
Abstract
We aimed to analyze compliance and persistence with hydroxychloroquine (HCQ) in real practice and identify risk factors for poor adherence in South Korean patients with systemic lupus erythematosus (SLE). This retrospective longitudinal study evaluated 235 SLE patients in whom oral HCQ was newly started from 2002 to 2016 at a tertiary hospital in South Korea. Compliance was assessed using one-year medication possession ratio (MPR) and non-compliance was defined as a one-year MPR < 0.8. Persistence was determined as the time from HCQ treatment initiation to discontinuation without interruption for ≥56 days. The mean one-year MPR of HCQ was 0.88 and the frequency of non-compliance was 19.9%. During the study period, 115 (48.9%) patients discontinued HCQ and forgetfulness and/or carelessness (73%) were the most common reason for HCQ non-persistence, followed by adverse events (10.4%), unknown factors (10.4%), and pregnancy (6.1%). Median duration until HCQ discontinuation was 55.1 months and the one-year persistence rate to HCQ was 0.8. SLE Disease Activity Index 2000 (SLEDAI-2K) < 6 was a significant risk factor for non-compliance (OR = 2.98, p = 0.001) and non-persistence (HR = 1.55, p = 0.046) with HCQ after adjusting confounding factors. However, HCQ adherence was not associated with the dose of HCQ or concomitant immunosuppressive medications. Our data showed that overall adherence to HCQ in SLE patients was suboptimal in real practice and SLEDAI-2K score < 6 was a risk factor for poor adherence, suggesting the need to improve adherence with HCQ treatment in SLE patients, especially in those with low disease activity.
Introduction
Systemic lupus erythematous (SLE) is a chronic systemic autoimmune disease characterized by a relapsing-remitting course and a highly variable prognosis. As persistent inflammation in SLE can lead to irreversible organ damage which is linked with substantial morbidity and mortality, therapeutic strategies aim at reducing overall burden of systemic inflammation. 1 In addition, patients need to be maintained on long-term treatment due to the chronicity, incurability, and unpredictability of SLE. 1 In this respect, hydroxychloroquine (HCQ) is regarded as a mainstay in the treatment of SLE because of its efficacy in preventing flares, achieving remission, reducing the risk of cumulative damage, and even reducing overall mortality.2,3 Lifelong treatment with HCQ is now recommended for all patients with SLE irrespective of disease severity and the use of other treatments unless contraindication exists.1,4,5 Thus, adherence to HCQ is crucial to control disease progression and optimize clinical outcome in patients with SLE. However, lack of medication adherence is quite common and known to be associated with unfavorable treatment outcomes including higher morbidity and increased frequency of acute care utilization,6,7 which is considered to be a serious problem in the management of SLE. 6
Adherence has been used as general term consisting of both compliance and persistence. 8 “Compliance” indicates the extent to which a patient acts in accordance with the prescribed dose and interval of medication and is quantified by the medication possession ratio (MPR), which is defined as the ratio of the number of days for which a medication has been dispensed to the total number of days in a pre-specified time period.8,9 “Persistence” indicates the length of time from initiation to discontinuation of therapy. 8 Namely, adherence reflects both the accuracy (compliance) and consistency (persistence) in following a therapeutic regimen. 10 To characterize the comprehensive medication-taking behavior of patients, both compliance and persistence should be defined and assessed separately. 8 In particular, long-term medication persistence can be interpreted as a composite measure of efficacy, safety, and tolerability in patients with chronic conditions such as rheumatic diseases.11,12 Adherence to HCQ in patients with SLE has been reported previously using various methods including validated self-reported patient questionnaires, pharmacy refill records, and blood HCQ concentration.13–16 However, most of the previous studies were based on short-term follow-up periods and did not distinguish between compliance and persistence when reporting the results of HCQ adherence. Thus, the present long-term clinical study aimed to analyze compliance and persistence with HCQ in real practice and identify risk factors for poor adherence to HCQ in South Korean patients with SLE.
Methods
Study design and population
The present study is a retrospective longitudinal analysis evaluating 235 South Korean patients with SLE aged from 12 to 74 years in whom oral HCQ was newly started for the treatment of SLE from January 2002 to April 2016 at the regional rheumatism center of a tertiary hospital in South Korea. All patients were diagnosed with SLE based on the American College of Rheumatology (ACR) revised criteria for the classification of SLE. 17 All study patients were ethnically South Korean and resided in the same country. We defined the index date as the date of the first prescription for HCQ without use in the prior six months 7 and SLE patients were followed up longitudinally from the index date to April 2017 through reviews of electronic medical records. All HCQ prescriptions were made by highly experienced rheumatologists at our center. To ensure correct identification of new HCQ users and sufficient data for assessment of compliance and persistence, only SLE patients who had electronic medical records for at least six months before and 12 months after their index date were eligible for this study.9,18 SLE patients with other rheumatic or autoimmune diseases, including rheumatoid arthritis, spondyloarthritis, juvenile idiopathic arthritis, systemic sclerosis, polymyositis, dermatomyositis, and mixed connective tissue disease, were excluded; however, SLE patients with secondary Sjogren’s syndrome were included. The Research and Ethical Review Board of the Pusan National University Hospital approved this study and waived the need for informed consent because of the study’s retrospective design (IRB no. 1705-005-055).
