
Abstract
Objective
This study aimed to validate the Japanese version of the LupusPRO questionnaire for use with systemic lupus erythematosus patients.
Methods
Participants were 205 lupus patients recruited from three rheumatology centers in Japan. Demographic data were collected and quality of life was assessed using the LupusPRO and the Short Form Health Survey-12. Disease activity was evaluated by physicians using the Systemic Lupus Erythematosus Activity Index. Some participants completed questionnaires 10–14 days after the first survey. Internal consistency reliability, test-retest reliability, content validity and convergent validity were examined, and confirmatory factor analysis was performed.
Results
Participants’ mean age was 47.8 ± 13.6 years. Older participants scored lower on physical quality of life and higher on coping than younger participants. The LupusPRO showed satisfactory test-retest reliability (n = 111). Test-retest reliability was lower for the mental and social aspects of quality of life, indicating fluctuations in quality of life during the two-week interval. Internal consistency reliability was good and convergent validity with the corresponding domains of the Short Form Health Survey-12 was satisfactory. Confirmatory factor analysis showed a good model fit.
Conclusion
The Japanese LupusPRO is a reliable and valid measure to evaluate treatment interventions for systemic lupus erythematosus.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease that results in multiple organ damage. 1 Advances in medical treatment have substantially improved SLE survival rates, and the number of elderly SLE patients is expected to increase. 2 SLE patients have lower quality of life (QoL) than rheumatoid arthritis patients.3–6 Five QoL scales have been developed to investigate SLE patients’ perspectives on the impact of the disease;7–11 however, none of these scales have been translated into Japanese.
One of these SLE-specific QoL scales is the Lupus Patient Reported Outcome Too (LupusPRO), which was developed in the United States. 11 It measures procreation, coping, desires/goals and satisfaction with care, which are not addressed by the other SLE-specific scales. The LupusPRO has been used to evaluate the effect of interventions12,13 and has been translated into four languages, including Spanish, French, Turkish and Chinese.14–17 The LupusPRO has been validated in several English-speaking countries.18,19
The purpose of this study was to establish the reliability and validity of the Japanese version of the LupusPRO. Japanese SLE patients are unique, as they are covered by a special medical assistance program that covers almost all medical expenditure. Easy access to medical care means that Japanese samples are more varied in age and represent a greater range of disease duration than samples in previous validation studies.11,14–17
Methods
Translation and establishment of the reliability and validity of the Japanese LupusPRO
The LupusPRO comprises two constructs: health-related QoL and non-health-related QoL. The health-related QoL domains are (1) lupus symptoms, (2) cognition, (3) lupus medications, (4) procreation, (5) physical health, (6) pain/vitality, (7) emotional health and (8) body image. The non-health-related QoL domains are (1) desires/goals, (2) social support, (3) coping and (4) satisfaction with care. In total, the LupusPRO comprises 43 items (30 for the health-related QoL construct, 13 for the non-health-related QoL construct) that relate to the past four weeks in the patient’s daily life. Each item is scored on a five-point Likert scale ranging from “none of the time” to “all of the time.” The score for each domain ranges from 0 to 100; higher scores indicate better QoL.
We obtained permission to develop the Japanese version of the LupusPRO from Dr Meenakshi Jolly, the author of the original version. The LupusPRO was translated by the first author following the guidelines for translation of the instrument. 20 The Japanese version was back-translated. It was compared with the original scale, and minor modifications were made to the Japanese version. The face validity of the Japanese version was tested by four SLE patients and an expert panel (three rheumatologists and two nurses), and minor changes were made to clarify the wording. Then, the expert panel was asked to evaluate each item using a Likert scale ranging from 1 (not relevant) to 4 (highly relevant). We calculated the content validity index for each item and the mean content validity index for the scale. Content validity indices for the scale and for each item were tabulated. A cutoff of 0.90 21 was considered the minimum acceptable validity.
Participants
We recruited outpatients at three rheumatology centers (university hospital, city hospital, private hospital) in western Japan between June 2015 and February 2016. Eligibility criteria were (1) age ≥20 years, (2) meeting the American College of Rheumatology classification criteria for SLE, 22 (3) ability to complete the self-administered questionnaires in Japanese and (4) written informed consent to participate in the study. An age of ≥20 years was chosen as this is the legal age of adulthood in Japan; therefore, participants did not require parental consent to take part. Consecutive patients who attended the outpatient department were screened for eligibility and were contacted by the first author. The exclusion criteria were (1) a major comorbidity that would affect QoL, such as the terminal stage of cancer and (2) overlap with other autoimmune diseases, such as rheumatoid arthritis.
