
Abstract
Objective
This study aims to exhibit the prognosis, both mortality and morbidity, of patients with systemic lupus erythematosus (SLE) in a single-center cohort in China.
Methods
A cohort of Chinese SLE patients were recruited from April 2009 to February 2010, and followed up regularly in clinic at Peking Union Medical College Hospital (PUMCH). Data for baseline, follow-up, and survival were collected, including demography, manifestations, activity, the Systemic Lupus International Collaborating/American College of Rheumatology (SLICC/ACR) Damage Index (SDI), and medications. The Kaplan–Meier method was adopted for survival analysis. Predicting and risk factors for both mortality and morbidity were evaluated by the Cox proportional hazard model. Associated factors were analyzed by the logistic regression model.
Results
A total of 260 patients were included at entry. The one-, three-, and five-year survival rates were 98.4%, 95.5%, and 93.8%. The proportion of patients with organ damage increased from 13.4% at baseline to 28.4% at year 6. Regression analysis showed that organ damage led to higher mortality, and organ-involved flare was associated with more future damage. Time from onset to diagnosis > 1 year, nephropathy and severe organ involvement were potential prognostic factors. Furthermore, onset age > 50 and previous organ damage were predictors for further damage.
Conclusion
Organ damage, severe organ involvement, and prolonged remission could be targets for the management of Chinese SLE patients to further reduce mortality. Early diagnosis, paying more attention to severe organ involvement, and preventing organ-involved flares and new organ damage would be crucially important in the future for Chinese SLE patients.
Introduction
Systemic lupus erythematosus (SLE) is a chronic multisystem autoimmune disease with lifelong recurrent flares and sometimes severe, even fatal, episodes. With the development of diagnostic and treatment strategies, the long-term survival rates of SLE patients improved markedly from the 1950s to the 2000s. 1 Moreover, the meta-analysis that we previously published showed that the long-term survival rates of Chinese SLE patients are comparable to Caucasians.2,3 Nonetheless, the fact is that there are few studies focusing on the prognosis of Chinese SLE patients.
Apart from mortality, other clinical outcomes, such as organ damage and disease flares, are crucial for long-term prognosis of SLE patients. Therefore, to yield superior outcomes for SLE patients, treat-to-target (T2T in SLE) principles and recommendations were initially developed by an international task force in 2014. 4 Targeting at remission, preventing organ damage and improving quality of life were core concepts of these recommendations. It has been proposed in Caucasian cohort studies that organ damage predicts higher mortality and minimizing organ damage should be a goal of SLE treatment.5,6 Moreover, disease flares, or higher disease activity, was reported to be predictive for more damage in the future.7,8 Therefore, avoiding subsequent flares, in other words maintaining prolonged remission, should be an important treatment target for SLE patients. 4 However, no study has ever elaborated the characteristics and significance of organ damage and flares in Chinese SLE patients, so we lack relevant data from Chinese SLE patients to further verify those recommendations for T2T in SLE. It was reported that in China, the largest country in the Asia-Pacific area, the prevalence rate of SLE was 97.5–100/100,000, which was relatively higher when compared to other ethnic groups (generally 20–70/100,000), 9 meaning that we have the largest number of SLE patients. Therefore, we are in demand of more research from China to provide more evidence for T2T in SLE from patients with different races and genetic backgrounds.
This study is the first single-center cohort to illustrate different outcomes of Chinese SLE patients, including mortality, organ damage, and flares, aiming to display a panorama of the long-term prognosis as well as confirm the validity of the concepts of T2T in SLE for Chinese SLE patients.
Patients and methods
Patients and follow-up
The patients were recruited from April 2009 to February 2010 at Peking Union Medical College Hospital (PUMCH), and were all registered in the Chinese SLE Treatment and Research (CSTAR) registry cohort after informed consent forms were signed by themselves or their authorized guardians. 10 In addition, this study was approved by the Ethics Committee of PUMCH, Chinese Academy of Medical Sciences (approval number S-197). All patients were Chinese with SLE who fulfilled four or more items of the 1997 revised American College of Rheumatology (ACR) criteria. After enrollment, all patients were followed up at clinic at least once a year. Definition of lost to follow-up was as follows: the patient never came to clinic for follow-up and couldn’t be contacted, or he or she chose to discontinue participation after enrollment.
