
Abstract
Objectives
The objectives of this paper are to look at the prevalence of neuropsychiatric manifestations and assess their impact on quality of life in North Indian lupus patients.
Methods
The study included consecutive patients with systemic lupus erythematosus (SLE) who were older than 18 years and met the SLICC 2012 criteria. A diagnosis of a neuropsychiatric syndrome was made as per ACR 1999 definitions. Manifestations occurring at any point in time after the diagnosis of SLE were considered if a reliable history and medical records were available. Quality of life was assessed by EuroQol-5D questionnaire. Means were compared by student t test for normally distributed data. Comparison of quality of life between groups was performed by the Kruskal–Wallis test and Mann–Whitney U test.
Results
This study included 101 patients of SLE with mean (±SD) age of 32.3 ± 10.0 years and a majority (n = 92) were females. Mean (±SD) age of diagnosis of SLE was 27.8 ± 9.2 years and disease duration (after diagnosis) was 4.6 ± 4.5 years. Thirty-three patients had neuropsychiatric manifestations with a total of 42 events. The most common manifestation was headache (10%) followed by anxiety disorder (5%) and peripheral neuropathy (9%). Other NPSLE syndromes observed in the study are seizure (4%), cognitive dysfunction (4%), depression (4%), acute confusional state (2%), autonomic neuropathy (2%), movement disorder (1%), and mononeuritis multiplex (1%). On comparing the groups of NPSLE, nephritis, and neither, there was a significant difference in mobility, self-care, pain, and worry. On post hoc test, there was a significant difference between the NPSLE and neither group.
Conclusion
Neuropsychiatric manifestations significantly affect quality of life in North Indian SLE patients.
Introduction
Systemic lupus erythematosus (SLE) is a chronic inflammatory disorder characterized by tissue damage that is mediated by autoantibodies and immune complexes. 1 Though neuropsychiatric manifestations of SLE were recognized by Kaposi more than a century ago, diagnosis and management of these continue to pose difficult challenges even today. 2 With increasing awareness and better diagnostic modalities, neuropsychiatric manifestations are being recognized more frequently in SLE patients and account for a considerable proportion of morbidity and mortality associated with this disease. These include cognitive disorders, mood disorders, headache, seizures, nerve or muscle involvement, stroke, transient ischemic attacks, movement disorders, psychosis, aseptic meningitis, and myelopathy. 3
Nervous system involvement remains one of the least understood aspects of SLE. The frequency of involvement has ranged from 20% to 95% in different studies. 4 This heterogeneity is due in part to differences in methodology adopted by different studies. Restriction of studies to single centers, inherent selection bias in established lupus cohorts and variable disease duration remain potential confounders. Attributing a neuropsychiatric manifestation directly to SLE remains challenging in view of the lack of diagnostic gold standards and overlap with common diseases like headache, anxiety, and depression. 5 Thus, it is not surprising that methodological differences in determining these manifestations have also contributed to the large variation in prevalence seen in the literature.
As clinical manifestations of SLE do depend on underlying genetic factors, one can expect that semiology and frequencies of neuropsychiatric manifestations in SLE will vary from population to population. Surprisingly, there is a paucity of well-conducted studies exploring neuropsychiatric manifestations of SLE in Indian population. Thus, we planned this study to delineate the prevalence and clinical profile of neuropsychiatric SLE (NPSLE) in the North Indian population as well as to study their impact on quality of life (QoL).
Methods
Patients
This study was conducted in a University Hospital in North India and included consecutive patients with SLE who attended the outpatient clinic or were admitted between 1 January 2015 and 30 July 2016. Patients satisfied the Systemic Lupus International Collaborating Clinics (SLICC) Classification 2012 criteria 6 and were 18 years of age or older. The institutional ethics committee approved the study and written informed consent was obtained from all participants.