Assessment of compliance and persistence with HCQ
Compliance with HCQ was estimated using the one-year MPR which was calculated as the sum of available HCQ supply days during the one-year study period divided by 365 potential days of HCQ treatment.9,19 SLE patients with a one-year MPR ≥ 0.8 were considered to be compliant with HCQ whereas non-compliance was defined as a one-year MPR < 0.8 as previously described.9,20–22 For example, if an SLE patient had been prescribed a daily dose of 200 mg HCQ for 365 days and had taken it for 280 days, the MPR of this patient would be 0.77 (280 ÷ 365 = 0.77) and would be considered non-compliant. An MPR < 0.8 was adopted as the definition of non-compliance due to its wide use in numerous previous studies9,20–22 Persistence was defined as the number of days from the date of HCQ initiation (index date) to the end of the last prescription issued or the end of the study period (30 April 2017) without a medication refill gap (permissible gap) of 56 days or more.8,9,23 Patients with SLE were considered to be persistent with HCQ if HCQ was restarted or the dose of HCQ was changed within the permissible gap, whereas a duration of HCQ discontinuation longer than the permissible gap was considered to be non-persistent, even if HCQ was subsequently reinitiated.9,20 During the study period, SLE patients had been uniformly informed about the importance of HCQ through the same booklet and advised to take HCQ with food to avoid gastrointestinal complaints in our center. Causes of non-persistence with HCQ were categorized as follows based on reviewing the patients’ medical records: (a) forgetfulness and/or carelessness, (b) adverse events, (c) pregnancy, and (d) unknown factors. HCQ discontinuation due to patients’ concern for HCQ use during pregnancy was cclassified as “pregnancy.” “Adverse events” were further subcategorized into allergic reactions, HCQ retinopathy, thrombocytopenia aggravation, lymphoma, gastrointestinal complaints, renal impairment, cardiomyopathy, and optic neuropathy.
Clinical data
The following demographic, clinical, and laboratory data were collected by reviewing the SLE patients’ medical charts: age at HCQ initiation, HCQ dose, sex, disease duration, baseline disease activity (SLE Disease Activity Index 2000; SLEDAI-2K), 24 clinical manifestations, immunological findings, and concomitant medications records. Disease duration was calculated from the date at SLE diagnosis to the index date and presented as months, and the baseline SLEDAI-2K in each SLE patient was measured at presentation. The presence of SLE manifestations during the study period, including malar rash, discoid rash, photosensitivity, oral ulcer, arthritis, serositis, biopsy-proven lupus nephritis, psychosis, leukopenia, lymphopenia, and thrombocytopenia, were recorded and defined as ACR revised criteria for the classification of SLE. 17 Anemia was defined as Hb < 12.5 in females or <14.0 in males. Immunological data such as anti-nuclear antibody (ANA), IgG anti-dsDNA antibody, C3, C4, anti-Sm antibody, lupus anticoagulant, and IgG and IgM anticardiolipin antibodies were also obtained. ANA was assessed using indirect immunofluorescence on HEp-2 cells and anti-dsDNA, anti-Sm, and anticardiolipin antibodies were determined by enzyme-linked immunosorbent assay. Concomitant medications included oral glucocorticoids (GCs), methotrexate (MTX), azathioprine (AZA), mycophenolate mofetil (MMF), tacrolimus (TAC) and cyclophosphamide (CYC). Regarding CYC, only intravenous agents had been available during the study period in our center.
Statistical analyses
For continuous variables, the Kolmogorov–Smirnov test was used to check for the normality of data distribution. Continuous variables were presented as mean ± standard deviation (SD) or median (interquartile range [IQR]) as appropriate, whereas categorical variables were summarized as the number of cases with percentages. To test for differences in clinical characteristics between SLE patients compliant and non-compliant with HCQ, Student’s t-test or the Mann–Whitney U test were applied for continuous variables and the chi-square test or Fisher’s exact test were used for categorical variables. Persistence with HCQ was analyzed and presented as a Kaplan–Meier survival analysis and the log-rank test was employed to examine differences between the survival curves. Multivariable logistic and Cox regression models with backward selections including covariates with p < 0.1 in univariable analyses were performed to identify risk factors for non-compliance and non-persistence. Age and sex were included as a priori confounders in multivariable models. A two-sided p < 0.05 was considered statistically significant. Data storage and analyses were carried out using PASW 19.0 for windows (Chicago, IL, USA) and STATA 11.0 for Windows (StataCorp LP, College Station, TX, USA).
