
Abstract
Neuropsychiatric events in systemic lupus erythematosus patients may present a diagnostic and therapeutic challenge. Common and heterogeneous, their characterization and attribution to systemic lupus erythematosus and non-systemic lupus erythematosus is important and derived from clinical assessment, selection and interpretation of investigations. A standardized approach to assigning attribution has been used in recent studies. The current therapies are largely empiric, based upon known disease mechanisms and treatment of other serious organ disease in systemic lupus erythematosus. Further insight on the immunopathogenetic mechanisms and clinical outcome of neuropsychiatric systemic lupus erythematosus is required to inform the design and execution of therapeutic clinical trials.
Introduction
Nervous system disease has been recognized in all cohorts of patients with systemic lupus erythematosus (SLE) regardless of patient demographic characteristics, recruitment from community or academic medical centers, or geographic location. Neuropsychiatric (NP) symptoms are one of the most frequent concerns of lupus patients and a challenge for the diagnosing and treating physician. The specific complaints vary from common entities such as headache, mood disorders and cognitive complaints to less frequent NP events such as seizures and psychosis. For most of these NP events their lack of specificity for SLE makes attribution difficult despite advances in neuroimaging and other diagnostic tools. The complexity of the nervous system and the relative lack of accessibility to tissue have slowed the discovery of pathogenetic mechanisms in contrast to other organ involvement such as skin and kidney. Despite these challenges, considerable progress has been made over the past decade in elucidating a clearer understanding of the clinical manifestations, immunopathogenic mechanisms and treatment options for nervous system disease in SLE. Central to all of these advances is the issue of attribution of NP events and the avoidance of diagnostic pitfalls in individual SLE patients.
Classification of NP events
Neuropsychiatric syndromes in systemic lupus erythematosus as defined using the American College of Rheumatology nomenclature
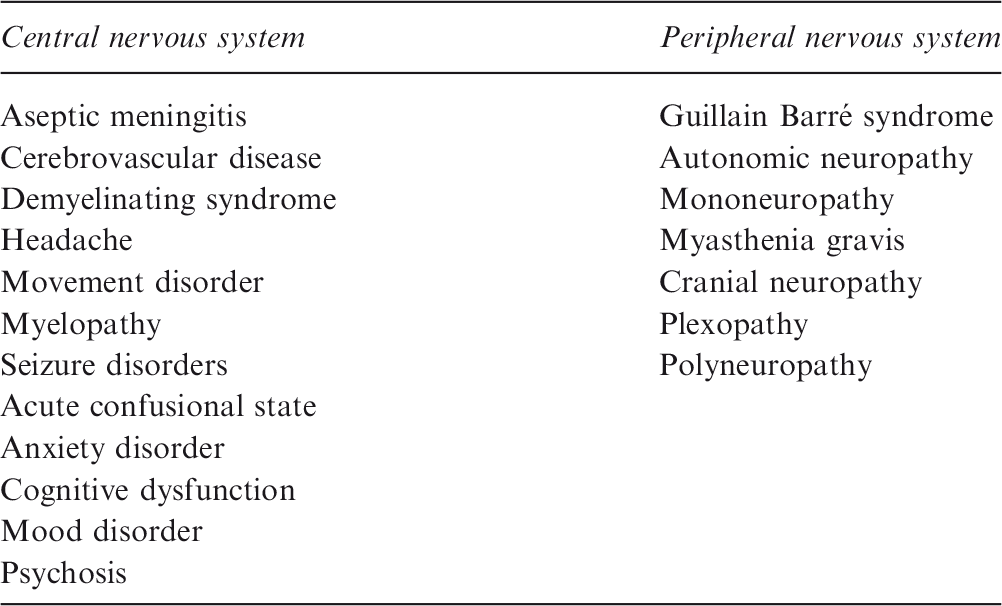
From The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum 1999; 42: 599–608 with permission. 2
Attribution of NP events in SLE
Attribution of neuropsychiatric events in systemic lupus erythematosus

SLE: systemic lupus erythematosus; NP: neuropsychiatric; ACR: American College of Rheumatology.
Attribution Model A (most stringent): NP events which had their onset within six months of diagnosis of SLE and had no “exclusions” or “associations” and were not one of the NP events identified by Ainiala et al.5,a were attributed to SLE.
