
Abstract
Objective
This study sought to evaluate the effects of a nutritional intervention on the lipid metabolism biomarkers associated with cardiovascular risk, and their variation over time, in juvenile systemic lupus erythematosus (JSLE) patients. This study also investigated the relationships between these biomarkers and dietary intake, nutritional status, disease variables, and medication used.
Methods
A total of 31 10- to 19-year-old female adolescents with JSLE for at least six months were analyzed. The participants were randomly allocated to two groups: nutritional intervention or control. The intervention group received verbal and printed nutritional instructions once per month over nine months. Before and after the intervention, the participants underwent assessments of anthropometry; dietary intake; physical activity; socioeconomic status; total cholesterol and fractions; triglycerides; apolipoprotein A (Apo A-I); apolipoprotein B (Apo B); paraoxonase (PON) activity (a) and amount (q); myeloperoxidase (MPO); and small, dense LDL-c (sdLDL) particles.
Results
After nine months, we found significant reductions in the calorie, carbohydrate, total fat, saturated fat, and trans fat intakes in the intervention compared with the control group over time. The PONa/HDL-c ratio increased by 3.18 U/ml/mg/dl in the intervention group and by 0.63 U/ml/mg/dl in the control group (p = 0.037). Unlike the intervention group, the sdLDL levels of the control group worsened over time (p = 0.018).
Conclusion
The present study detected a reduction in calorie and fat intake, which indicates an improvement of HDL-c function and possible protection against cardiovascular risk for the intervention group.
Keywords
Introduction
Patients with systemic lupus erythematosus (SLE) are at high risk for premature atherosclerosis. The risks of nonfatal myocardial infarction and coronary artery disease among 18- to 44-year-old patients with SLE are two and 17 times higher than the general population, respectively. 1 The frequency of dyslipidemia is higher among children and adolescents with juvenile-onset SLE (JSLE) compared with the overall pediatric population. 2
SLE-related dyslipidemia and atherosclerosis have multifactorial origins as well as relationships with traditional and non-traditional risk factors such as disease activity, increased proinflammatory cytokine production, increased lipoprotein oxidation, endothelial dysfunction, the presence of autoantibodies, the use of glucocorticoids and other drugs, and kidney involvement.3–5
Recently published cohort studies of the biomarkers related to cardiovascular risk (CVR) in children and adolescents with SLE have reported higher concentrations of small, dense low-density lipoprotein cholesterol (LDL-c) (sdLDL) particles in association with disease activity, reduced apolipoprotein A-I (Apo A-I) and increased apolipoprotein B (Apo B).6,7 A reduction in serum paraoxonase (PON) concentration was found in adults with SLE, showing a negative correlation with CVR. Furthermore, an increase in myeloperoxidase (MPO) concentration was described.8–11
Nutritional intervention studies aimed at promoting dietary changes have shown efficacy with regard to reducing body weight; calorie, total fat, and saturated fat intake; 12 and lipid metabolism biomarker levels in adults with SLE.13,14 No similar studies have been conducted with pediatric patients.
Considering the high frequency of CVR factors in patients with SLE, the need to extend knowledge regarding lipid metabolism markers, and the lack of well-defined protocols for pediatric patients, nutritional intervention studies are needed to reduce the aforementioned factors.12–14
The present study sought to investigate the effects of a nutritional intervention on the CVR-related lipid metabolism biomarkers, and their variation over time, in adolescents with JSLE. This paper also assessed the associations between these biomarkers and dietary intake, nutritional status, disease variables, and medications used.
Methods
A total of 43 10- to 19-year-old female adolescents were followed up from March to December 2013 at a pediatric rheumatology outpatient clinic. A total of 31 adolescents with JSLE were included in a randomized, controlled nutritional intervention study that lasted nine months.