Clinical assessment for neuropsychiatric manifestations
All included SLE patients underwent a complete clinical evaluation with history, file review, and clinical examination to screen for current or past neuropsychiatric manifestations. A final diagnosis of a neuropsychiatric syndrome was made as per the definition and diagnostic criteria of the American College of Rheumatology (ACR) 1999 definitions. 7 Some modifications or simplifications were used. These included (a) to exclude non-specific headaches, this study included headaches that lasted at least four hours and were unresponsive to analgesics including opioids; (b) to classify patients as having a mood disorder or anxiety, patients who reported symptoms leading to “significant distress or impairment in social, occupational, or other important areas of functioning” (statement taken from ACR 1999 definitions) were evaluated and the diagnosis confirmed by a psychiatrist; (c) to evaluate cognitive impairment, patients with a score of 23 or less on the mini-mental state exam were labeled as having cognitive impairment. No other formal testing/questionnaires or neurocognitive battery was used; (d) to evaluate the presence of autonomic neuropathy, measuring the orthostatic drop in blood pressure on standing (fall ≥30/15 mm hg was considered abnormal) was used; and (d) symptoms of peripheral neuropathy were screened using the diabetic neuropathy symptom (DNS) score. 8 This consists of questions on unsteadiness, pain or tenderness, pricking sensation, and numbness. If any question was answered in the affirmative, nerve conduction tests were performed. In addition, in around one-fourth of the asymptomatic patients, nerve conduction tests were performed to assess subclinical neuropathy. In all patients, disease activity was measured in all cases by Safety of Estrogens in Lupus Erythematosus National Assessment (SELENA)-Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) scoring. 9
QoL
QoL was assessed in all patients by the EuroQol-5D questionnaire. 10 Both English and Hindi versions were made available to patients. The EuroQol questionnaire has scores on five dimensions of self-care, mobility, usual care, pain/discomfort, and anxiety depression. Patients were asked to indicate their health state by ticking one of the three appropriate statements in each of the five dimensions. These three statements corresponded to no problem, some problem or unable to do (or extreme in case of pain and anxiety/depression). In addition, patients rated their global health on a visual analog scale from 0 to 100.
Statistical analysis
Variables are presented as mean ± SD (standard deviation) and categorical variables as percentages. Chi-square test was used to analyze categorical variables between two groups (NPSLE compared to no NPSLE). Means were compared by student t test for normally distributed data between two groups. Mann–Whitney U and Kruskal–Wallis tests were used to analyze QoL between different patient groups (non-normally distributed). A p value of < 0.05 was considered significant. All tests were two sided.
Results
Demographic characteristics of the study population
Comparison of clinical and investigational parameters in patients with and without neuropsychiatry manifestations of systemic lupus erythematosus
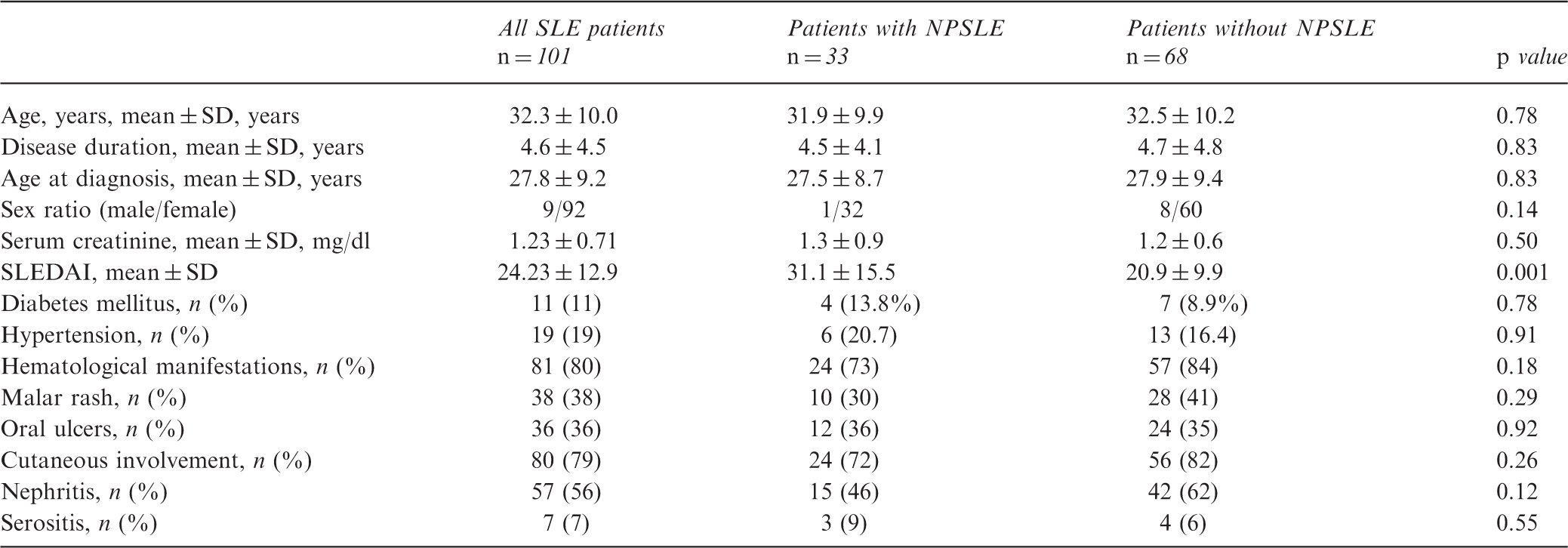
NPSLE: neuropsychiatric systemic lupus erythematosus; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index.