Attribution Model B (least stringent): NP events which had their onset within 10 years of the diagnosis of SLE and had no “exclusions” and were not one of the NP events identified by Ainiala et al.5,a were attributed to SLE.
Ainiala NP events: all headaches, anxiety, mild depression, mild cognitive impairment and polyneuropathy lacking electrophysiologic confirmation. Arthritis Rheum 2001; 45: 419. 5
Over a range of studies in the SLICC cohort these attribution rules have provided consistent results in the proportion of NP events attributed to SLE and non-SLE causes. Depending upon the stringency of the attribution rule, the proportion of NP events attributed to SLE in newly diagnosed SLE patients varied from 19% to 38% of NP events in 6% to 12% of patients over the first year of the illness. Although headache and mood disorders were the most frequent NP complaints, seizure disorders, cerebrovascular disease, acute confusional states and neuropathies were the most common NP syndromes attributed to SLE. The cumulative occurrence of NP events increased over time, although the proportion of events attributed to SLE and non-SLE causes remained the same.6,7 Studies using these attribution rules have shown differences in clinical outcomes for NP events attributed to SLE and non-SLE causes, 4 stronger associations with some lupus autoantibodies8,9 and stronger associations between patient and physician reported outcomes for NP events attributed to SLE. 4
In a subsequent study by Bortoluzzi et al. 10 four themes were considered in constructing an attribution model, the first three of which were similar to those used in the SLICC inception cohort: (i) temporal relationship of NP events to the diagnosis of SLE; (ii) recognition of confounding factors (i.e. alternative causes or non-SLE contributing factors derived from the ACR case definitions for 19 NP syndromes); (iii) identification of minor or common NP events as described by Ainiala et al.; 5 (iv) favoring factors (i.e. clinical and non-clinical variables which support the attribution to SLE derived from European League against Rheumatism (EULAR) recommendations on NPSLE 11 and an expert panel). The first item applied to all NP events and for the latter three items, lists of variables specific for each NP event were required. The study included the 19 NP syndromes as per the ACR case definitions. The validation exercise