Results
Clinical characteristics of patients with systemic lupus erythematosus receiving hydroxychloroquine
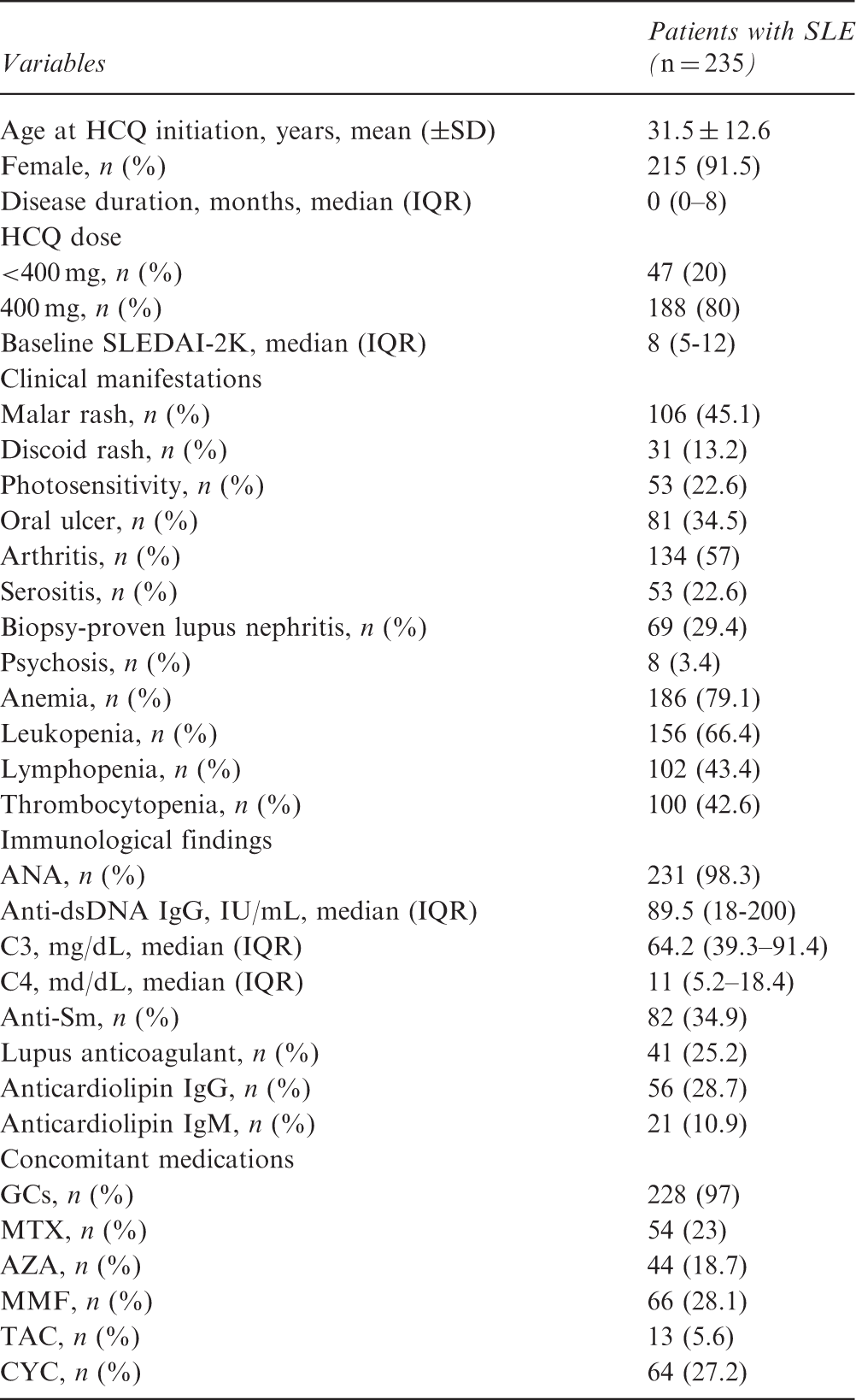
ANA: anti-nuclear antibody; AZA: azathioprine; CYC: cyclophosphamide; GCs: glucocorticoids; HCQ: hydroxychloroquine; MMF: mycophenolate mofetil; MTX: methotrexate; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000; TAC: tacrolimus.