Prevalence of neuropsychiatric manifestations
Prevalence of neuropsychiatric manifestations
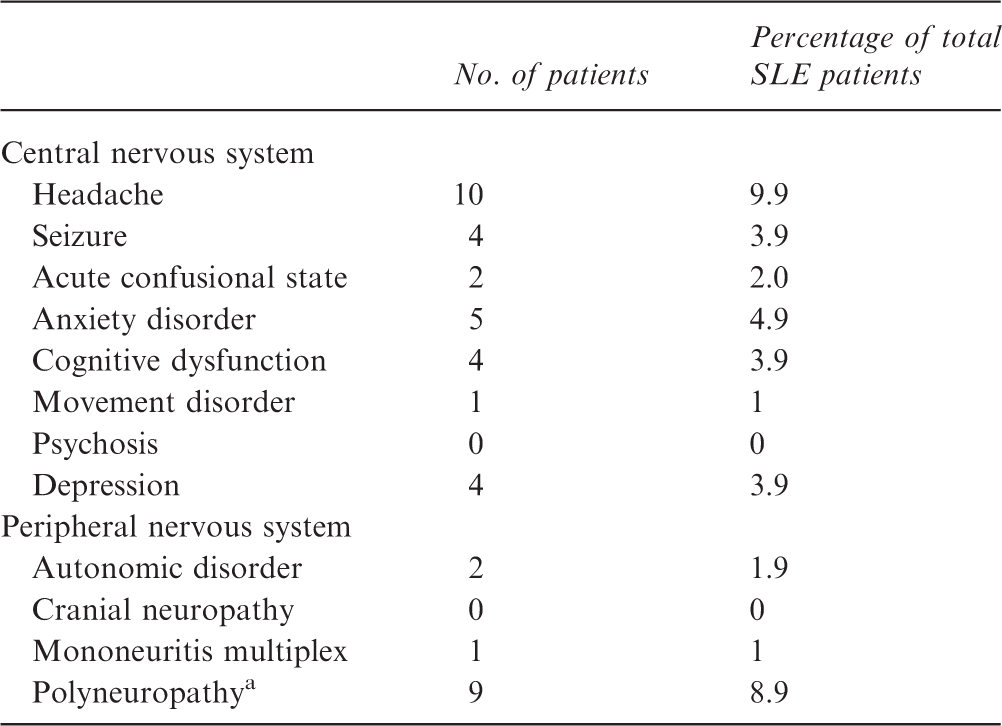
Among these, four were asymptomatic (out of 29 screened) and five had symptoms.
Among central nervous system manifestations, headache occurred in 10 patients. All these patients had tension-type headaches, with no patient reporting migrainous headache. Seven of these patients had isolated headache, while two had associated neuropathy and one had associated seizures. Cognitive dysfunction was seen in four patients. One patient with cognitive dysfunction also had chorea while one had coexistent mononeuritis multiplex and lupus nephritis. Depression was seen in four patients. Two patients with depression had lupus nephritis while one had coexistent myocarditis. Seizures were seen in four patients, being the presenting manifestation in one of them. Among them, magnetic resonance imaging (MRI) of the brain revealed periventricular white matter abnormalities in three patients and cerebrospinal fluid (CSF) evaluation showed lymphocytic pleocytosis with normal sugar and mildly elevated protein in all. One patient had hemichorea that responded to pulse methylprednisolone and cyclophosphamide. MRI of the brain revealed bilateral basal ganglionic hyperintensities in this patient.