used retrospective data on SLE patients from seven Italian rheumatology centers over a five-year period. Statistical modeling was used to derive a weighted attribution score for each of the NP events and validated by comparison to the attribution determined by a multidisciplinary team who graded the events as related, uncertain or unrelated to SLE. The area under the receiver operating characteristic (ROC) curve using dichotomous outcomes (related vs uncertain/not related) was 0.866 in the derivation dataset and 0.816 in the validation dataset. In the combined dataset a cut-off score of ≥6, yielded a positive predictive value (PPV) of 78.8% (95% CI 73.4–83.6%) and negative predictive value (NPV) of 76.1% (95% CI 69.1–82.2%). Adjusting the attribution score to >7 provided a PPV of 86.3% (95% CI 76.2–93.2%) and a score <3 provided a NPV of 85.7% (95% CI 63.7–97%) in the validation dataset.
NP events and health-related quality of life (HRQoL) in SLE
Regardless of attribution of NP events to SLE or non-SLE causes, most
4
although not all,
12
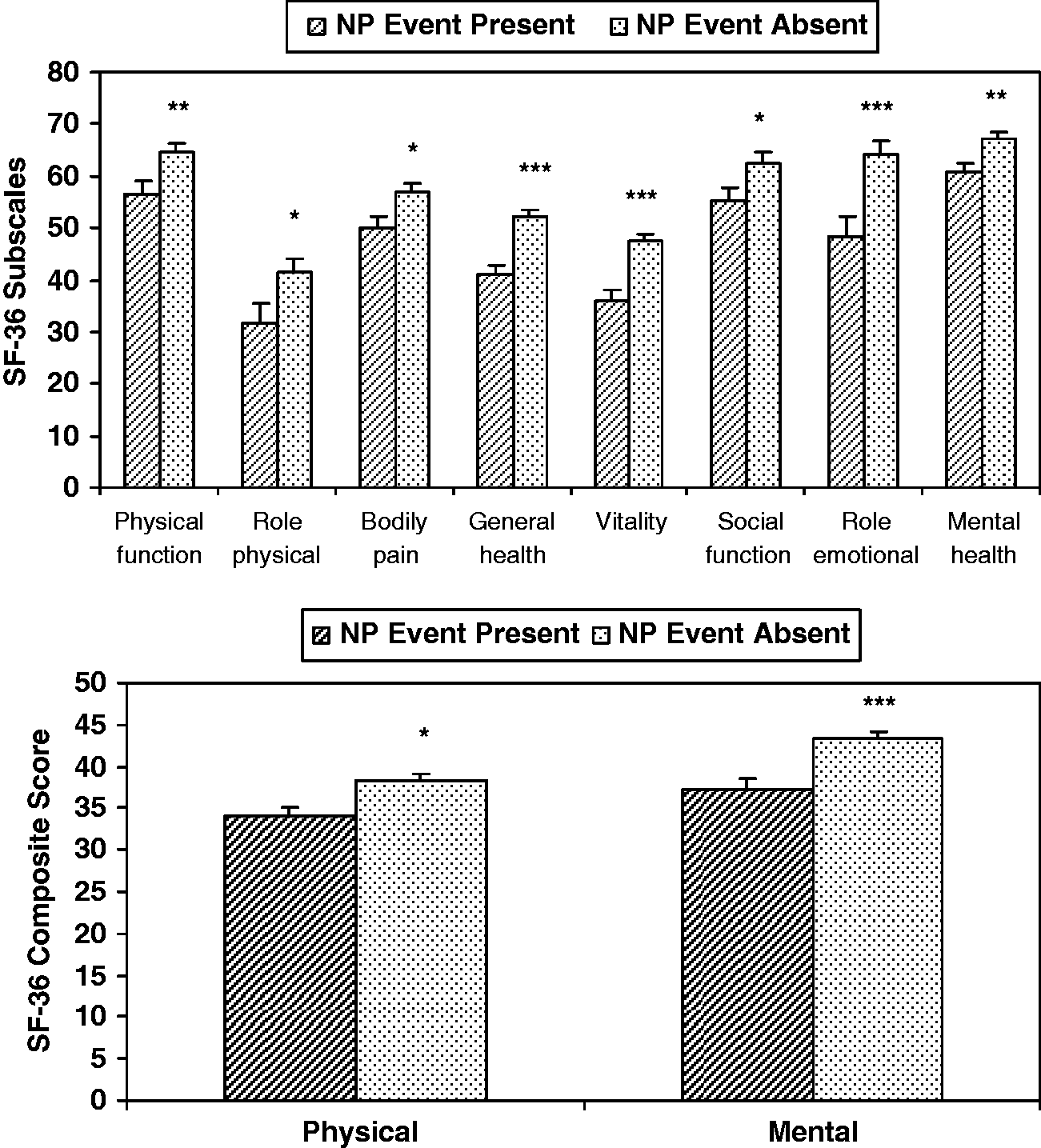
events are associated with a significant negative impact on health-related quality of life (HRQoL) (Figure 1). This is true even when other factors that impact HRQoL, such as global SLE disease activity, cumulative organ damage and medications, are taken into account. Clinically meaningful changes in HRQoL concur with physician determination of improvement or deterioration in NP events over time, indicating that HRQoL is a valid global patient outcome in clinical studies of NPSLE.
13
The correct attribution has implications for the study of pathogenic mechanisms, selection of investigative and treatment strategies.
Negative impact of NP events on HRQoL in patients with SLE. The difference in HRQoL of patients newly diagnosed with SLE with and without NP events is indicated by SF-36 subscale scores (upper panel) and physical and mental composite scores (lower panel), expressed as means ± SEM. Those patients with NP events, regardless of attribution to SLE or non-SLE causes, had consistently lower scores, indicating poorer HRQoL. Abbreviations: *p < 0.05; **p < 0.01; ***p < 0.001; HRQoL: health-related quality of life; NP: neuropsychiatric; SF-36: short form 36; SLE: systemic lupus erythematosus. Permission obtained from John Wiley & Sons, Inc. © Hanly JG, et al. Arthritis Rheum 2007; 56: 265–273.