Ethical considerations
This study was approved by the Ethics Committee of Osaka University and three rheumatology centers (ethics committee approval numbers: 14505 (319)-2). At the initial contact with the participants, the first author provided a verbal and written explanation to confirm their willingness to participate. After obtaining written informed consent, the first author distributed the questionnaires to participants.
Data collection
The self-administered questionnaires were used to collect demographic information, information about SLE duration and QoL data using a generic health-related QoL tool (Medical Outcomes Study Short Form Health Survey-12, SF-12) 23 and the LupusPRO. The following demographic information was obtained: gender, age, educational attainment, employment status and family structure. The SLE Disease Activity Index (SLEDAI) 24 was used to determine disease activity, and information on current SLE medications was collected. The SLEDAI information was abstracted from electronic medical records by the primary physician and included laboratory results, health history since last visit and physical examination data. A flare was defined as an increase of ≥3.0 in the total SLEDAI score between the previous visit and the date of the survey. 24
To examine test-retest reliability, approximately half the participants, 127 patients, were asked to fill out the questionnaires 14 days after the first survey and return them to the first author in a pre-stamped addressed envelope. An interval of 14 days was chosen following previous recommendations for reliability testing of psychometric scales, which all specify a 14-day interval and advocate a range of two days to four weeks.25–27
Statistical analyses
Descriptive statistics were calculated for all variables. Then, demographic and QoL data were stratified by two age groups (<50, ≥50 years) by biological reproductive age, a definition used by the World Health Organization. 28 This age cutoff point was chosen for age stratification because the procreation subscale score could have affected the LupusPRO health-related QoL score. T-tests were used for parametric variables and Wilcoxon rank-sum tests were used for non-parametric variables to test the statistical significance of differences between the two age groups.
Cronbach’s alpha was used to examine internal consistency for each LupusPRO domain; an alpha of >0.7 was considered acceptable. 29 Correlation coefficients between item scores at the two time points were calculated to assess test-retest reliability.
Content validity, convergent validity and construct validity were evaluated. Content validity was evaluated using the content validity index for the scale and the indices for each item; a coefficient >0.9 was considered acceptable. 21 Convergent validity was evaluated using Spearman’s correlations between the LupusPRO domains and the corresponding SF-12 domains.
To test construct validity, a confirmatory factor analysis of the LupusPRO item responses was performed using a robust weighted least squares estimator. The goodness of fit of the hypothesized item-to-scale relationships was evaluated using the comparative fit index, the Tucker-Lewis index (which is also a comparative fit index) and the root mean square error of approximation. The comparative fix index and the Tucker-Lewis index quantify the difference between the examined and independence model; higher scores indicate larger differences. The root mean square error of approximation quantifies the difference to the fully saturated model. It is generally recommended that acceptable fit requires a comparative fit index and Tucker-Lewis index ≥0.9030,31 and a root mean square error of approximation ≤0.08. 32
JMP 11 (SAS, Cary, NC, USA) was used for descriptive analysis and SPSS Amos 24 (IBM, Armonk, NY, USA) was used for confirmatory factor analysis. All reported p values are two tailed, and p values <0.05 were considered statistically significant. There are several adjustment methods available for multiple comparisons; however, they tend to increase type II errors. 33 Therefore, we did not adjust for type II errors.
Results
The content validity indices for the scale and each item of the Japanese LupusPRO were evaluated by five experts. The mean content validity index for the scale score was 0.99, and the mean content validity index for each item score was 0.99.