JSLE diagnosis was established based on the recommendations of the American College of Rheumatology (ACR). 15 Patients with JSLE for at least six months with any clinical manifestation or any degree of disease activity were included. Pregnant adolescents (n = 2) were excluded, as were those with active nephrotic syndrome (n = 1), chronic kidney failure (n = 2), liver failure (n = 0), hypothyroidism (n = 1), diabetes (n = 0), dyslipidemia requiring pharmacological treatment (n = 2), delayed neuropsychomotor development (n = 1), and those who did not adhere to treatment (n = 3). The institutional research ethics committee approved this study (CEP 195.789); informed assent and consent were obtained from the participants and their parents/guardians, respectively.
Using Random Allocation for Windows, 16 the participants were randomly allocated to two groups: The first underwent a nutritional intervention, and the second acted as the control group. The rheumatologists and laboratory staff were blinded to participant allocation.
The nutritional intervention included six steps at monthly intervals and three reinforcement visits regarding the subjects discussed, for a total of nine meetings. The same nutritionist provided verbal instructions on an individual basis.
A printed booklet containing instructions based on the guidelines for dyslipidemia was provided as support material. The verbal instructions were developed and delivered to the participants and their relatives.17,18 The participants also received individual diet plans that were elaborated by the Institute of Medicine, Dietary Reference Intakes (DRI). 19
At each intervention visit, the participants received one booklet chapter (i.e., the one that corresponded to the subject discussed). If the participants missed a visit, then the corresponding subject was discussed at another time.
The intervention included the following six steps: (a) general orientation on dietary behavior; (b) notions of healthy eating based on food rotation; (c) emphasis on adequate carbohydrate and fat intake, including types of fat and attention to food labels; (d) orientation on adequate salt, sugar, diet, and light foodstuffs intake; (e) qualitative changes emphasizing fruit and vegetable (antioxidants), sea fish (omega-3), and soluble and insoluble fiber consumption; and (f) orientation on diet and lifestyle, frequency of eating at snack bars, sedentary and leisure activities on weekends, and participation in parties and other events.
The participants received an anthropometric assessment at the beginning and end of the study that included measurements of body mass index (BMI) and height for age (H/A) 20 classified according to the World Health Organization criteria. 21 Pubertal staging was performed according to Marshall and Tanner, considering breast development (B) only. 22
Participant food intake was assessed once per month based on a 24-hour diet recall. 23 Macronutrient, total fat, cholesterol, and mono-, polyunsaturated, saturated, and trans fat intakes were calculated using the Nutrition Support Program (Programa de Apoio à Nutrição, version 2.5 NutWin/Unifesp), 24 which uses the United States Department of Agriculture (USDA) Food List as a database and includes data from the Brazilian List of Food Composition (Tabela Brasileira de Composição de Alimentos; TACO). 25
The data related to disease were collected from participants' medical records, including the Systemic Lupus Erythematosus Disease Activity Index-2000 (SLEDAI-2K) 26 and the Systemic Lupus International Collaborating/ACR Damage Index (SLICC-ACR/DI) 27 scores that corresponded to the date of the sample collection. Questionnaires were applied to collect data regarding physical activity, 28 socioeconomic level, 29 and family CVR. 30
Blood samples were collected in duplicate after a 12-hour fast at the beginning and end of the study for analysis of the following lipid metabolism biomarkers: total cholesterol, high-density lipoprotein cholesterol (HDL-c), LDL-c, and triglycerides (TG) via the enzymatic calorimetric method; paraoxonase 1 activity (PONa) via a kinetic spectrophotometric method using a paraoxon diethyl-p-nitrophenyl phosphate reagent (Sigma-Aldrich); paraoxonase 1 amount (PONq) using a sandwich enzyme-linked immunosorbent assay (ELISA) kit (MyBioSource, San Diego, CA, USA); sdLDL via a competitive inhibition enzyme immunoassay (Cusabio, China); Apo A-I and Apo B 100 using ELISA kits (Mabtech, Cincinnati, OH, USA); and MPO using an ELISA kit (MyBioSource, San Diego, CA, USA).