3
Etiology and pathogenesis of NPSLE
A rational approach to the investigation and treatment of NP events attributed to SLE is based upon an understanding of underlying immunopathogenic mechanisms which consist of vascular abnormalities, autoantibodies and inflammatory mediators
14
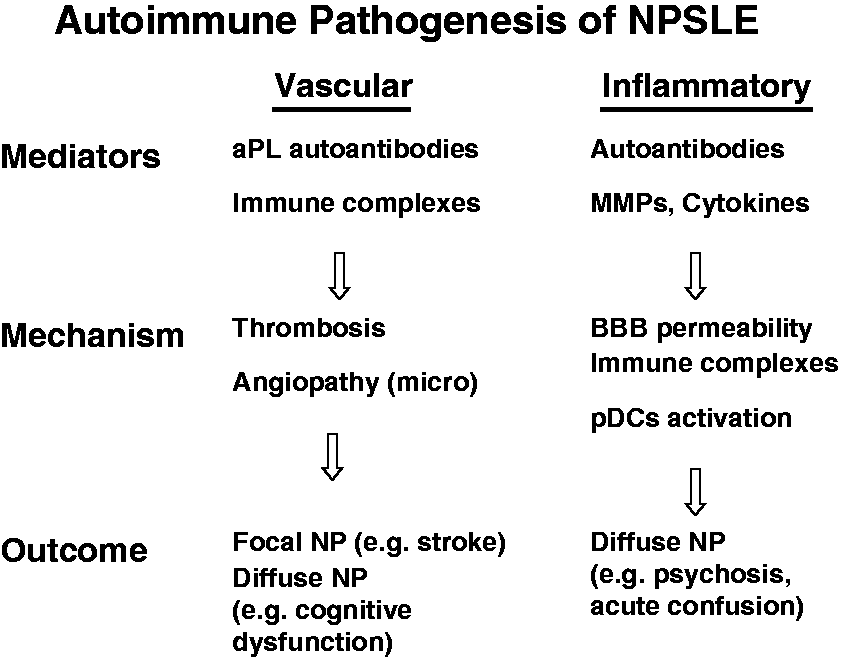
(Figure 2). The combined data from animal and human studies suggest two separate and potentially complementary autoimmune pathogenic mechanisms for NPSLE
14
(Figure 3): (i) vascular injury involving large and small caliber vessels mediated by antiphospholipid antibodies, immune complexes and leukoagglutination. Clinical sequelae include focal NP events such as stroke and diffuse NP events such as cognitive dysfunction; (ii) autoimmune inflammation mediated injury with increased permeability of the blood–brain-barrier, intrathecal formation of immune complexes, production of IFN-α and other inflammatory mediators. Clinical sequelae include diffuse NP manifestations such as psychosis and acute confusion.
Factors contributing to neuropsychiatric (NP) events in systemic lupus erythematosus (SLE) patients. Focal and diffuse nervous system events may result from direct autoimmune/inflammatory mechanisms related to SLE (Primary NPSLE), or a consequence of complications of the disease (e.g. hypertension), or its therapy (e.g. infection) (Secondary NPSLE), or a concurrent non-SLE related NP event. Adapted from Hanly JG. Neuropsychiatric lupus. Curr Rheumatol Rep 2001; 3: 205–212.
15
Autoimmune pathogenic mechanisms for NPSLE: (i) vascular injury involving both large and small caliber vessels mediated by antiphospholipid antibodies, immune complexes and leukoagglutination which results in focal NP events such as stroke and in diffuse NP events such as cognitive dysfunction; (ii) injury due to inflammation in which increased permeability of the blood–brain-barrier, formation of immune complexes, and production of IFN-α and other inflammatory mediators lead to diffuse NP manifestations such as psychosis and acute confusional states.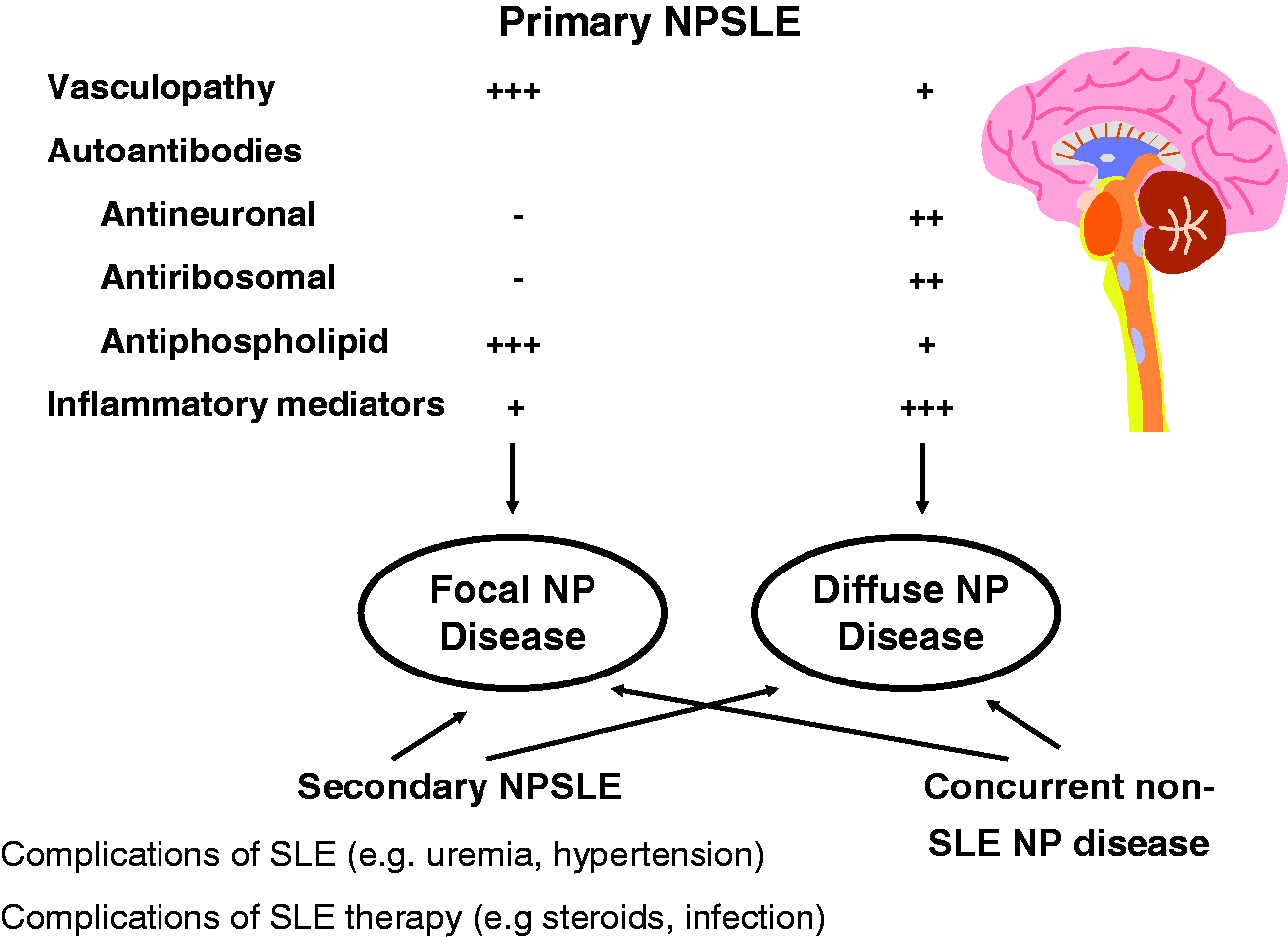