Definition of organ damage, severe organ involvement and disease flare
Organ damage is defined as irreversible tissue injury that occurs after SLE disease onset and persists for at least six months. 11 The Systemic Lupus International Collaborating/American College of Rheumatology (SLICC/ACR) Damage Index (SDI), which covers 12 organ systems, was adopted to evaluate organ damage of SLE patients. 12 Organ damage was recorded if the patient’s SDI score ≥ 1 point. Then the detail and occurrence time of the damage were supplemented.
Severe organ involvement is defined as several subtypes of SLE that were reported to be of low incidence and might have worse prognosis in different studies, including neuropsychiatric SLE (NPSLE), interstitial lung disease (ILD) caused by lupus, gastrointestinal involvement (GI) caused by lupus, and pulmonary arterial hypertension secondary to SLE (PAH).13,14
Different scoring systems have been developed to assess disease activity and define disease flares for SLE patients. 15 Among them, the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) is still the most prevalent for clinical practice. 16 SLEDAI-2K combined with treatment was applied to define disease flare. In our study, disease flare was identified if the patient’s episode fulfilled one of the following criteria: (a) SLEDAI-2K score > 4 points, with restarting or increasing corticosteroids or immunosuppressants; (b) new onset or worsening of SLE manifestations (not included in the SLEDAI-2K), with restarting or increasing corticosteroids or immunosuppressant agents.
Data collection
Baseline data were collected through the CSTAR online registry, including demography, clinical manifestations (including malar rash, discoid lesion, photosensitivity, oral ulcers, arthritis, serositis, hematologic involvement, nephropathy, NPSLE, and some rare organ involvements such as PAH that were detected by echocardiography, and ILD that was detected by chest X-ray or computerized tomography), laboratory results (including complete blood count, urine analysis, autoantibodies (antinuclear antibody (ANA), anti-double-stranded DNA (anti-dsDNA), anti-Sm, anti-Ro/SSA, anti-La/SSB, anti-RNP, anti-rRNP, and antiphospholipid antibodies (aPL)), SLEDAI-2K, SDI scores, and medications. Clinical records were reviewed to collect follow-up data, mainly for SLEDAI-2K, SDI scores, and therapy adjustment. Telephone interview was employed to supplement additional data for analysis.
Statistical analysis
The Kaplan–Meier (KM) method was adopted for survival analysis. A KM curve was performed to obtain one-, three-, and five-year survival rates. Cox regression analysis was applied to study the relationship between organ damage and death. Risk factors both for mortality and organ damage were evaluated by multivariate regression analysis of the Cox proportional hazard model. To avoid the influence of treatment, only newly diagnosed patients were included for regression analysis of organ damage. The definition of newly diagnosed patients was that the time from diagnosis to enrollment was less than one year. The results were presented as hazard ratios (HRs) and 95% confidence intervals (CIs). The statistical analysis was performed by SPSS 19.0.
Results
Baseline characteristics
A total of 260 patients were enrolled in our study. Among them, six patients were lost to follow-up after recruitment. The mean age at disease onset was 29.0 ± 11.6 years, and the mean age at diagnosis of SLE was 30.2 ± 11.6 years. The average age at entry was 32.0 ± 11.7 years, and the average time for follow-up was 6.18 ± 1.58 years. The clinical manifestations of our cohort were malar rash (42.5%), discoid lesions (7.1%), photosensitivity (20.9%), oral ulcers (21.7%), arthritis (45.7%), serositis (12.6%), hematologic involvement (54.3%), nephropathy (49.6%), NPSLE (9.8%), ILD (3.5%), GI (3.5%), and PAH (2.4%).
Mortality, organ damage, and flare
The one-, three-, and five-year survival rates of the involved 254 patients from enrollment were 98.4% (95% CI 96.8%–99.99%), 95.5% (95% CI 93.0%–98.0%), and 93.8% (95% CI 90.9%–96.7%). A total of 16 patients died during follow-up. The major causes were infection (six patients), severe active SLE (one hematologic and one neuropsychiatric), sudden cardiac death (one patient), cerebrovascular event (one patient), and undefined reasons (six patients).
At entry, 13.4% (34/254) of the patients had organ damage. It increased to 28.4% (67/236) at year 6. A total of 84 accumulated damages appeared in 67 patients. The top five damaged organs were musculoskeletal (32.14%), neuropsychiatric (17.86%), pulmonary (10.71%), peripheral vascular (9.52%), and ocular (9.52%) (Figure 1). A total of 175 patients were newly diagnosed and were included for regression analysis for organ damage.
