealed grade 3 PD signal, hypoechoic areas and entheseal thickening at the distal insertion of the right patellar tendon and grade 2 PD signal with hypoechoic areas at the tibial insertion of the left patellar tendon (Figure 4). No MSUS pathological findings were detected in the other entheses examined.
Case no. 4 (Patient G.A.). Right patellar tendon, distal insertion ((a) transverse scan – GS image and PD image; (b) longitudinal scan – GS and PD image) and left patellar tendon, distal insertion ((c) longitudinal scan – GS image and PD image). The pictures show thickened distal patellar tendons enthesis, more evident on the right side, hypoechoic areas (asterisks) and PD signal (grade 3 at the right patellar tendon enthesis, grade 2 at left patellar tendon enthesis). GS: grey-scale; PD: power Doppler; pt: patellar tendon; t: tibia.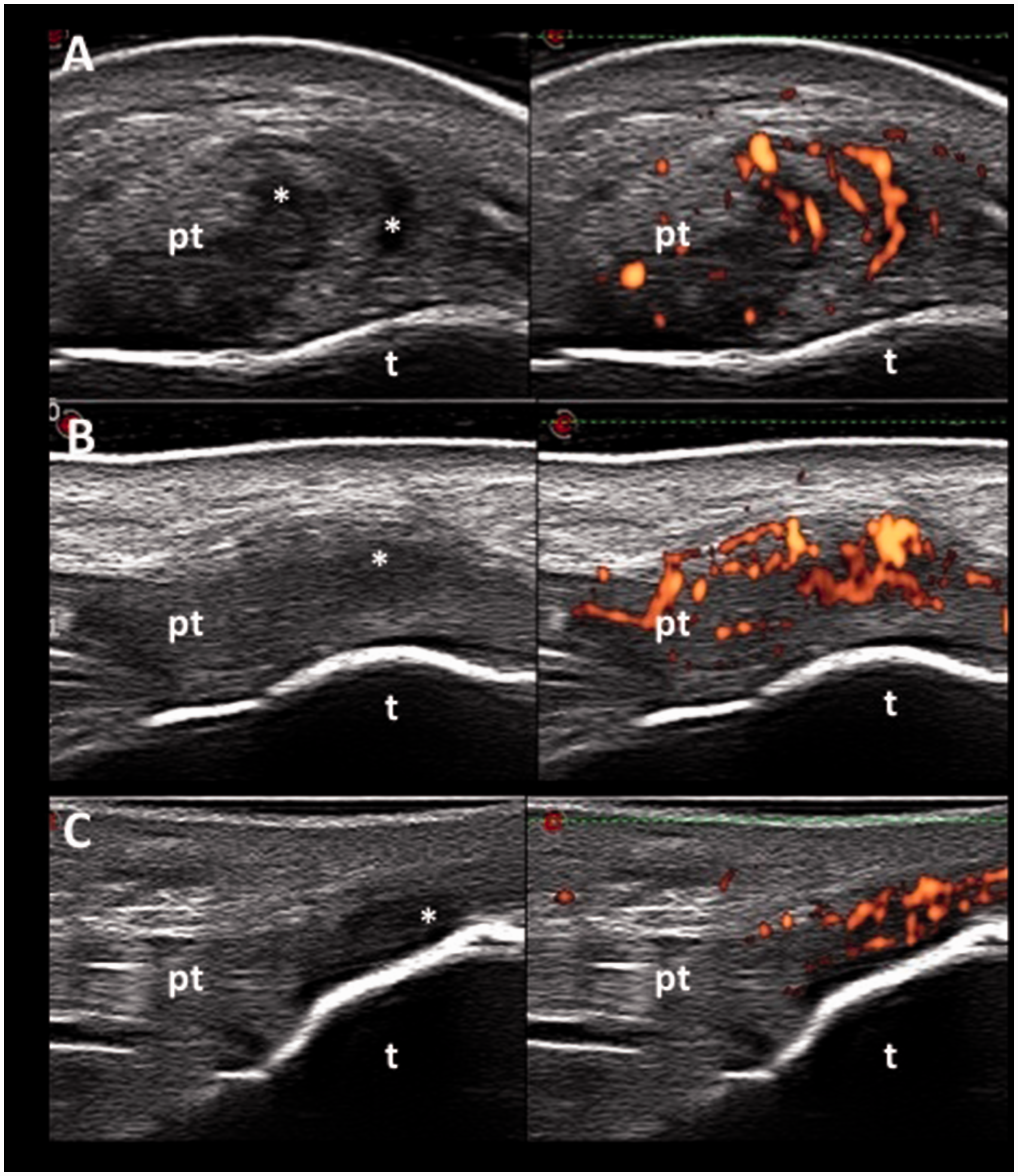
The diagnosis of SLE and rhupus arthropathy was made. SLEDAI-2K was 8. We opted for MTX (10 mg/week subcutaneously), HCQ (400 mg/day orally) and oral methylprednisolone (2 mg/day). Surgeons have not removed, for the moment, the liver haemangioma, opting for a radiological follow-up.