Among peripheral nervous system manifestations, five patients had symptomatic peripheral neuropathy. In addition, screening electrophysiological testing was carried out in 29 asymptomatic patients, of whom four had subclinical neuropathy. Thus, the incidence of neuropathy in our cohort was 8.9% (9/101). Two patients had autonomic neuropathy and one had mononeuritis with foot drop and right median nerve palsy.
Comparison of patients with and without NPSLE
There were no statistically significant differences in the prevalence of lupus nephritis, hematological manifestations, serositis, malar rashes, or cutaneous manifestations in patients with NPSLE compared to those without NPSLE. However, current SLEDAI of neuropsychiatric patients was significantly higher than those without NPSLE (p = 0.001) (Table1).
QoL
Proportion of patients with levels of difficulty by EuroQol dimension
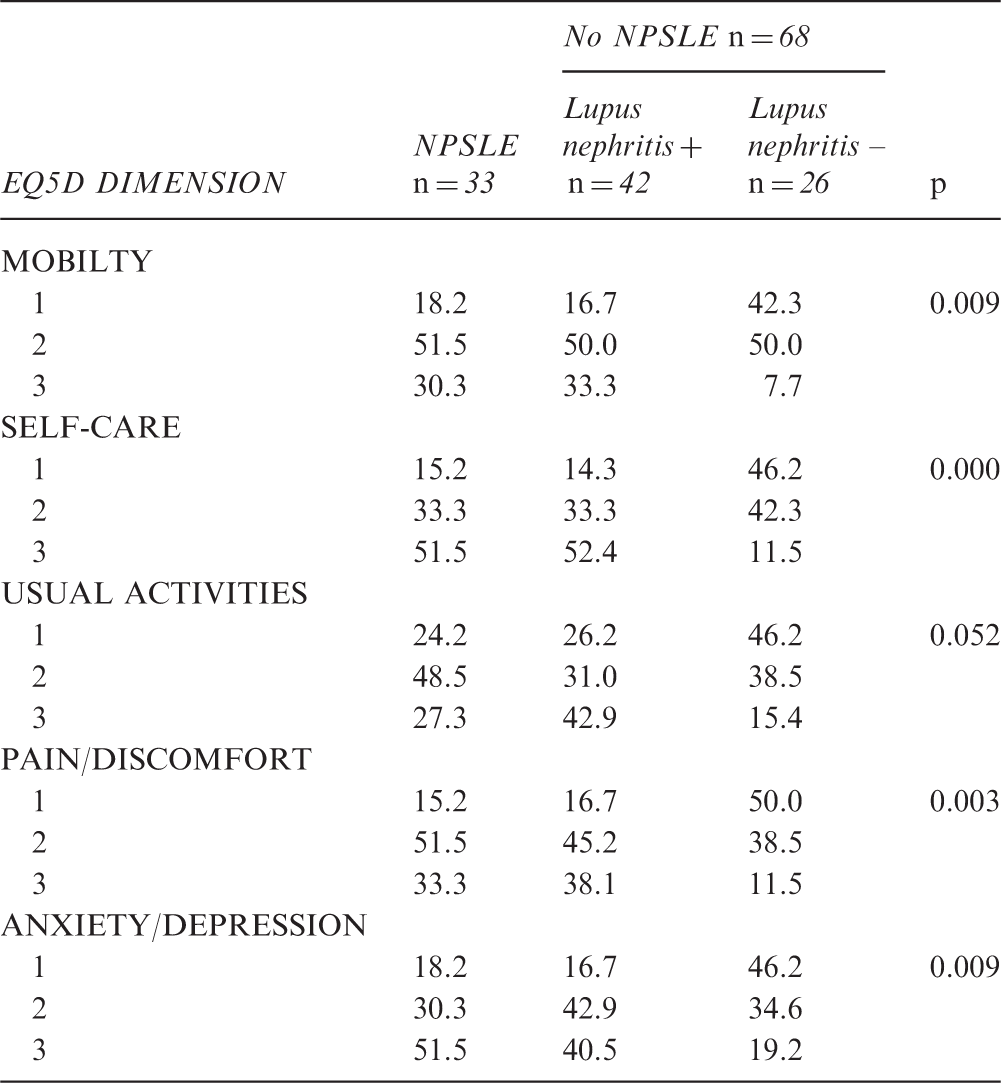
1: no problem/no symptom; 2: some problem/some symptom; 3: lots of problems/lots of symptoms; NPSLE: neuropsychiatric systemic lupus erythematosus.