Logistic regression models for a non-compliance to hydroxychloroquine in patients with systemic lupus erythematosus
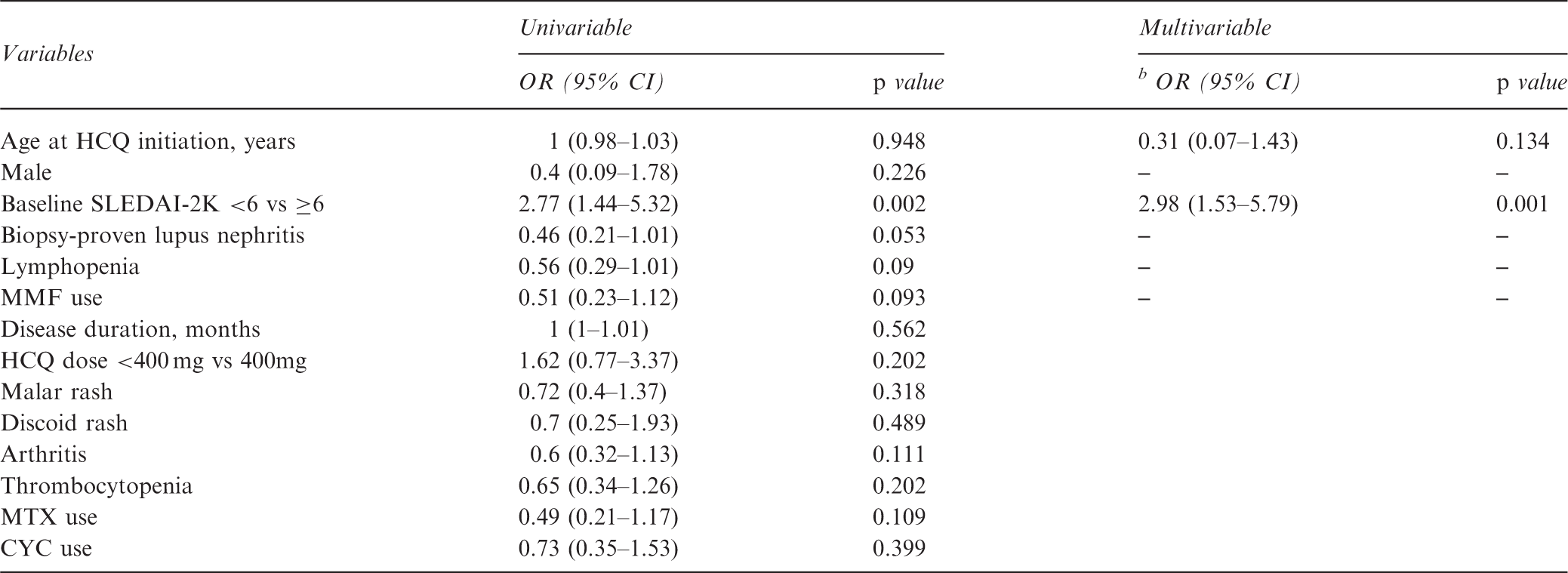
CYC: cyclophosphamide; HCQ: hydroxychloroquine; MMF: mycophenolate mofetil; MTX: methotrexate; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000.
Non-compliance was defined if the one-year medication possession ratio was less than 0.8.
Estimated using multivariable backward logistic regression models including age, male, baseline SLEDAI-2K < 6 vs ≥6, biopsy-proven lupus nephritis, lymphopenia and MMF use.
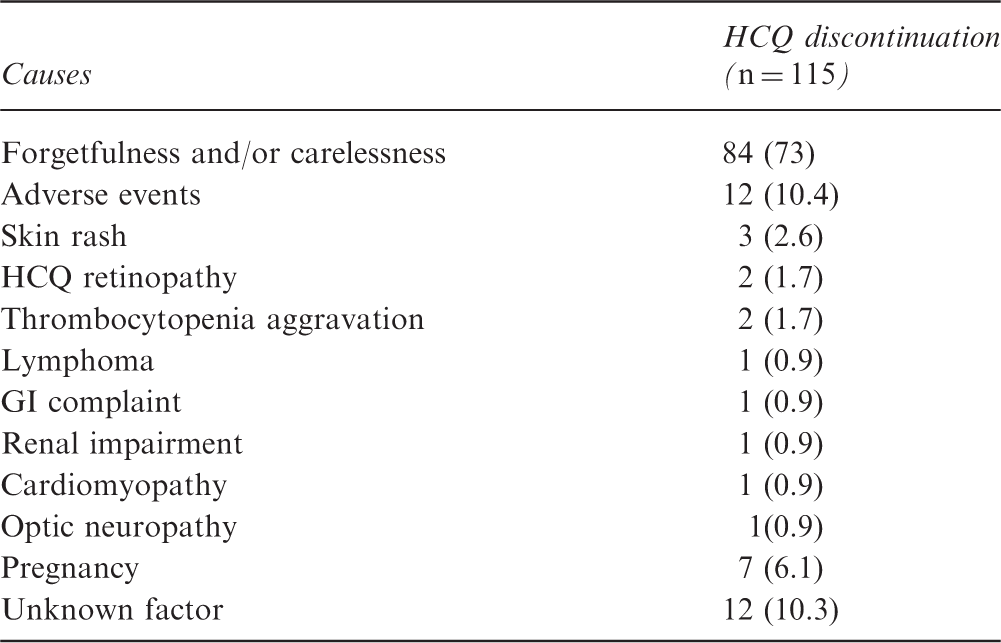
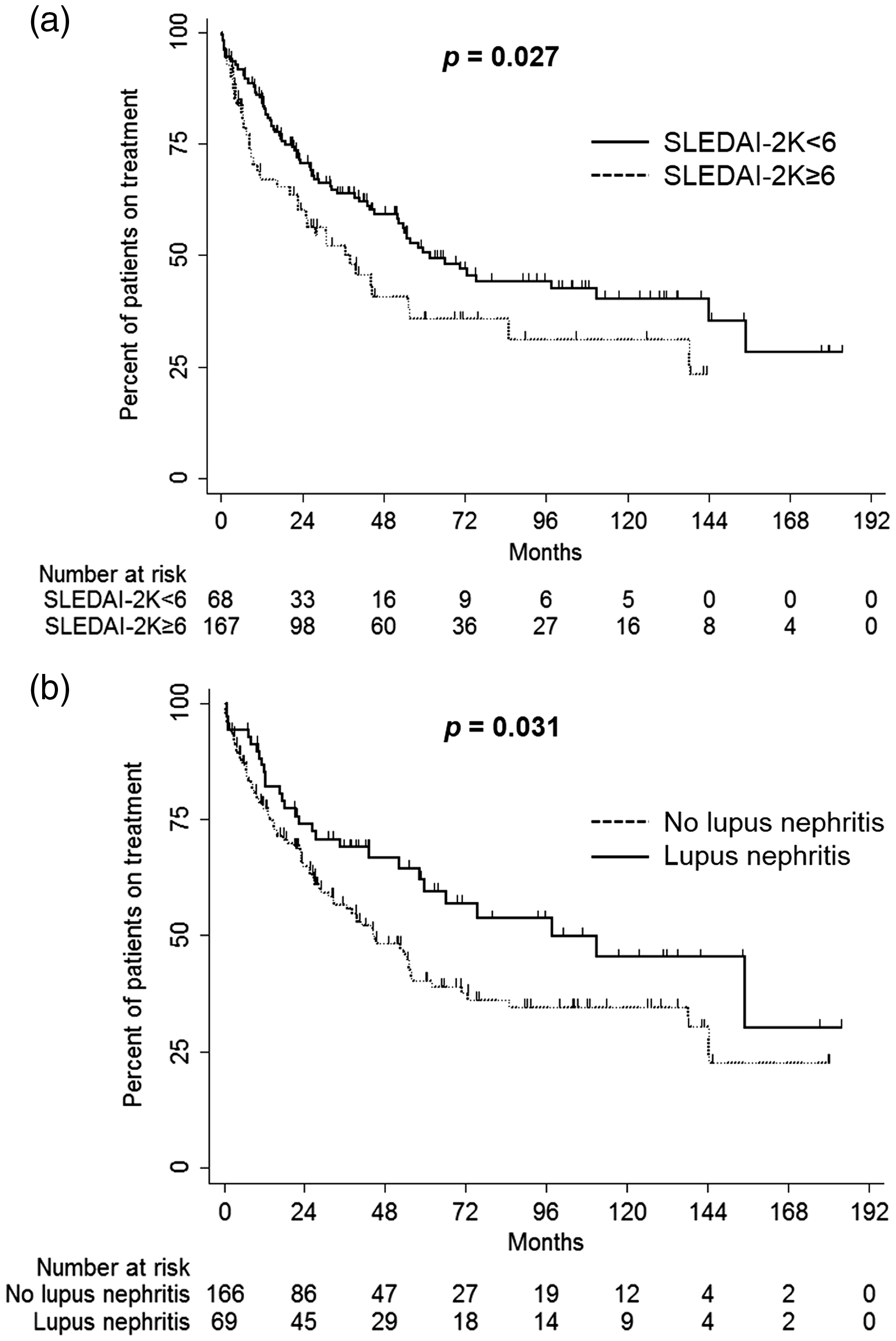
Persistence with HCQ in patients with SLE is illustrated in Figure 1. During the study period, 115 (48.9%) patients discontinued HCQ and the one-, two-, three-, four-, and five-year persistence rates were 0.8 (95% CI = 0.74–0.85), 0.67 (95% CI = 0.61–0.73), 0.61 (95% CI = 0.54–0.67), 0.54 (95% CI = 0.47–0.61), and 0.46 (95% CI = 0.39–0.54), respectively. The most incidences of HCQ discontinuation occurred within the first year after initiation and the median duration until discontinuation was 55.1 (95% CI = 40.3–69.9) months. Causes of HCQ discontinuation in SLE patients are summarized in Table 3. Forgetfulness and/or carelessness (73%) were the most common reasons for HCQ non-persistence, followed by adverse events (10.4%), unknown factors (10.4%), and pregnancy (6.1%). Among adverse events, two (1.7%) patients stopped HCQ due to HCQ retinopathy which was diagnosed by ophthalmologists at our center. SLE patients with a SLEDAI-2K score <6 showed significantly worse persistence with HCQ than those with SLEDAI-2K score ≥6, while patients with biopsy-proven lupus nephritis had better HCQ persistence than those without (Figure 2).