In addition, the following parameters were analyzed: high-sensitivity C-reactive protein (hs-CRP) via a particle-enhanced immunoturbidimetric method; blood glucose via an enzymatic colorimetric method; and insulin via chemiluminescence. Fasting blood glucose and insulin values were used to calculate Homeostasis Model Assessment of Insulin Resistance (HOMA-IR). 31
The lipid profile was classified based on the cutoff points recommended by the American Academy of Pediatrics. 32 The non-HDL-c (NHDL-c) value was calculated and classified according to the Bogalusa Heart Study. 33 In addition, the following ratios were calculated: total cholesterol/HDL-c, LDL-c/HDL-c, Apo B/Apo A-I, TG/HDL-c, LDL-c/Apo B, and PONa/HDL-c.
The statistical analysis was performed using Stata 12.0. The dichotomous variables were expressed as absolute numbers and percentage. The continuous variables were tested for normality using the Kolmogorov-Smirnov test. Since all the variables were parametric they were expressed as mean±standard deviation.
The Chi-square test or exact Fisher's test were used in the bivariate analysis for the comparison of the categorical variables between the intervention and control groups. The McNemar's test was used for pairwise analysis of the categorical variables between beginning versus end of the intervention. Similarly, the pairwise Student t-test was used for comparison between intervention versus control groups at the beginning and end of the intervention.
The multivariate analysis employed mixed linear regression models to evaluate the effects of explanatory variables (time, group, SLEDAI, use of medication, nutritional status, body composition, food consumption, physical activity, and ultrasensitive CRP levels) on each of the numeric dependent variables (total cholesterol, LDL-c, HDL-c, TG, non-HDL-c, Apo-B, Apo-A-I, sdLDL, MPO, and PONa).
At first a logistic regression model with random effect was adjusted for the variables with dichotomous characteristics, in a similar way as for those with numeric characteristics. Alternatively, a logistic regression model with cluster robust approaches, which corrects standard errors of estimates considering observations in one individual, was employed.