Descriptive data for the study participants
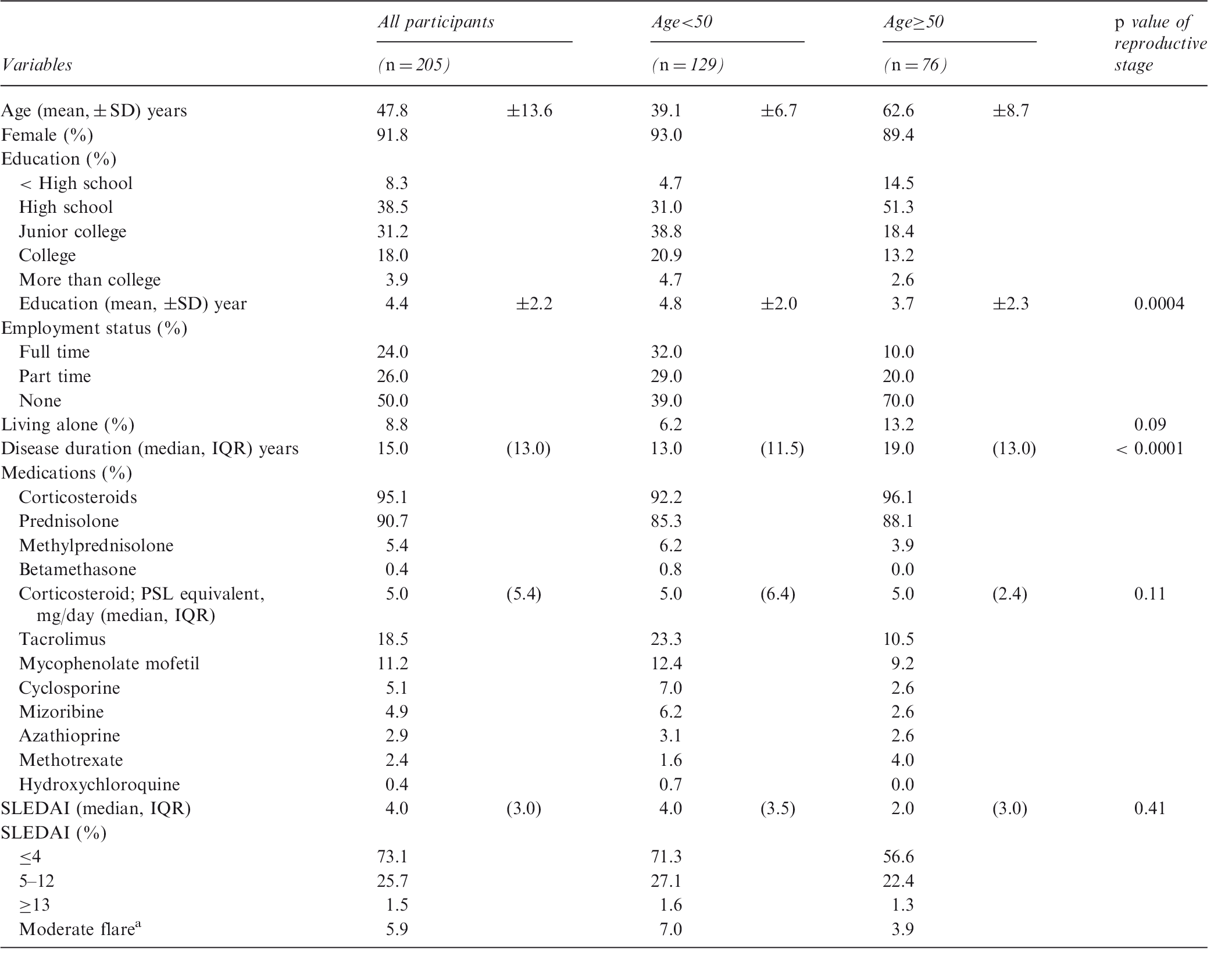
IQR: interquartile range; PSL: prednisolone; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; aA flare was defined as an increase of ≥3.0 in the total SLEDAI score between the previous visit and the date of the first survey.
Participants <50 years (hereafter, the younger group) had significantly more years of schooling than participants ≥50 years old (hereafter, the older group). The younger group had significantly shorter disease duration than the older group. There was no difference in disease activity (based on SLEDAI scores) and corticosteroids use between the two age groups. In contrast, the use of immunosuppressive drugs was more common in the younger group (Table 1).
Regarding generic QoL, SF-12 scores were higher for physical function, body pain and social function, and lower for vitality. After stratifying by age, the younger group had significantly higher median scores for the three physical domains, but lower median scores for mental health, than the older group.