Persistence with hydroxychloroquine in patients with systemic lupus erythematosus evaluating by the Kaplan-Meier survival curve. Causes of hydroxychloroquine discontinuation in patients with systemic lupus erythematosus GI: gastrointestinal; HCQ: hydroxychloroquine. Persistence with hydroxychloroquine in patients with systemic lupus erythematosus according to SLEDAI-2K score (A) and the presence of biopsy-proven lupus nephritis (B).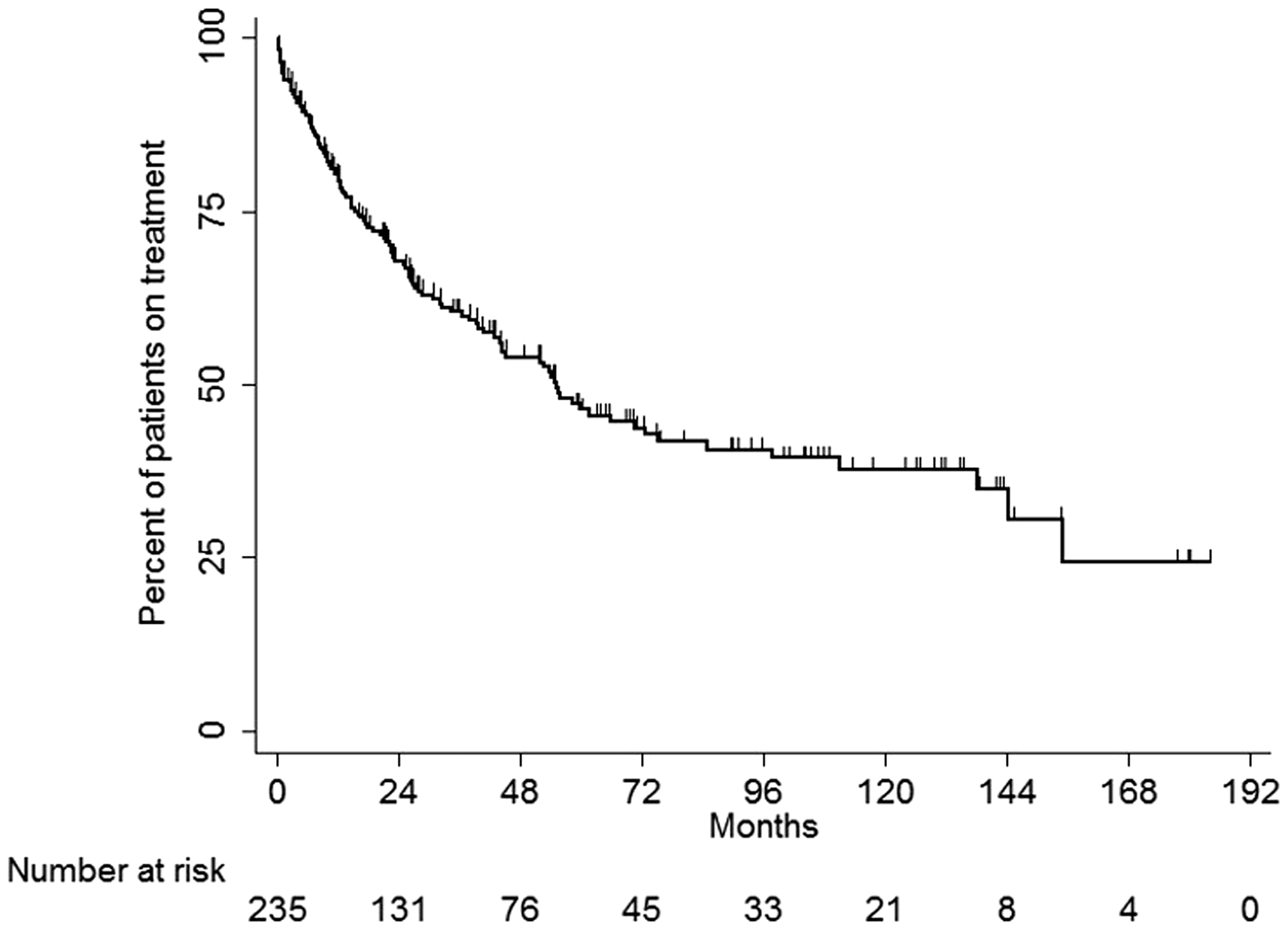
Cox regression analyses for non-persistence to hydroxychloroquine in patients with systemic lupus erythematosus
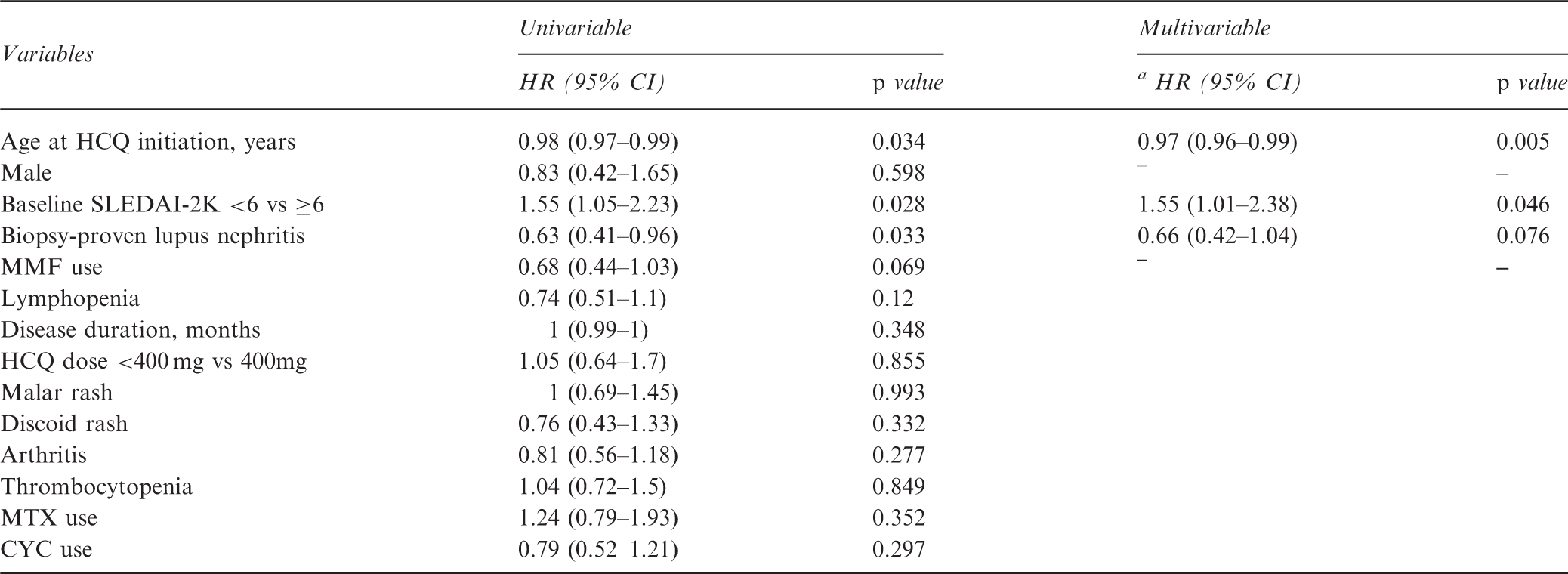
CYC: cyclophosphamide; HCQ: hydroxychloroquine; MMF: mycophenolate mofetil; MTX: methotrexate; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000.
Estimated using multivariable backward Cox regression models including age, male, baseline SLEDAI-2K <6 vs ≥6, biopsy-proven lupus nephritis and MMF use.
Discussion
The present study analyzed the compliance and persistence with HCQ in South Korean patients with SLE in a real clinical setting from pharmacy refill records. Although lifelong HCQ treatment is emphasized for optimal long-term clinical outcome, the rate of non-compliance was 19.9% and half of SLE patients in our study had discontinued HCQ at 55.1 months after the initiation of treatment. This finding suggests that adherence to HCQ in SLE patients was inadequate in real practice. The most common causes of HCQ discontinuation were forgetfulness and/or carelessness, suggesting the importance of appropriate patient education to improve HCQ adherence. Low disease activity measured by SLEDAI-2K score <6 was found to be a significant risk factor for both poor compliance and persistence with HCQ in patients with SLE. An association between older age and better persistence was also observed, but HCQ adherence was not associated with the dose of HCQ or concomitant immunosuppressive medications in our study.
Treatment adherence has been considered to be a crucial component in the management of chronic rheumatic diseases and the non-adherence rate in SLE patients varies from 3% to 76% according to the methods for measuring adherence and the medication used.6,25,26 Drug adherence can be measured by indirect methods including self-reported questionnaire, physician rating, pill counts, and pharmacy records, or direct methods such as blood drug concentration,6,25 although there is no gold standard. Self-reporting and physician assessments were widely utilized in previous studies, but these methods are subjective and can overestimate adherence. 