
Abstract
Background
Systemic lupus erythematosus (SLE) is an autoimmune disease with presence of autoantibodies and characteristic multi-organ involvement. Relatives of SLE patients have an increased risk of autoantibody production and autoimmune diseases.
Methods
In 2001, 226 first degree relatives (FDRs) of a population-based cohort of SLE patients were examined for the prevalence of autoantibodies and self-reported health complaints. In 2013, 143 FDRs were re-investigated and deceased’s medical records were examined.
Results
Participants and non-participants were comparable regarding baseline characteristics, while deceased FDRs were older than participants, but with comparable ANA status. ANA status at baseline correlated to ANA status at follow-up. At follow-up, two FDRs reported SLE and 15 FDRs other autoimmune diseases. No observation at baseline alone could predict self-reported health. During follow-up 33 died at median age 76 years. Three deceased FDRs were diagnosed with an autoimmune disease.
Conclusion
The study showed that FDRs of SLE patients have an increased prevalence of ANA compared to healthy controls. The prevalence increased during follow-up, and ANA positive FDRs at baseline were prone to be ANA positive at follow-up. ANA positive FDRs had more self-reported autoimmune diseases, including SLE and rheumatoid arthritis, than reported from other population-based investigations.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by the presence of autoantibodies and multi-organ involvement. 1 The pathogenesis of SLE is not fully understood, but central factors are inadequate clearing of apoptotic material, 2 hyper-reactive B cells 3 and insufficient T-cell regulation,3,4 leading to autoantibody production. 1 Antinuclear autoantibodies (ANA) can be detected several years prior to symptoms and diagnosis of SLE. 5
The development of SLE may partly be due to genetic factors, as indicated by the clustering of SLE in certain families.6–8 Higher concordance of SLE has been demonstrated in monozygotic twins compared to dizygotic twins, 9 and gene studies have shown that certain genes are correlated to an increased risk of SLE. 10 Previous studies have shown a higher prevalence of autoantibodies among first degree relatives (FDRs) of SLE patients11–14 and increased risk of autoimmune diseases compared to the background population.7,15,16
Denmark is a country with low incidence of SLE, 17 and SLE tends to have a milder course in Danish patients compared to patients from other countries. 18
In the present study, a 12-year follow-up was done on FDRs of a population-based cohort of SLE patients. At baseline, FDRs were examined for selected autoantibodies and self-reported health complaints. 12 The aim of the present study was to investigate if observations at baseline could predict autoantibody status, self-reported health complaints and death after 12 years of follow-up.
Materials and methods
In the baseline study 12 years prior to the present study, all FDRs of a population-based SLE cohort were examined for the prevalence of autoantibodies including ANA and anti-double stranded DNA (dsDNA) and self-reported health using a questionnaire. 12 All living FDRs were re-invited after 12 years and received oral and written information. Questionnaires and blood samples were collected. After consent from relatives of deceased FDRs, medical records of the deceased were reviewed.
A control group of 200 healthy individuals (blood donors) was used as a reference population for autoantibodies in both studies. As regards self-reported health, no reference population was used.
Blood samples from FDRs were collected by the FDR’s general practitioners or by the first author, and serum was frozen at -80℃. ANA and dsDNA analyses were performed using the same methodology as in the baseline investigation: ANA was tested in indirect immunofluorescence using HEP-2 cells in monolayer titres 1:40, 1:80 and 1:160, 19 and dsDNA was tested by the ELISA technique at dilution 1:100 by a commercial kit (Varelisa dsDNA, by Phadia, now Thermo Scientific). All tests were done in duplicate and noted as positive or negative.
The questionnaire from the baseline investigation was used again, with one additional question concerning current and former smoking habit. 20
Deceased FDR’s medical records were reviewed by the first author. Diagnoses, cause of, and age at death were registered. When information was missing the general practitioner of the deceased was asked for additional data.