Distribution of different accumulated organ damages.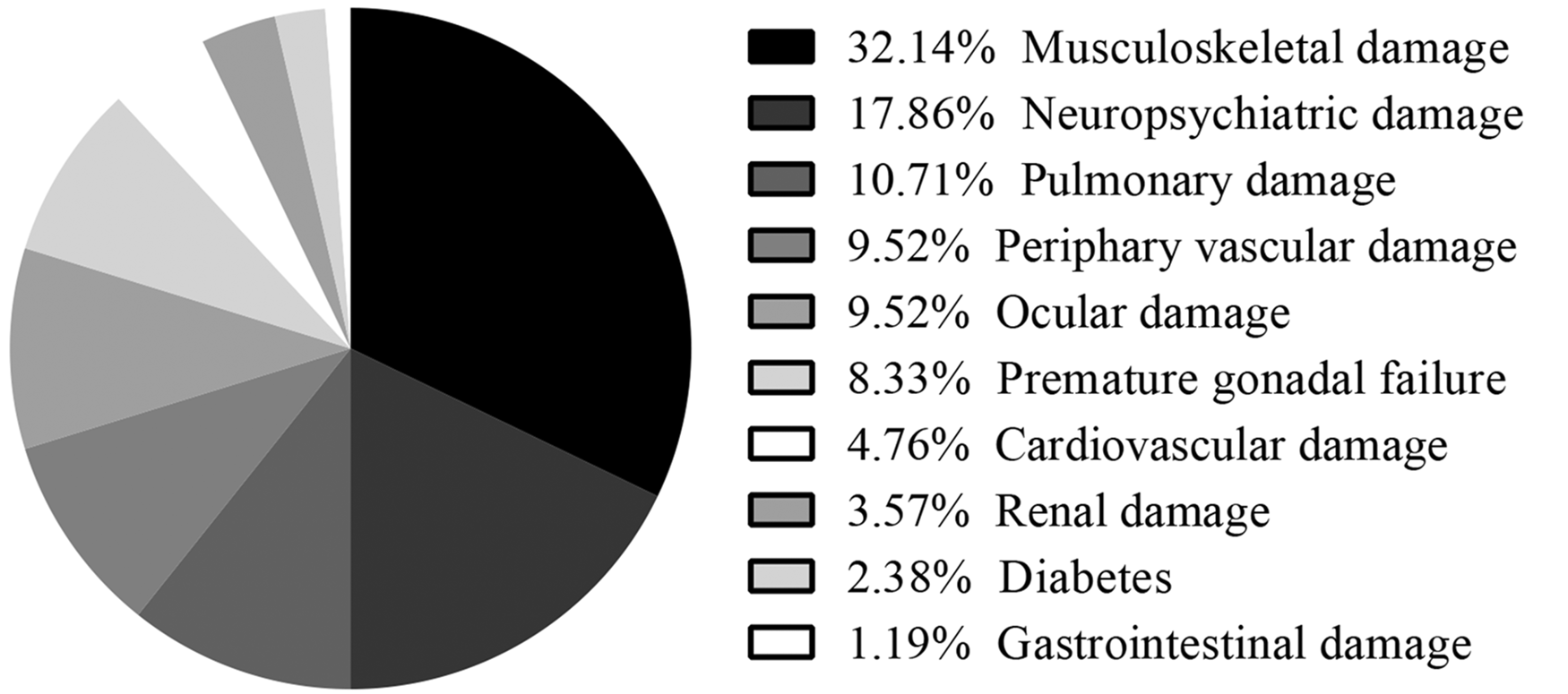
During follow-up, 227 flares were recorded in 254 patients. The flares were classified into different subtypes by different organs that were affected during disease flare. Among them, the top five kinds of flares were renal (30.40%), mucocutaneous (29.52%), hematologic (14.10%), articular (12.77%), and neuropsychiatric (3.52%) (Figure 2).