6 Measuring blood or urine drug levels may be an objective and attractive approach and undetectable HCQ serum concentrations are reported to reflect long-term non-adherence due to its long elimination half-life (40 days). However, routine use of drug level monitoring is limited by unavailability, cost-effectiveness, and inability to estimate overall adherence. 6 Blood HCQ concentrations in particular are highly variable among patients and can be affected by various factors including dosage, renal function, disease activity, and the use of immunosuppressive agents.16,27 Thus, it is impossible to differentiate between poor adherence and other pharmacokinetic factors using drug level measurements alone. On the other hand, analysis of pharmacy refill records is a straightforward method for the calculation and interpretation of treatment adherence. 25 It can enable measurement of both compliance and persistence, thus providing more comprehensive information regarding adherence in the real setting. 8 To our knowledge, this is the first study to separately report compliance and persistence with HCQ in patients with SLE using long-term pharmacy refill data.
The present study revealed that the non-compliance rate with HCQ defined as the one-year MPR < 0.8 was 19.9%. In our literature review, four previous papers investigating adherence with HCQ in SLE patients based on pharmacy information were identified.7,13,14,28 The non-adherence rate ranged from 51% to 79% in these studies, which seemed to be higher than ours. This discrepancy may be due to the differences in the characteristics of study populations (for example, adult-onset versus childhood-onset SLE), the source of pharmacy data (for example, medical chart versus insurance claim data), and the methodology of measuring MPR (for example, one-year versus last four visit MPR).7,13,14,28 In addition, the five-year persistence rate with HCQ was less than 50% in our study. Persistence is equally important to compliance in terms of adherence, 29 however, little attention has been given to long-term persistence with HCQ in previous studies reporting treatment adherence in SLE patients. Given the importance of lifelong HCQ therapy, our data indicate a suboptimal persistence in real clinical practice, suggesting a need for intervention to improve long-term adherence to HCQ in SLE patients.