Statistics
Significance levels were set at 5%. Comparison of continuous and normally distributed data was performed using Student’s t-test and given as mean with 95% confidence intervals. Not-normally distributed data were given as median and range. Dichotomous data were analysed with the χ 2 test, when limited by small numbers using Fisher’s exact test. Categorical ranked data were analysed with the Wilcoxon–Mann–Whitney test and, when not ranked, the Kruskal–Wallis test. Development of ANA status from baseline to follow-up was analysed with logistic regression and adjusted for gender and age. The number of participants in the groups limited the analyses from including more variables.
Ethics
The study was approved by the local ethics committee of the Region Southern Denmark (Project ID: S-20120146).
Results
Of the 226 FDRs from baseline, 143 participated in the present study (Figure 1). Thirty-three had died and the medical records of 29 (88%) were investigated.
Flowchart showing FDRs at baseline and at follow-up.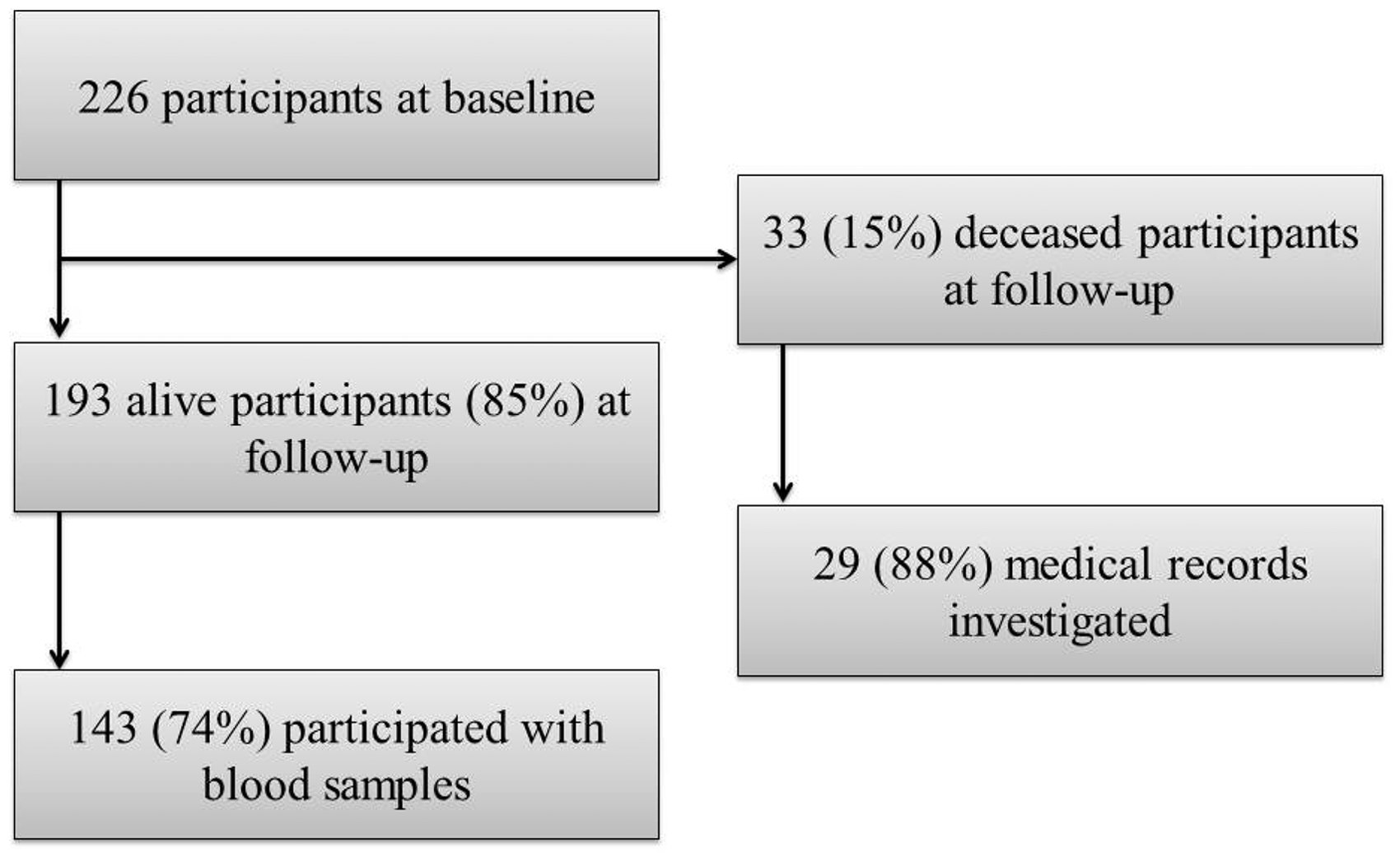
Characteristics of participating and non-participating alive FDRs with respect to age, gender, family relation, oral contraceptives (OC), hormone replacement therapy (HRT) and ANA status
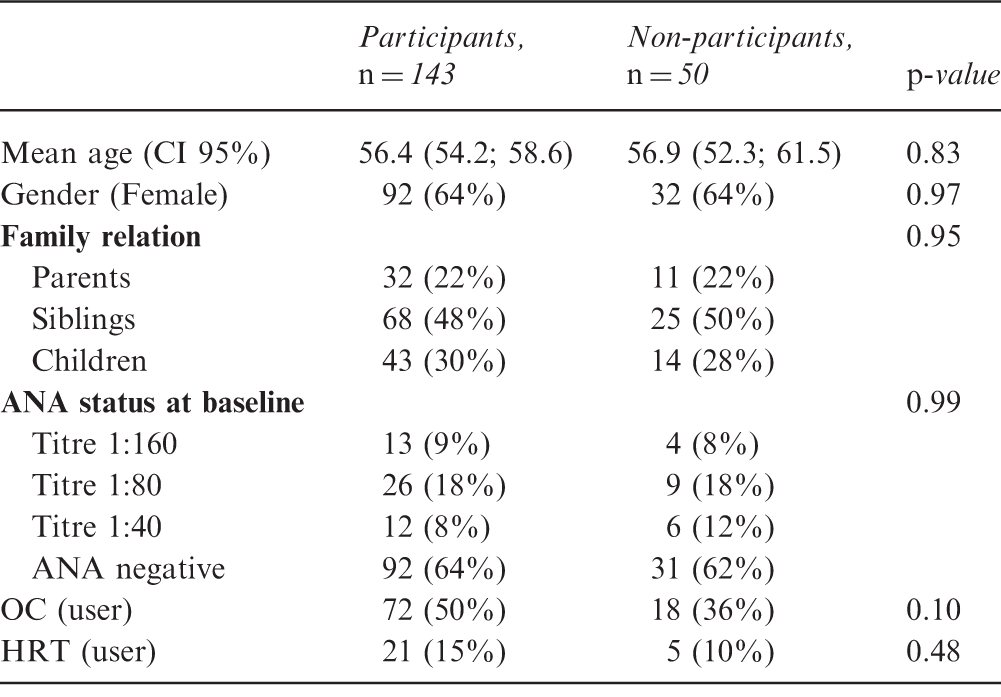
HRT: hormone replacement therapy; OC: oral contraceptive
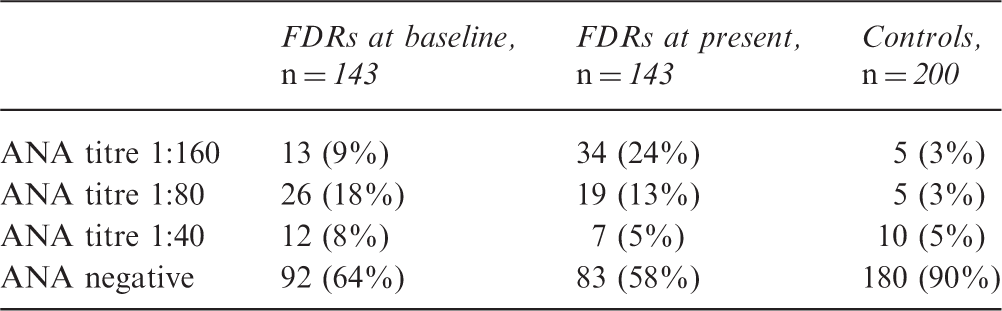
ANA status in FDRs in the present study, at baseline and in controls
Observed and expected numbers of ANA positive FDRs, at baseline (rows) and in the present study (columns)