Descriptive statistics for LupusPRO and SF-12 scores in Japanese lupus patients (0 = worst QoL, 100 = best QoL)
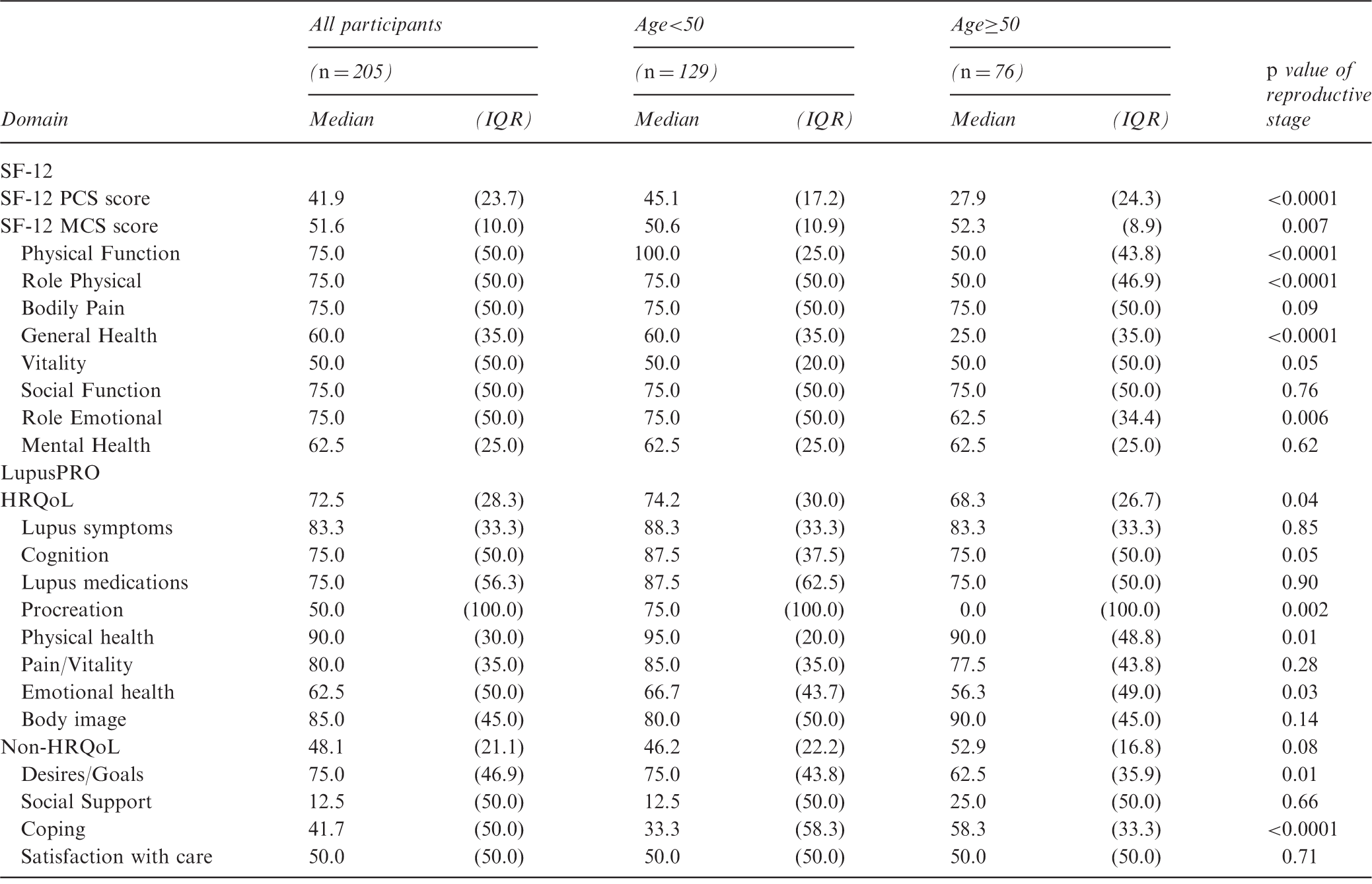
HRQoL: health-related quality of life; IQR: interquartile range; MCS: Short Form Health Survey-12 mental component summary score; PCS: Short Form Health Survey-12 physical component summary score.
Of the 12 LupusPRO domains, Cronbach’s alpha did not reach 0.7 for four domains (lupus symptoms, lupus medications, social support and coping).