Proportion of different types of flares.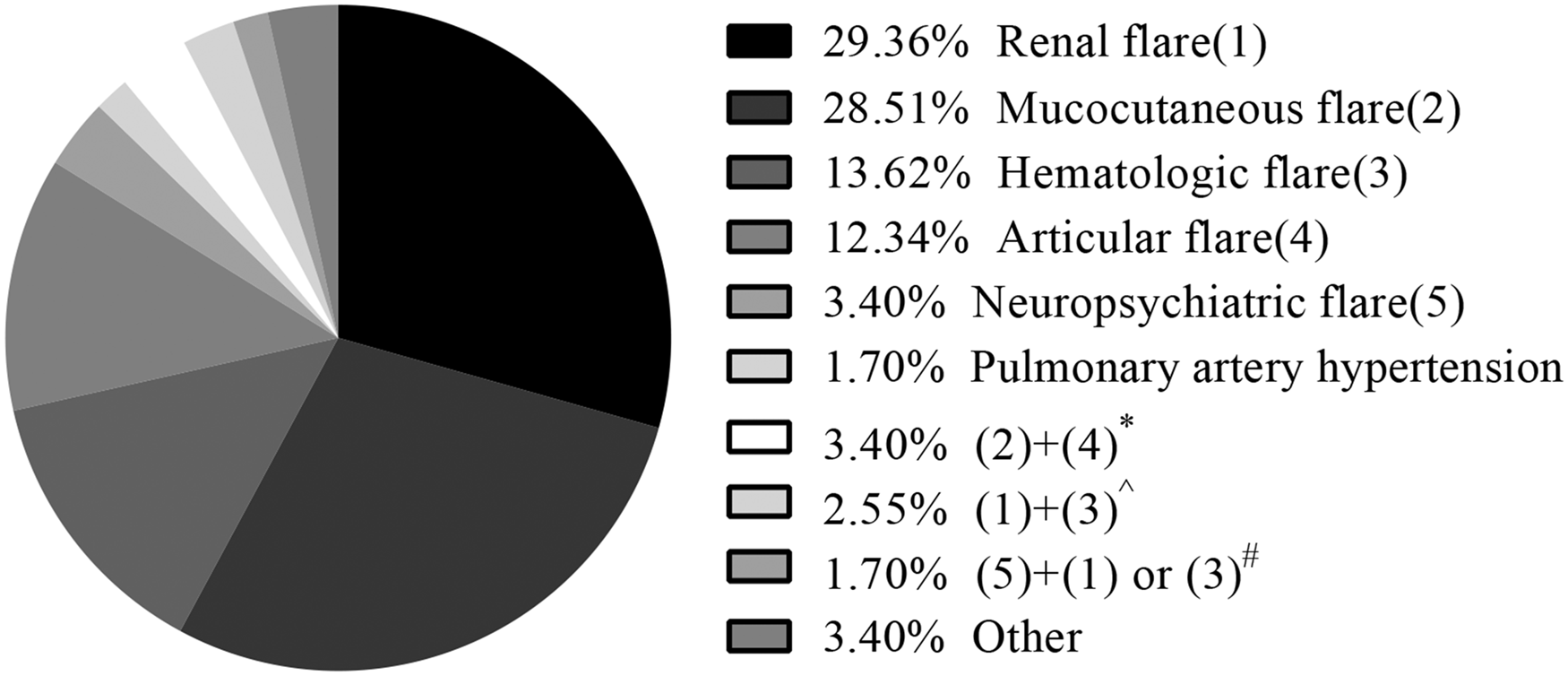
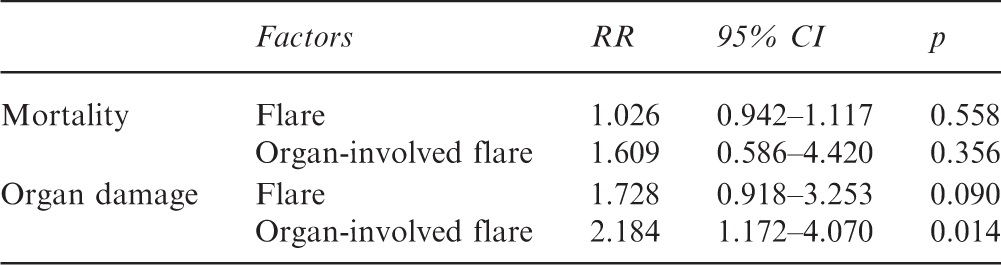
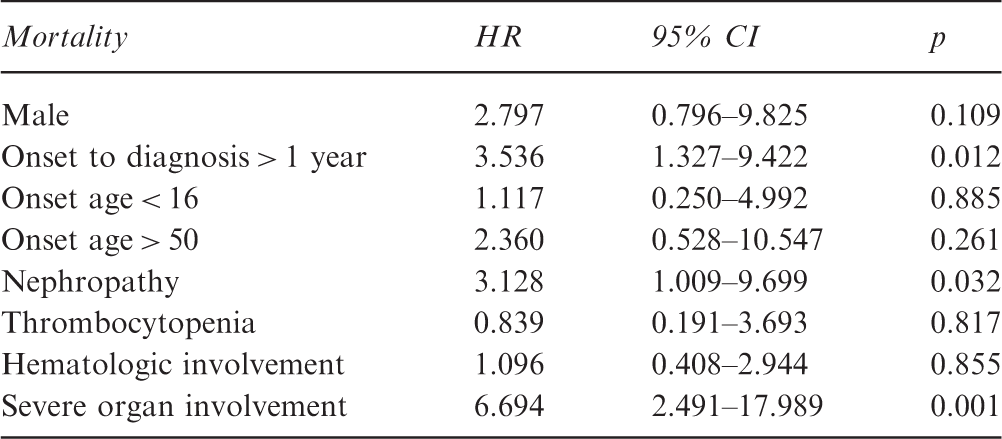
To study the relationship between organ damage, flare, and death, the KM method and Cox regression analysis were performed. KM curves were drawn, showing that the survival rate of patients with baseline damage was lower than those without damage at entry (Figure 3). After controlling for the influence of disease duration at entry, it showed that organ damage at baseline gave rise to higher mortality (HR 4.299, 95% CI 1.466–12.606, p = 0.008). Flare was not a direct predictor for either death (relative risk (RR) 1.026, 95% CI 0.942–1.117, p = 0.558) or organ damage (RR 1.728, 95% CI 0.918–3.253, p = 0.090). However, organ-involved flare during follow-up led to higher probability of new damage (RR 2.184, 95% CI 1.172–4.070, p = 0.014), though we did not find it to be a risk factor for mortality (RR 1.609, 95% CI 0.586–4.420, p = 0.356) (Tables 1 and 2).
Kaplan–Meier survival curves for patients with/without baseline damage. SDI: Systemic Lupus International Collaborating/American College of Rheumatology Damage Index. Cox regression analysis of flare for mortality and organ damage RR: relative risk; CI: confidence interval. Cox regression analysis for mortality. HR: hazard ratio; CI: confidence interval.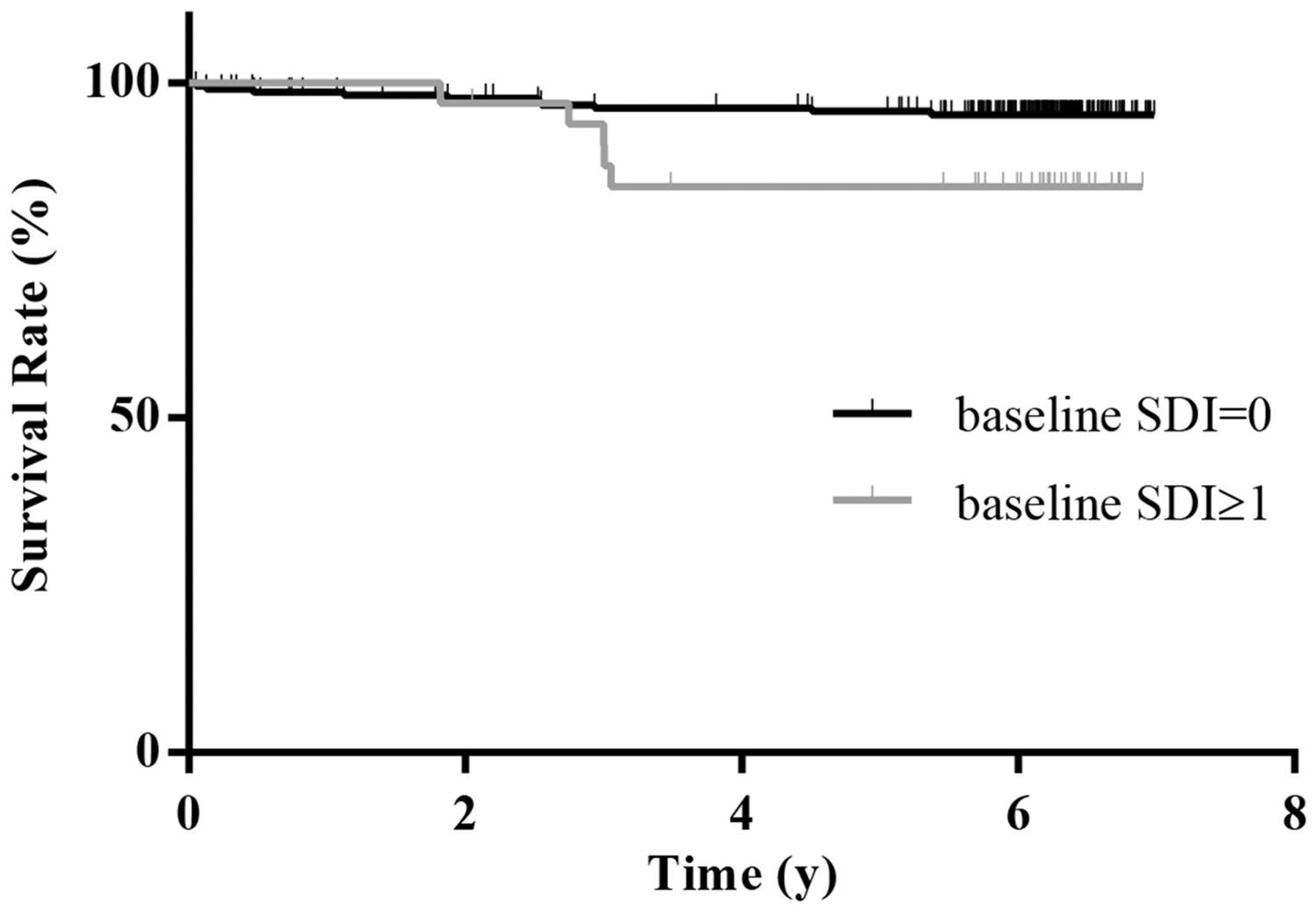