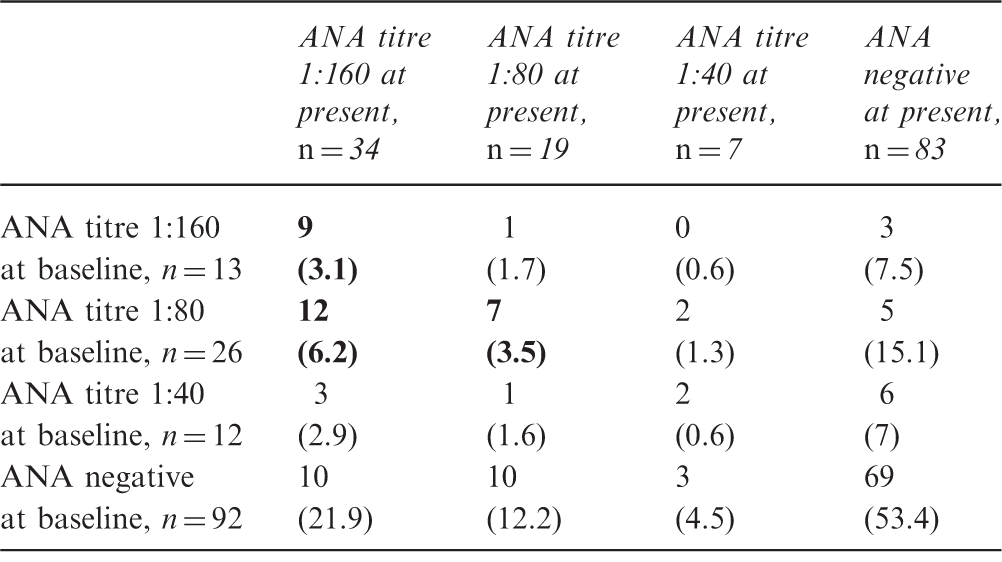
Upper number is the observed number and the number in brackets denotes expected the number if ANA titres were randomly distributed. Baseline ANAs at higher titres (>1:80) were associated with high titres at follow-up (bold).
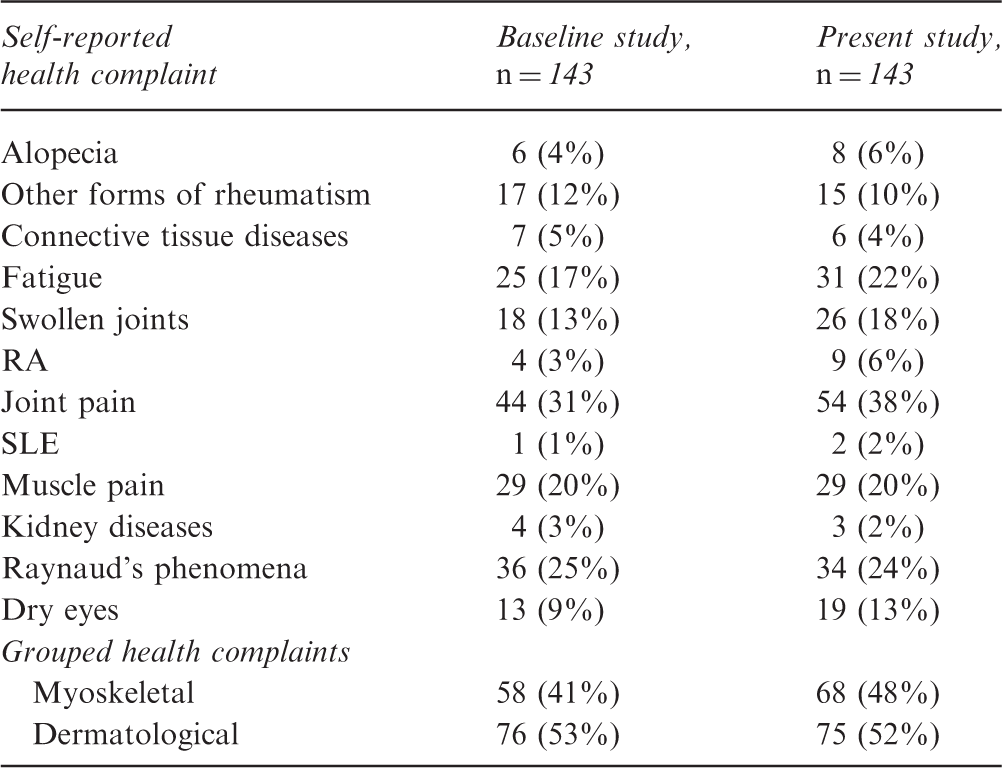
Distribution of selected self-reported health at baseline and at present
In a multiple regression model, ANA at present was predicted by ANA at baseline (p < 0,001 in all three titres) but not by gender or age. No single baseline health complaint was correlated with development of ANA at present. The number of participants limited the number of variables in a logistic regression analysis; hence, several combinations of health complaints could not be investigated. Baseline ANA positivity at titre 1:80 or higher was correlated to rheumatoid arthritis (RA) at follow-up, but not to any other self-reported health complaint. The nine FDRs who were repeated ANA positive at titre 1:160 did not have more self-reported health complaints in total, or any single health complaint, compared with the remaining FDRs.
The prevalence of dsDNA positivity among FDRs showed an increasing tendency from 0.7% at baseline to 4% in the present study (p = 0.12). Among healthy blood donors 1% was dsDNA positive. No autoantibody or self-reported health complaints at baseline could predict dsDNA status in the present study (data not shown).