Diagnostic approach and investigation for NPSLE
The diagnostic work-up should include an approach similar to that employed in non-SLE patients presenting with the same manifestations. 11 For example, the investigation of a transient ischemic attack or stroke should include a screening echocardiogram and Doppler ultrasound of the carotids in addition to lupus specific tests such as antiphospholipid antibodies. Additional examples include a search for metabolic abnormalities, infection and use of psychoactive drugs in patients with acute confusion and work-up for diabetes mellitus and vitamin B12 deficiency in patients with peripheral sensory neuropathy.
Autoantibodies in the circulation and cerebrospinal fluid (CSF)
Circulating antiphospholipid antibodies should be measured in patients with focal NP events or cognitive decline and anti-ribosomal P antibodies in patients with psychosis. Examination of cerebrospinal fluid (CSF) is done primarily to exclude infection but provides an opportunity to measure autoantibodies. For example, studies of paired serum and CSF samples from patients with and without NPSLE events16,17 found significant associations between NP events and CSF anti-NR2 autoantibodies. The identification of proinflammatory cytokines and biomarkers of neurological damage in CSF may provide clinically useful tools in the future.
Electrophysiological studies
Electroencephalography (EEG) is required to investigate seizure disorders, 18 nerve-conduction studies to confirm sensory/sensorimotor polyneuropathies and skin biopsy is required for diagnosing small-fiber neuropathies.