Variables with significance at 2% in the bivariate model were selected for the linear regression as well as for the logistic in the model. Initially all selected variables were included. The variables that were not significant at 5% were then excluded in sequence in order of significance (backward method). All statistical tests adopted a 5% significance level.
Results
General characteristics of adolescents with JSLE at baseline
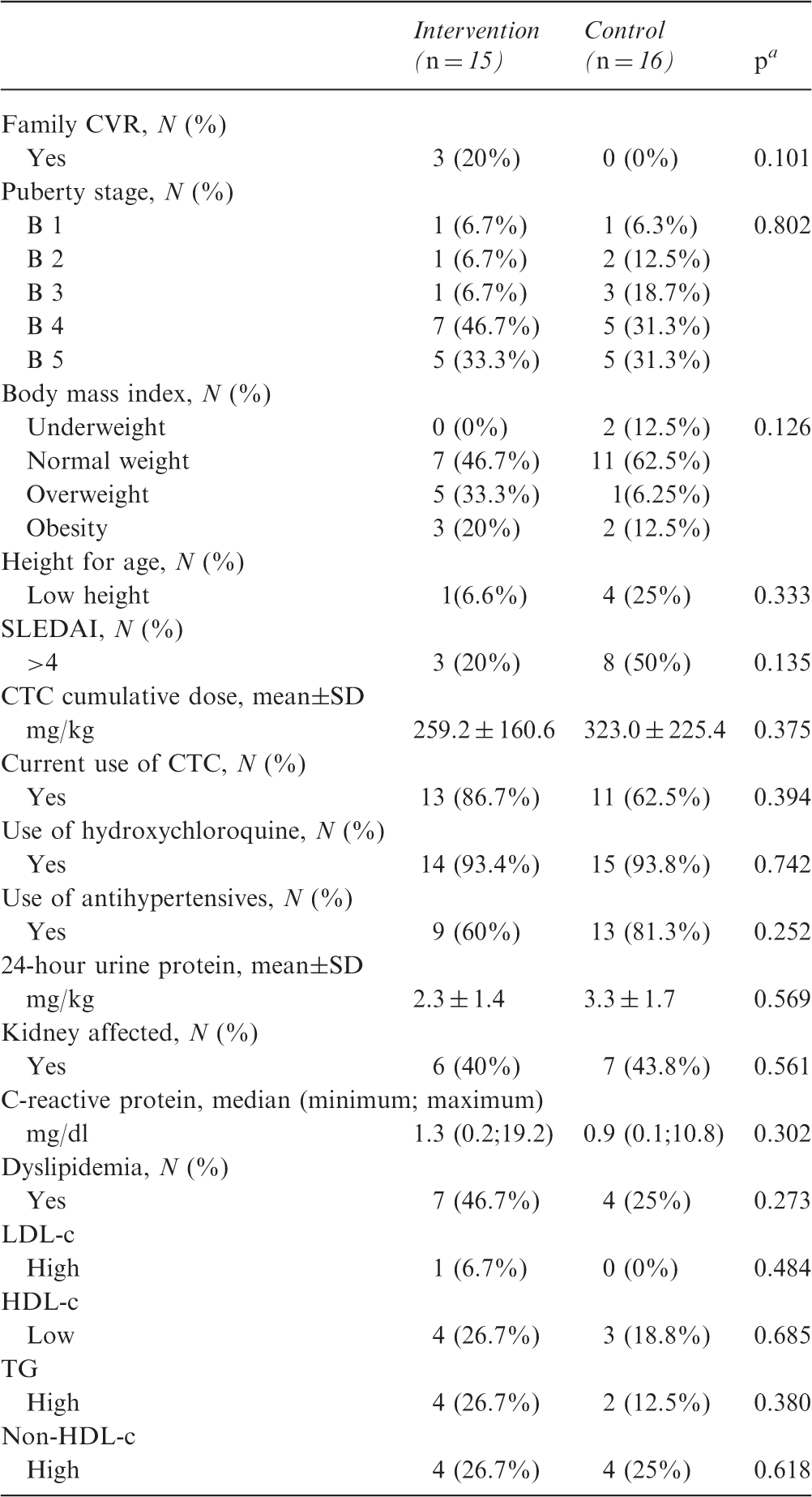
JSLE: juvenile systemic lupus erythematosus; CVR: cardiovascular risk; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; CTC: corticosteroids; LDL-c: low-density lipoprotein cholesterol; HDL-c: high-density lipoprotein cholesterol; TG: triglycerides; B: breasts; B 1: pre-adolescent; elevation of papilla only. B 2: breast bud stage; elevation of breast and papilla as a small mound, enlargement of areola diameter. B 3: further enlargement of breast and areola, with no separation of their contours. B 4: projection of areola and papilla to form a secondary mound above the level of the breast. B 5: mature stage, projection of papilla only, due to recession of the areola to the general contour of the breast. 22
p: Chi-square or Fisher's exact test significance level.
The average ages of the participants in the intervention and control groups at baseline were 15.7 ± 2.9 years old and 15.3 ± 2.3 years old, respectively (p = 0.712); the average durations of disease, SLEDAI-2K, and SLICC/ACR-DI were 50.8 ± 31.4 months and 62.2 ± 35.8 months (p = 0.359); 2.2 ± 3.1 and 3.7 ± 4.0 (p = 0.243); and 0.3 ± 0.6 and 0.2 ± 0.4 (p = 0.699), respectively. The control and intervention group were classified according to their socioeconomic level as moderate (p = 0.435).
At baseline, dyslipidemia was detected in 7/15 (46.7%) and 4/16 (25%) participants from the intervention and control groups, respectively; this difference was not significant (p = 0.273; Table 1). At the end of the study, dyslipidemia was detected in 4/15 (26.7%) and 6/16 (37.5%) participants from the intervention and control groups, respectively; this difference was not significant (p = 0.398).