Discussion
Anecdotal overlap between SLE and seronegative spondyloarthropathies has been described (i.e. sacroileitis, 25–28 psoriasis 29 ). To the best of our knowledge, our case series shows for the first time unequivocal and relevant MSUS findings of enthesitis in four patients with adult SLE. All of them presented with inflammatory involvement of the hands and wrists (clinical and/or revealed by MSUS) and moderate-to-high disease activity as assessed by the SLEDAI-2K. Of interest is that three out of four patients did not show any clinical signs of enthesitis (Case 1, Case 2 and Case 3). Intense PD signal was the most relevant MSUS pathological finding. Entheseal thickening and hypoechoic areas represented the main GS findings. The tibial insertion of the patellar tendon was the most frequently affected area. Pattern analysis of the ultrasound images reveals the prevalent involvement of the tendinous side of the enthesis, whereas signs of bone reaction or damage including enthesophytes, calcifications and bone erosions were not detectable. Due to the small sample size of this case series, it is not possible to draw any definitive conclusion regarding pathophysiology and/or clinical relevance of entheseal involvement in SLE. However, the detection of MSUS enthesitis in patients without other predisposing factors for enthesopathy indicates that enthesis, especially of the patellar and Achilles tendon, could be a missing target in the evaluation of SLE patients. Case 1 and Case 4 presented clinical and serological characteristics indicative of a possible overlap with a different autoimmune disease. Further investigation in a large cohort of patients is required to determine whether these characteristics may be positively correlated to tendon involvement. Although the inflammatory process in SLE is traditionally attributed to synovial tissue areas, subclinical inflammation at the entheseal level should not be regarded as a surprising finding considering the multisystemic inflammatory involvement of SLE. The absence of a systematic MSUS assessment of enthesis in SLE patients might explain why enthesis has not been considered among the possible targets of the disease. We believe that the presence of MSUS enthesitis in asymptomatic patients should not be ignored. Subclinical inflammation could lead to tendon mechanical resistance weakening thus representing a potential risk factor for a subsequent tendon rupture. Of interest is that most of the tendon ruptures in patients with SLE occur at the patellar tendon level. 30 In our case series, Case no. 2 showed a vast area of derangement of the typical echotexture of the patellar tendon, with a high-degree PD signal (Figure 2(a)). If these lesions were confirmed as imaging biomarkers of a process that may potentially affect the tendon mechanical resistance, other well-known independent risk factors for tendon rupture such as corticosteroid therapy, quinolones, and/or local mechanical stress and strain should be considered and, if possible, avoided in these patients.
Conclusions
The detection of unequivocal MSUS findings of enthesitis in a group of SLE patients was unexpected. This case series is small but opens a window to the potential entheseal involvement in SLE which is a still unexplored area of research. We believe that more attention should be paid to patellar and tendon entheses even in asymptomatic SLE patients. Further investigations are needed in order to define SLE entheseal involvement prevalence and clinical relevance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.