Discussion
This study found neuropsychiatric manifestations in nearly one-third of lupus patients in a North India university center. This is similar to some of the previous studies like those by Hanly et al. (30.4%) and Yu et al. (34.6%).11,12 However the reported prevalence varies widely between various studies conducted across the world from 20% to 90%13–21 (Figure 1). This is due to the use of differing definitions and criteria used. Indeed, it is difficult to have uniform definitions for many NPLSE manifestations, especially cognitive and psychiatric manifestations. We have used simplified criteria and expert diagnoses that may lack sensitivity but are expected to be specific.
Prevalence of NPSLE in various studies across the world.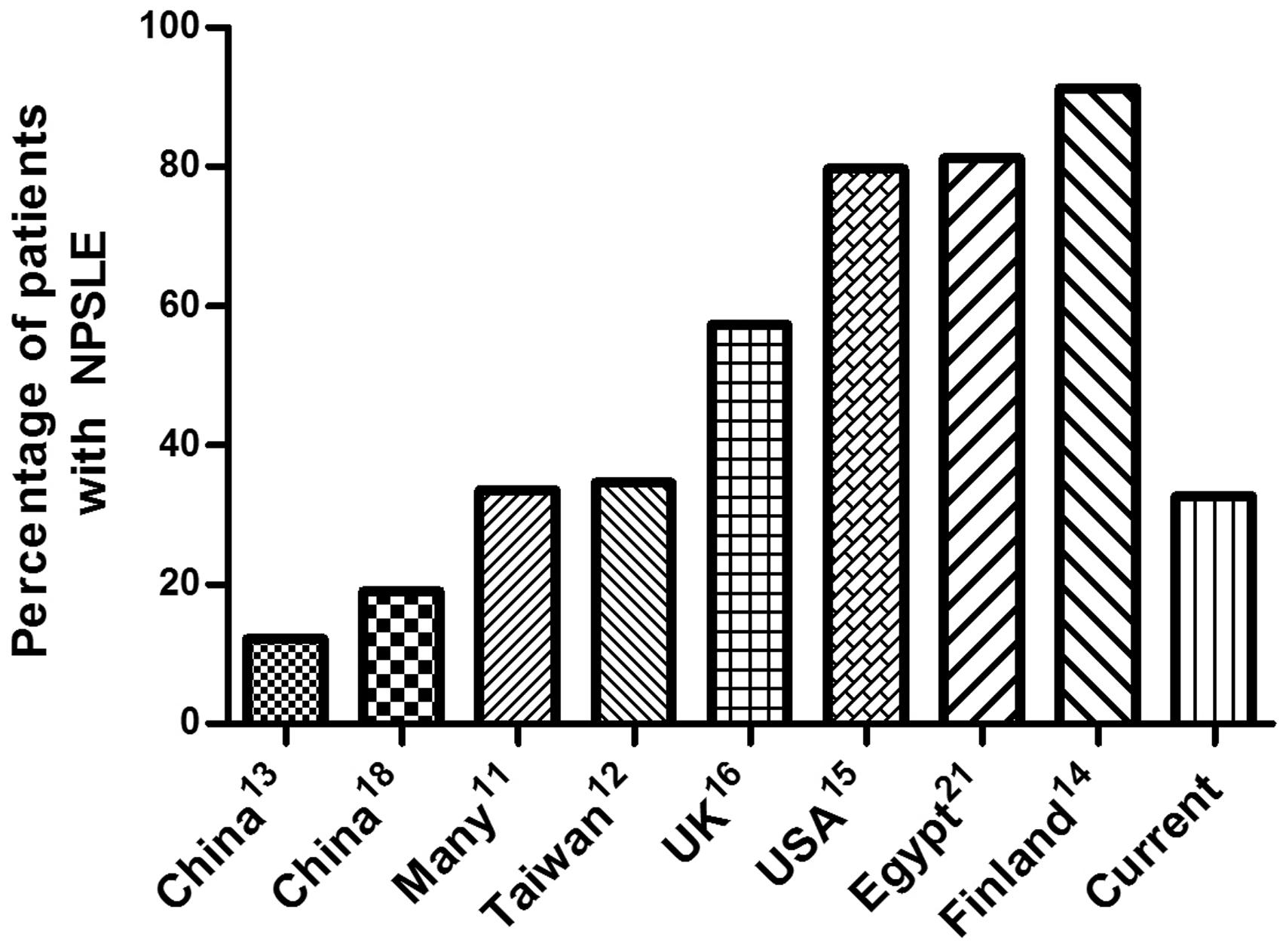
The most common neuropsychiatric manifestation in our study was headache. Indeed, headache has consistently been found to be the most frequent in different series worldwide with a prevalence ranging from 3.6% to 54.3%.13–17 We did try to keep a stricter definition and included only those patients whose headaches lasted at least four hours and were unresponsive to analgesics including opioids. This was based on initial studies suggesting that most lupus-associated migrainous headaches last longer than four hours. 22 In addition, keeping a longer duration (like three days as in the British Isles Lupus Assessment Group (BILAG)-2004 for scoring as active manifestation) was thought to be highly restrictive for the purpose of this study. 23 Surprisingly the most common type was tension and not migrainous headaches. Among the other central nervous system manifestations, the prevalence of seizures in our study was less than 10% as in many other series11,13,14,16 and movement disorder was uncommon (1% or less).
As to peripheral nervous system involvement, our study found the prevalence of autonomic neuropathy, mononeuritis multiplex, and peripheral polyneuropathy to be 1.9, 1, and 8.9% respectively. Previously some studies have found a similar high prevalence ranging from 13.1% to 28.3%,14,15,17 whereas others have reported a low prevalence ranging from 0.6 to 2.8%.11–13 The higher prevalence in our study is partly due to screening that was performed in almost one-fourth of the patients who were asymptomatic that revealed subclinical neuropathy in a significant number of patients. The cause of neuropathy in SLE ranges from inflammation due the disease (autoimmunity), vasculopathy that may be related to antiphospholipid antibodies, and drugs. 24 However, we did not conduct any further investigations to elucidate possible etiologies in this study.