FDRs testing positive of any autoantibody at either baseline or in the present study tended to have more self-reported health complaints at follow-up compared with FDRs consistently autoantibody negative, including muscle pain (25% vs 17%, p = 0.224), joint pain (40% vs 36%, p = 0.663), RA (13% vs 2%, p = 0.028) and alopecia (9% vs 3%, p = 0.260).Correcting for age in logistic regression did not make the results less significant in general. Smoking status, oral contraceptives and hormone replacement therapy did not show any relation to ANA or dsDNA status.
Two FDRs reported to have SLE, but only one was ANA positive. The other was negative of all autoantibodies at both baseline and follow-up. Six FDRs reported to have ‘other connective tissue diseases’ (OCTD), but there were no correlations to autoantibody status at baseline and follow-up.
Four FDRs reported to have RA at baseline and follow-up and an additional six reported to have RA at follow-up (6% in total), while one stopped reporting RA at follow-up. Four of the six incidents of self-reported RA (67%) were ANA positive at baseline (titre 1:160 or 1:80). Seven of the nine reporting RA at follow-up were females, with a median age of 58 years (range 43–80). Except from ANA, no baseline observation could predict the development of self-reported RA.
Deceased FDRs had a median age of 76 years (range 48–91 years). Three out of 29 (10%) deceased FDRs had a diagnosis of rheumatic or autoimmune disease at the time of death: one had retroperitoneal fibrosis, one had granulomatosis with polyangiitis and one had polymyalgia rheumatica. The FDR with retroperitoneal fibrosis had a positive ANA in titre 1:160 at baseline; the other two were not positive for any autoantibody. No baseline health complaint or autoantibody could predict death during the 12 years follow-up (data not shown).
Discussion
In this follow-up study we demonstrated ANA positivity in significantly more FDRs compared to healthy controls. This is in line with previous reports.12,21,22 The prevalence of high-titre (1:160) ANA positivity in FDRs increased to 24% during 12 years of follow-up. Navarra et al. have reported a prevalence of 9% 21 and Ramos et al. reported 16% ANA positive at titre 1:120. 22 An increasing prevalence of autoantibody positivity with increasing age has been described before23–25 and is believed to be a result of several mechanisms including ‘subclinical’ autoimmunity increasing with age, usage of certain drugs and environmental exposures. 24 Corresponding to our findings, Nass et al. demonstrated that relatives of patients with celiac disease testing positive for an autoantibody at baseline tended to have a higher prevalence of autoantibodies at follow-up. 26
Interestingly, Xavier demonstrated persistent ANA positivity for four years in a cohort of elderly (mean age 73.2 years), but none of the ANA positives developed autoimmune disease during follow-up. 25 In the present study we did, however, demonstrate that persistent high-titre positivity was also found in younger FDRs. This indicates that persistent ANA positivity may be reserved to certain subgroups not only defined by increasing age. Continued surveillance for development of autoimmune disease still seems appropriate, considering a mean age among repeated ANA positives of 46.9 years.