Reliability and validity of the Japanese LupusPRO
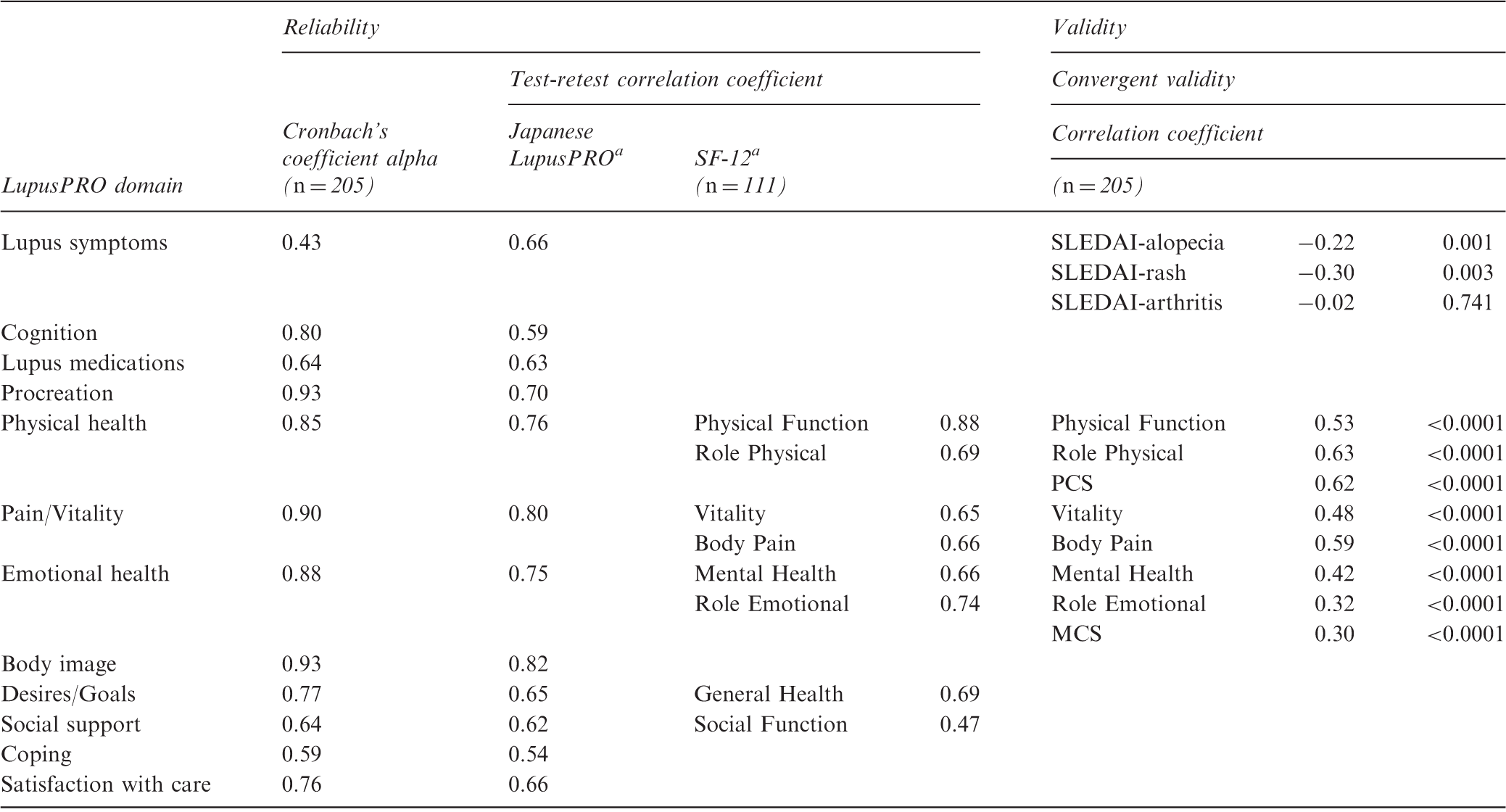
MCS: Short Form Health Survey-12 mental component summary score; PCS: Short Form Health Survey-12 physical component summary score; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index. aAll p values for test–retest correlation coefficients were <0.0001.
Convergent validity was tested using the SLEDAI subscales; SLEDAI-alopecia and SLEDAI-rash had significant but weak inverse correlations. Convergent validity of the three LupusPRO domains was examined by calculating correlations between the LupusPRO domains and the corresponding SF-12 domains. Physical health, pain/vitality and emotional health showed moderate correlations with the corresponding SF-12 domains (Table 3).
Confirmatory factor analysis results for the Japanese LupusPRO (n = 205)

CFI: comparative fit index; TLI: Tucker–Lewis index; RMSEA: root mean square error of approximation.
Discussion
We established the reliability and validity of the Japanese LupusPRO in a sample of 205 patients and found that age was associated with QoL. Further, the low test–retest reliability indicated fluctuations in non-physical-related QoL during a two-week interval.