Dietary intake of adolescents with juvenile systemic lupus erythematosus at the beginning and end of the study by group—nutritional intervention and control
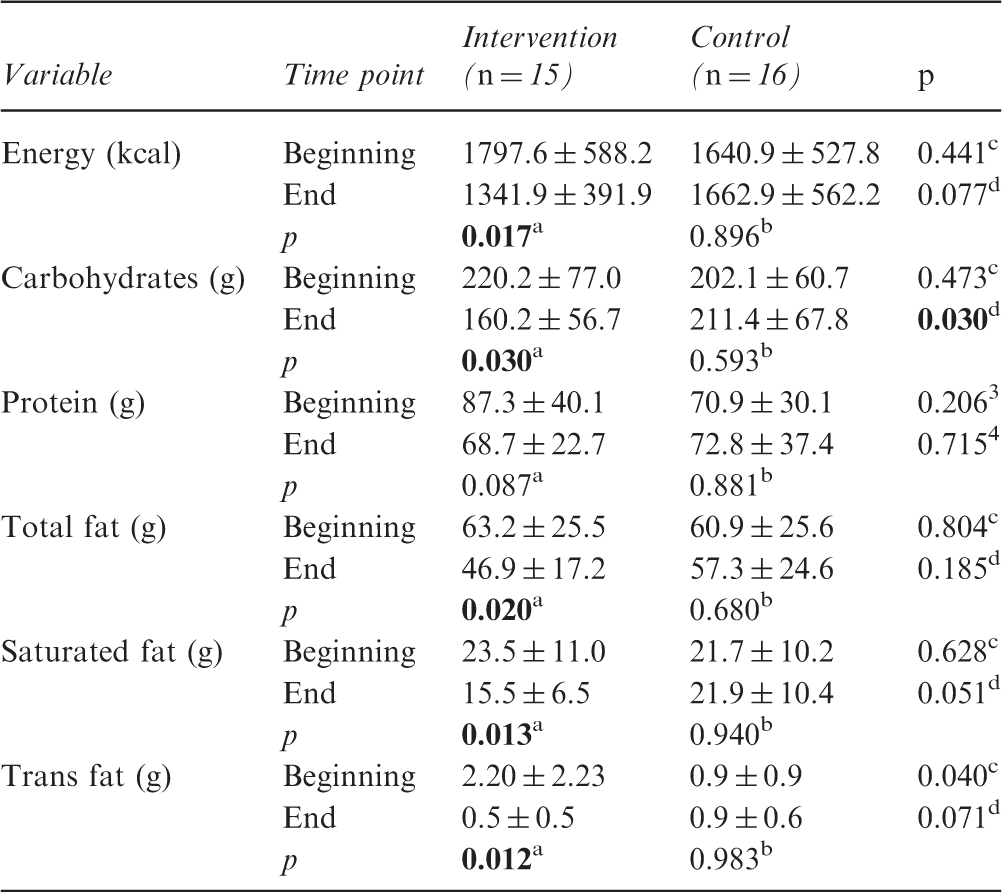
p: paired Student's t-test significance level (intervention group at the beginning and end of the study).
p: paired Student's t-test significance level (control group at the beginning and end of the study).
p: independent-samples Student's t-test significance level (intervention group vs. control group at the beginning of the study).
p: independent-samples Student's t-test significance level (intervention group vs. control group at the end of the study). Bold values signify p<0.05.
Physical activity, disease activity (SLEDAI-2K), and BMI of adolescents with JSLE at the beginning and end of the study by group—nutritional intervention and control
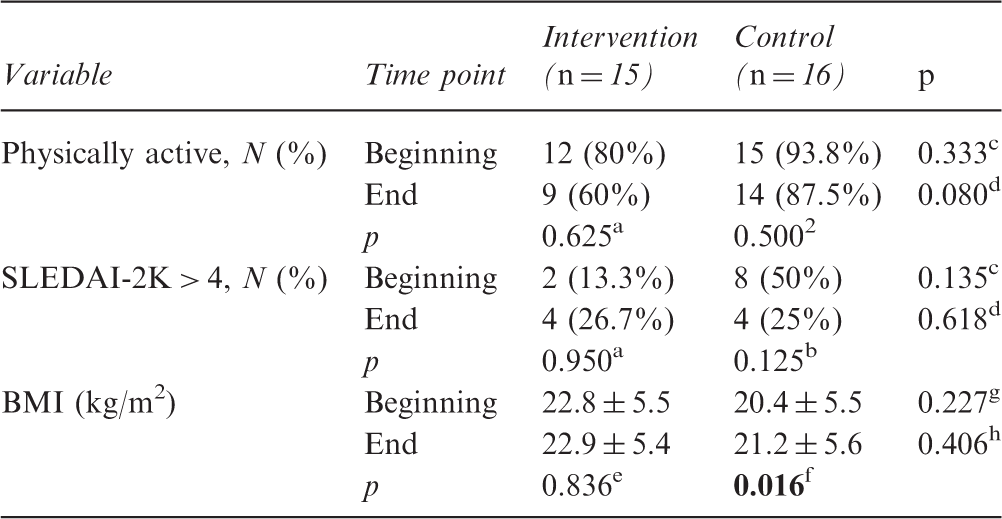
JSLE: juvenile systemic lupus erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index-2000; BMI: body mass index.