As autoimmune disease may be considered a result of the interaction of autoantibodies with the immune system, resulting in clinically well-defined autoimmune diseases,27,28 it is noteworthy that repeated ANA positivity was not associated with any specific health complaints in this study. An important reservation in this analysis is the relatively low number of FDRs investigated, resulting in an expectance of few incident cases of autoimmune diseases in a 12-year period. Results from Arbuckle et al. did convincingly demonstrate that SLE patients develop autoantibodies several years prior to a diagnosis of SLE. 5
Smoking has been linked to the development of RA and SLE. 29 In our study there was no association between self-reported former or current smoking and the presence of autoantibodies. Young et al. found a weak correlation between former smoking and production of anti-Ro, but otherwise no connection between autoantibody production and smoking among FDRs to SLE patients. 30
Self-reported health included two FDRs reporting SLE, corresponding to a roughly estimated incidence of one per 1000 person-years, as compared to a Danish population-based study reporting an incidence of SLE of one per 100,000. 17 Self-reported SLE should also be critically reviewed, considering only one ANA positive in our analyses. On the other hand, FDRs could have extra knowledge about connective tissue diseases and therefore offer better self-reporting of this disease. In Iceland and Sweden SLE multiplex families have been described, 8 whereas this has until now not been the case in Denmark.
RA was reported by nine FDRs, corresponding to an estimated point prevalence of 6% among the FDRs. Of the nine, six were incident reports of RA corresponding to a crude estimate of 350 per 100,000 person-years among FDRs compared to an estimated incidence of RA in Denmark of 0.35 per 100,000 person-years. 31 Unfortunately, it was not possible to verify diagnoses within this study. The finding of more than expected self-reported RA and SLE, and the finding of reported rare autoimmune diseases among the deceased, all point towards a higher prevalence of autoimmune disease among FDRs. This is in agreement with previous studies reporting an increased presence of autoimmune diseases among FDRs compared to the background population.6,7,15 Still, the predictive value of ANA positivity was disappointing, as only six of 51 (12%) of the baseline ANA positive FDRs developed a self-reported autoimmune disease (RA, SLE and OCTD) compared to eight of 92 (9%) of the baseline ANA negative FDRs after 12 years of follow-up. ANA’s predictive value was most prominent in regards of RA, where four of six who developed RA were ANA positive at baseline. Hence, in this study relatives initially tested positive of ANA rarely develop autoimmune disease during 12 years of follow-up.
It has been debated if one should treat certain individuals prophylactically with immune modulating medicine to prevent the development of SLE.32,33 Our results do unfortunately not give any extra help for selection of possible subjects among relatives to SLE patients for prophylactic treatment.
The strengths of this study are a well characterized population of FDRs to SLE patients reporting health complaints using a well-defined questionnaire. Weaknesses include few cumulated years of follow-up in order to study rare events such as SLE and RA and the lack of evaluation of self-reported diseases.
Conclusion
FDRs to SLE patients are more prone to develop autoantibodies compared to healthy controls. If FDRs develop autoantibodies, they tend to stay autoantibody positive. FDRs reported more rheumatic diseases compared to the background population. ANA positive FDRs tended to have more self-reported autoimmune diseases, including SLE and RA, than reported from other population-based investigations.
Footnotes
Acknowledgements
The authors would like to thank all study participants for their contribution, and the SLE patients of providing relatives to investigate. We also like to thank the staff at the Rheumatic Department of Odense Universitetshospital and the participant’s general practitioners, who helped make the study possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.