In our study, no significant association was observed between NPSLE and other clinical features of SLE including hematological manifestations, nephritis, and cutaneous manifestations like malar rash or photosensitivity. Previously, variable associations have been described. One study observed significantly higher hematological manifestations in NPSLE patients; 18 however, it has not been found in other studies.19,25 Similarly, an association between nephritis and neuropsychiatric damage was shown in one of the prospective studies, 19 but no association was found in other studies between NPSLE and nephritis.20,25 Previous studies have also found an association between antiphospholipid antibodies and NPSLE. 18 However, we did not evaluate this aspect. In our study, significantly higher SLEDAI scores were found in patients with NPSLE compared to those without NPSLE, as has been found in many previous studies.12,18–20 Another limitation of our study is that we did not evaluate the occurrence of anti-NDMA or ribosomal-P associated with these patients.
Our study also showed a significantly lower QoL in patients with NPSLE compared to those without NPSLE or nephritis. However, there were no statistical differences between lupus nephritis and NPSLE patients. Our study suggests a significant impact of NPSLE manifestations on QoL. Surprisingly, despite a high prevalence of neuropsychiatric events, there have been relatively few studies to study their impact on QoL in these patients. Hanly et al. used the Short Form 36 (SF-36) health survey and also observed lower scores in NPSLE patients. 26 This is an area that requires greater research to evaluate the effect of therapies on QoL in these patients.
In conclusion NPSLE was found to be relatively common in Indian SLE patients, with headache, anxiety, and peripheral neuropathy being common manifestations. NPSLE was found to have a significantly detrimental effect on QoL.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.