p: McNemar's test significance level (intervention group at the beginning and end of the study).
p: McNemar's test significance level (control group at the beginning and end of the study).
p: Chi-square or Fisher's exact test significance level (intervention group vs. control group at the beginning of the study).
p: Chi-square or Fisher's exact test significance level (intervention group vs. control group at the end of the study).
p: paired Student's t-test significance level (intervention group at the beginning and end of the study).
p: paired Student's t-test significance level (control group at the beginning and end of the study).
p: independent-samples Student's t-test significance level (intervention group vs. control group at the beginning of the study).
p: independent-samples Student's t-test significance level (intervention group vs. control group at the end of the study). Bold values signify p<0.05.
Lipid and glucose metabolism biomarkers in adolescents with JSLE at the beginning and end of the study by group—nutritional intervention and control
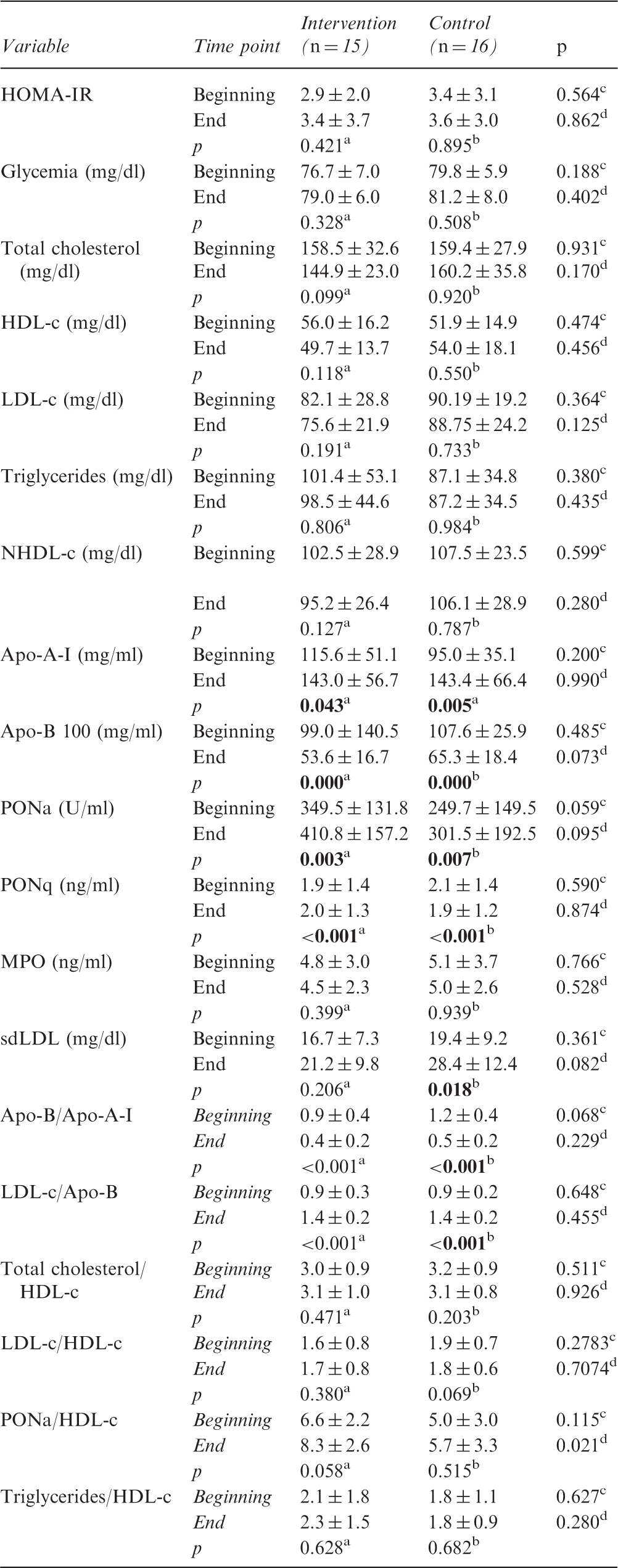
JSLE: juvenile systemic lupus erythematosus; HOMA-IR: Homeostasis Model Assessment of Insulin Resistance; HDL-c: high-density lipoprotein cholesterol; LDL-c: low-density lipoprotein cholesterol; NHDL-c: non-high-density lipoprotein cholesterol; Apo A-I: apolipoprotein A-I; Apo B: apolipoprotein B; PONa: paraoxonase activity; MPO: myeloperoxidase; sdLDL: small, dense low-density lipoprotein cholesterol.