Several factors related to HCQ adherence in patients with SLE were identified in the present study. First, baseline low disease activity (SLEDAI-2K score < 6) was a significant risk factor for both compliance and persistence with HCQ. Considering that poor treatment adherence may lead to deleterious clinical outcomes, the inverse relationship between disease activity and medication adherence in our study is unexpected. Like our finding, Feldman et al. reported that SLE patients with more comorbidities were likely to have better adherence to HCQ and immunosuppressive agents. 7 Although the exact explanation remains unclear, we may assume that SLE patients with more active or severe disease may have greater awareness of their health status and thus may be more motivated to maintain HCQ adherence over time, while asymptomatic or mildly symptomatic patients may not believe that HCQ is necessary or effective. This notion was also supported by previous studies investigating treatment adherence in patients with other chronic diseases such as inflammatory bowel disease, 30 HIV infection 31 and osteoporosis. 9 Thus, our data suggest that efforts to improve treatment adherence need to be targeted particularly at SLE patients with low disease activity. Second, a significant relationship between younger age and poor persistence with HCQ was observed in this study. A similar effect of younger age on non-adherence in SLE patients was shown in a previous study, 32 but non-significant relationships were also reported,28,33 which warrants further investigation. Third, in line with a previous report, 28 our data found that concomitant immunosuppressive agents were not associated with HCQ adherence, suggesting a considerable gap in adherence among medications used in SLE treatment. This finding may be explained by differences in patients’ expectations of treatment and concerns about adverse effects and costs between HCQ and other immunosuppressive agents.
Understanding the reasons for poor adherence in patients with chronic diseases could provide insight into developing strategies to overcome the barriers to adherence. In this study, forgetfulness and/or carelessness were the major cause of HCQ discontinuation in SLE patients, which is consistent with other chronic diseases requiring long-term treatment.34–36 Patient-reminder systems such as phone calls or reminder cards may be helpful to address this issue, but a recent study showed that cellular text messages did not improve treatment adherence in SLE patients. 14 Thus, the interaction between forgetfulness and treatment adherence in SLE patients is unclear, which warrants further studies. Of note, seven patients with SLE in our study stopped HCQ treatment due to safety concerns during pregnancy. Continuation of HCQ during pregnancy in SLE patients is recommended by most experts including the European League Against Rheumatism due to its efficacy in preventing lupus flares and obstetric complications.37–39 However, similar to our result, another study also found that a considerable portion of patients did not maintain HCQ therapy during pregnancy because of a fear of adverse events linked with HCQ such as congenital anomalies, 40 suggesting the importance of patient education for better disease control. In addition, two SLE patients in our study discontinued HCQ due to HCQ retinopathy. Recently, growing attention is being paid to HCQ retinopathy, as HCQ has been widely used for the treatment of SLE. HCQ retinopathy is irreversible and there is still no effective treatment, thus early recognition by regular screening and patient education are important for prevention. 41 Since daily dose and duration of therapy are the major risk factors for HCQ retinopathy, a maximum dose of HCQ ≤ 5.0 mg/kg was recommended by the American Academy of Ophthalmology. 41
Some important limitations need to be discussed. First, the pharmacy refill data used in the present study may overestimate overall adherence because they cannot ensure that the medications are actually taken by SLE patients. In addition, pharmacy data do not fully provide information regarding the reasons for non-adherence and we could not determine the causes for 12 cases of HCQ discontinuation (Table 3). However, studying medication adherence using pharmacy refill data has been validated by other approaches, such as patient reports, pill counts, and questionnaires,13,42 and numerous studies have investigated treatment adherence in patients with rheumatic diseases using pharmacy data. 25 Second, our study only included patient with SLE at a tertiary hospital, which may lead to selection bias. Third, socioeconomic, educational, and psychosocial statuses, all of which can affect medication adherence, were not fully adjusted in this study due to its retrospective design.
In conclusion, the present study showed that compliance and persistence with HCQ in South Korean patients with SLE were suboptimal in clinical practice, potentially hampering therapeutic efficacy and worsening clinical outcome. As the major causes of HCQ withdrawal in our study were forgetfulness and/or carelessness, clinicians need to emphasize to patients the importance of regular use of HCQ in the management of SLE. Of note, a baseline low disease activity in patients with SLE was significantly linked with poor compliance and persistence with HCQ, suggesting the need for strategies to improve adherence with HCQ treatment, especially in SLE patients with low disease activity. This study can provide an insight into the overall pattern of adherence to HCQ in patients with SLE, but further studies are needed to shed more light on our results.
Footnotes
Acknowledgments
We specially thank the late Professor Sung-Il Kim who devoted himself to education, research, and patient care in the Division of Rheumatology, Department of Internal Medicine, Pusan National University School of Medicine (1963 to 2011).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by clinical research grant from Pusan National University Hospital 2017.