As expected, the older group perceived their physical health to be worse compared with the younger group. Similarly, the mental aspects of QoL, as measured by both the generic and disease-specific QoL scales, were worse for the older group than for the younger group. Our findings support those of previous studies. An Italian study by Rinaldi et al. compared QoL in 126 SLE patients and healthy controls (age range: 25–64 years). 34 They found that in SLE patients, mean SF-36 physical health and mental health scores linearly decreased with increasing age, whereas scores for the healthy controls did not decrease with increasing age. A study of health-related QoL in patients with rheumatic disorders showed that older patients had worse QoL scores related to physical and social relationships than younger patients. 35 Our results showed that the older group had higher LupusPRO coping scores than the younger group, but the former had worse health-related QoL than the latter. Further research is needed to explore the effect of age on QoL to identify areas for intervention.
The test–retest reliability scores showed fluctuations in the LupusPRO emotional health and social support domains. In contrast, the physical aspects of LupusPRO were relatively stable. A similar pattern was found for SF-12 QoL scores. Of those LupusPRO test-retest validation studies using intervals of two to three days, three studies showed relatively high agreement for most of the domains,14–17 whereas the original LupusPRO validation study found low correlations (<0.7) for satisfaction with care, procreation, desires/goals and social support. 11 Differences in data collection methods and demographic characteristics may account for these inconsistent findings. Our participants completed the first questionnaire after finishing their physician consultation and completed the second questionnaire at home. They may have had more time to reflect on social support and emotional health issues. Previous studies lack descriptions of how these data were collected.14–17 Regarding demographic differences, our sample had a greater range of both age and SLE duration compared with participants in previous LupusPRO validation studies.11,14–17
Regarding the internal consistency of the LupusPRO, Cronbach’s alpha for lupus symptoms, lupus medications, social support and coping domains was less than optimal. 29 Cronbach’s alpha increases with the number of items in a domain, 36 and these domains comprise only a few items. Overall, the test-retest reliability of the Japanese LupusPRO was satisfactory and was in agreement with previous studies.11,14–17
We also established the content validity, convergent validity and construct validity of the Japanese LupusPRO. The content validity index was high and the face validity of the scale was established. Moderate correlations between the Japanese LupusPRO domains and the corresponding SF-12 domains demonstrated convergent validity. The weak correlation between the Japanese LupusPRO scores and the SLEDAI symptom scores (alopecia and rash) indicate that disease activity is not a good predicator of QoL in SLE patients, which is in accordance with previous studies.37,38 The confirmatory factor analysis results confirmed the construct validity of the LupusPRO.
One study limitation was that data were drawn from only some areas of western Japan. Another limitation is that only the SLEDAI was used to evaluate disease activity or organ damage. However, previous studies also found small correlations between these clinical indicators and the LupusPRO.11,14–17
A major finding of this study was that participants perceived that they had a low level of social support. Compared with provision for rheumatoid arthritis patient groups, there are few SLE self-help groups in Japan and online resources are limited. The formation of support groups and the improvement of online resources are urgently needed.
Fluctuations in mental and emotional aspects of QoL are of concern for health care professionals as well as for patients. We found that domain scores for social function, cognition and coping fluctuated more than scores for physical domains in the two-week interval. A similar pattern was found for SF-12 scores. Perceived lack of social support may indicate SLE participants’ vulnerability to stress, which would affect QoL related to social function, cognition and coping. Qualitative research is necessary to explore Japanese SLE patients’ perceptions of social support and other related QoL domains.
Conclusion
These findings demonstrate the reliability and validity of the Japanese version of the LupusPRO. We found that older participants had generally lower median QoL domain scores than younger participants. However, older participants seemed to cope better with SLE than younger participants. We also found that the social and mental aspects of QoL, as measured by the Lupus PRO and the SF-12, tended to fluctuate more than the physical aspects during a two-week interval. Health care professionals need to be attentive to the vulnerability of SLE patients. Future research is necessary to examine which factors predict QoL in SLE patients.
Footnotes
Acknowledgments
We would like to thank all patients who participated in this study and the staff at the three clinics that cooperated with the data collection. We would also like to acknowledge Dr. Atsushi Kumanogoh, Dr. Yasushi Tanaka, Dr. Chihiro Tanaka, and Dr. Noriaki Yoh for supporting this project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author (MI) received a research assistant scholarship for this project from Osaka University.