p: paired Student's t-test significance level (intervention group at the beginning and end of the study).
p: paired Student's t-test significance level (control group at the beginning and end of the study).
3p: independent-samples Student's t-test significance level (intervention group vs. control group at the beginning of the study).
4p: independent-samples Student's t-test significance level (intervention group vs. control group at the end of the study). Bold values signify p<0.05.
Mixed linear regression model with interaction between time and group for PONa/HDL-c ratio
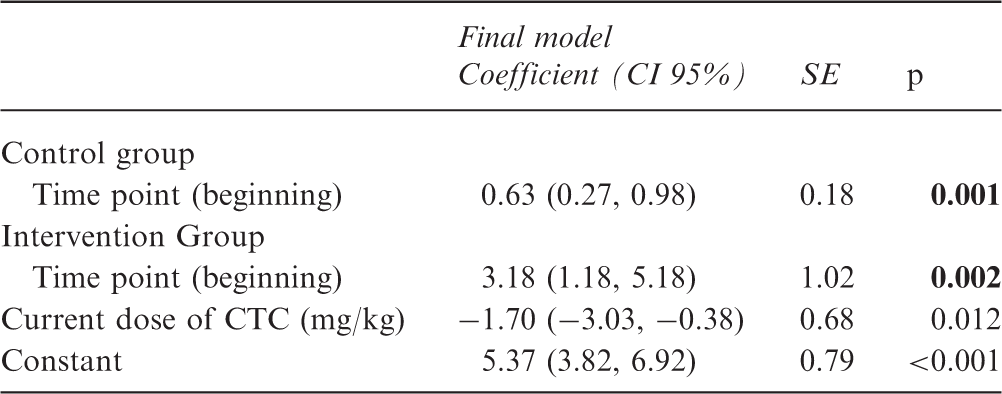
PONa: paraoxonase activity; HDL-c: high-density lipoprotein cholesterol; CTC: corticosteroids; CI: confidence interval; SE: standard error.
Variables in the initial model: time point, group, physical activity, current dose of corticosteroid (mg/kg), renal impairment, fat percentage, dietary intake (calories, total fat, saturated, and trans fat).
Variables in the final model: time point (reference = beginning), group (reference = control), and corticosteroid current dose (mg/kg). Bold values signify p<0.05.
Discussion
This pioneering study investigated the effects of a nutritional intervention on the lipid and glucose metabolism of adolescents with SLE. We found higher PON activity among the HDL-c particles and reductions in calorie and saturated and total fat intakes among the participants who received intervention, which indicates better HDL-c function and a consequent reduction in CVR. The concentration of sdLDL, which are also atherogenic particles, increased in the control group.