Neuropsychological assessment
Self-report measures of perceived cognitive impairment are poorly correlated with objective cognitive assessment in SLE patients,19,20 show low sensitivity, 21 and are associated with concurrent anxiety and depression. Screening tools such as the Montreal Cognitive Assessment Scale (MoCA) 22 are insensitive. Ideally, formal neuropsychological testing should be done when there is a clinical suspicion of impaired cognitive ability. If abnormal, testing should be repeated after several months, to measure change in cognition following observation or treatment. Computerized testing facilitates efficient screening of SLE patients by non-experts 23 but may fail to identify higher level cognitive impairment in SLE. 23
Neuroimaging
The assessment of brain structure and function by conventional and advanced neuroimaging helps to localize intracranial abnormalities, distinguish white or grey matter disease, measure cerebral atrophy and change over time. Computed tomography (CT) scanning has largely been replaced by conventional magnetic resonance imaging (MRI). With the exception of larger cerebral infarcts, there is a poor correlation between structural changes and clinical NP manifestations, which limits structural MRI as an indicator for disease progression in SLE. 24 Magnetic resonance angiography (MRA) provides a non-invasive visualization of cerebral blood flow, although not optimal for visualization of flow in small caliber vessels which are primarily involved in NPSLE. More advanced MRI methodology for detection of structural abnormalities includes magnetization transfer imaging (MTI), diffusion weighted imaging (DWI) and diffusion tensor imaging (DTI). 25
Magnetic resonance spectroscopy (MRS) measures biochemical compounds within pre-determined brain regions of interest. For example, N-acetylaspertate, which reflects the quantity of neuronal/axonal tissue, is decreased in SLE patients, even in the absence of visible damage on structural MRI.25,26 Other neurometabolites reported in active NPSLE include increased choline and lactate indicating inflammation and compromised tissue metabolism, respectively. 27
Positron emission tomography (PET) scanning is the most objective neuroimaging study of brain function, but access and cost limit its applicability. 28 Single photon emission computed tomography (SPECT) scanning 28 provides semi-quantitative analysis of regional cerebral blood flow and metabolism. It is exquisitely sensitive and in SLE patients 29 SPECT imaging has identified both diffuse and focal deficits which may be fixed or reversible. However, the findings are not specific for SLE, 30 do not always correlate with clinical NP manifestations 31 and their clinical significance is unclear.
Blood-oxygen-level-dependent functional MRI (BOLD-fMRI) measures changes in local brain deoxyhemoglobin levels that reflect neuronal activity and thereby provide indirect measures of brain function. The results from preliminary studies 32 suggest that compensatory adaptation of neuronal function through the recruitment of additional cortical pathways supplements impaired function of standard pathways. These compensatory responses maintain cognitive function in the short-term but may eventually be overcome and manifest as overt cognitive impairment. Future studies with fMRI should provide insights into changes in functional organization of neural networks that arise in NPSLE.
Treatment principles
The correct attribution of NP events is a critical first step in the care of individual patients with NP events. The decision to use potent immune suppression is unnecessary and potentially risky for NP events attributed to non-SLE causes for which symptomatic therapies may be effective and safe. The wrong attribution of NP events (e.g. seizures, mood disorders or headache) to SLE when scoring disease activity measures (e.g. SLEDAI-2K 33 and BILAG 34 ) may result in erroneously high global disease activity scores. This is a particular problem with NP variables due to their heavy weighting within disease activity indices.
Treatment, which is tailored to specific NP manifestations and the needs of individual patients, can be considered as four major components: (i) treatment of comorbidities (e.g. infection, hypertension) contributing to the NP event; (ii) use of symptomatic therapies (e.g. anti-depressants, anti-seizure drugs); (iii) high dose corticosteroids and immunosuppressive drugs (e.g. azathioprine, cyclophosphamide, mycophenolate mofetil) for NP events attributed to autoimmune inflammatory mechanisms; (iv) full anticoagulation in patients with NP events attributed to intravascular thrombosis.
Prognosis
The literature is divided on the significance of NP disease in SLE when assessed by outcomes such as mortality35,36 and hospitalization. 37 A clinical study of SLE patients with a mean follow-up of 3.6 years 6 reported resolution in approximately 15% of NP events at each annual assessment, but the majority of events persisted to some degree. Most of the longitudinal studies of cognitive function found stable cognitive test performance over time and progressive cognitive dysfunction occurred in a minority of patients.38,39 Recent studies using a systematic approach to attribution have reported more favorable outcomes for NP events attributed to SLE.4,7,12,40
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Hanly’s work is supported by the Canadian Institutes of Health Research grant number MOP-88526.