No previous nutritional intervention studies have sought to reduce lipid metabolism markers using well-defined protocols in pediatric patients. In addition, the studies conducted with adults12–14 have applied briefer interventions and have not assessed specific biomarkers such as sdLDL, MPO, Apo A-I, Apo B, or PON activity.
One nutritional intervention program seeking to reduce CVR in adult women with SLE found significant reductions in total cholesterol, LDL-c, TG, body weight, and total and saturated fat intake at a 12-week follow-up assessment. 13 Another study detected a reduction in the plasma cholesterol concentration after six weeks of nutritional counseling based on North American guidelines. 14 The present study did not detect significant changes in the classic lipid profile following nutritional intervention. The following hypotheses might account for this finding: (a) The sample was composed of adolescents who experience continuous changes in their body compositions and lipid profiles, and they have difficulty changing their dietary habits; 34 (b) JSLE is more aggressive than the adult form of the disease; 35 and (c) a physical activity protocol was lacking.
Although BMI did not change in the intervention group, it significantly increased in the control group, which suggests that the intervention had benefits for the former group. Importantly, the groups did not differ with regard to the dose of glucocorticoid used or the disease activity over time, which are factors that can influence BMI.
At the end of the nine-month intervention, we found a reduction in the carbohydrate intake of the intervention group compared with the control group as well as reductions in calorie and fat intakes within the intervention group over time. These findings beneficially reduce CVR at an age when changes in dietary habits are limited. 36
The HDL-c levels of most participants were adequate; however, the particles of this cholesterol component might become dysfunctional and pro-atherogenic during SLE-related systemic inflammation. Pro-inflammatory HDL-c is characterized by a reduction of the particles' Apo A-I and PON. 37
The present study did not detect variations in the Apo A-I, PONa, or PONq levels between the groups or within the groups over time. However, we found an increase in the PONa/HDL-c ratio, which suggests that PONa might be a more interesting marker than Apo A-I to assess HDL-c function. One way to estimate the amount of PON in HDL particles is calculating PON/HDL-c, which represents PON activity per HDL particles. Higher values correspond to higher PONa amount/activity per HDL particle. PON has protective effects against HDL-c and LDL-c peroxidation as well as postprandial oxidative stress; it inhibits the biosynthesis and stimulates the influx of cholesterol into macrophages, and it modulates lipid metabolism in adipose tissue. 38
sdLDL is atherogenic, susceptible to oxidative changes, and can negatively influence CVR. 39 Increased sdLDL particle concentration has been found in adolescents with SLE and correlated with disease activity. 6 Our study found a significant increase in this particle only in the control group; however, it was not associated with disease activity. This finding indicates that a nutritional intervention might contribute to cardiovascular protection.
hs-CRP did not change over time. As previous research has shown, hs-CRP is not a specific marker of disease activity in patients with SLE; rather, it increases only under conditions of serositis or infection. 40
The current nutritional intervention was effective because the atherogenic protection markers increased in the intervention group, and these participants exhibited satisfactory adherence to intervention. One possible explanation for this outcome might be the fact that participants complied with all of the steps that the same nutritionist provided throughout the nine-month intervention. Importantly, previous studies conducted with adults did not report details regarding participant adherence, and the interventions were briefer.12–14
Regarding the limitations of the present study, we call attention to our small sample size; the use of one 24-hour dietary recall per visit, which might not have reflected our participants' usual dietary intakes; and the lack of evaluation concerning acute-phase proteins and specific cytokines.
The present pioneering study found an improvement in the lipid marker profiles of the intervention group. This finding reinforces the relevance of nutritional intervention among adolescents with JSLE to reduce CVR.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: São Paulo Research Foundation (Fundação de Amparo à Pesquisa do Estado de São Paulo; FAPESP) (2012/08529‐8), Brazilian Federal Agency for Support and Evaluation of Graduate Education (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior; CAPES), and grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq 303752/2015‐7 to MTT).