Prediction of death and organ damage
Cox regression analysis for organ damage
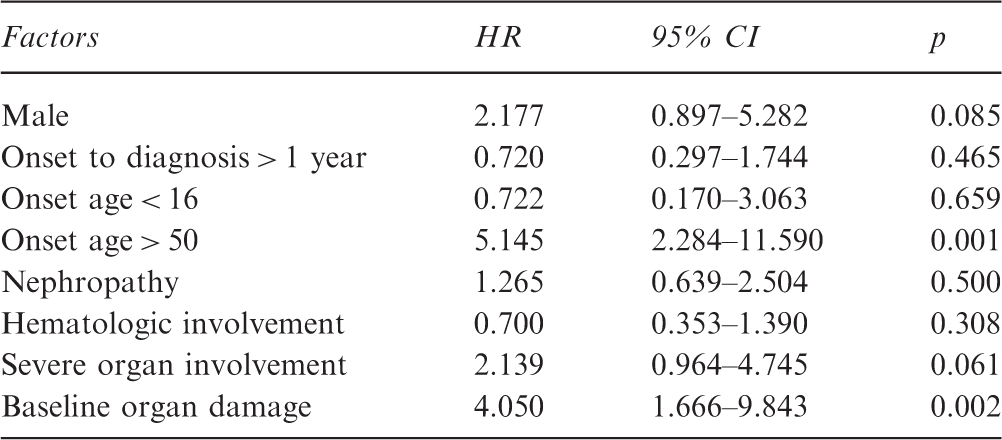
HR: hazard ratio; CI: confidence interval.
Discussion
In survival analysis, the five-year survival rate was similar to the result of our previous meta-analysis for Chinese SLE patients, as well as the major causes of deaths. We found several independent predicting factors for mortality, including late diagnosis from disease onset, organ damage, and severe organ involvement. Early diagnosis was thus still important for Chinese SLE patients and we need to keep strengthening the awareness of early identification of SLE patients in China. Former studies have proposed that irreversible organ damage causes more deaths in Caucasian SLE patients. 17 Our study confirmed that organ damage also predicts higher mortality and it can be a potential treating target for Chinese SLE patients. In the past, several specified and rare organ-involved subtypes of SLE, which we call severe organ involvement in our study, were reported to have worse prognosis, including NPSLE, GI, PAH, and ILD.13,14,18,19 In our study, we found that patients who had these organs affected resulted in more deaths. Therefore, preventing severe organ involvement should be another potential target for SLE treatment in China and deserves more attention in future clinical practice.
For organ damage accrual, compared with the increasing proportions reviewed by Sutton et al. in a meta-analysis in 2013, the percentage increase in our study was relatively lower. 17 This could be the result of ethnic effect as demonstrated by Bruce et al. in 2015 that Asian SLE patients had lower rates of new damage, or the implication of improved prognosis because the reviewed studies were mostly completed before 2010. As for organ damage prediction, late onset age, previous damage, and organ-involved flares were shown to be independent factors that lead to more damage. Among them, the first two were in line with prior studies that were mostly conducted in the Caucasian SLE cohort. 20 In large studies, it was proposed that higher global disease activity was one of the main predictors for damage development, and the number of flares was associated with the presence of chronic damage and damage accrual.5,7,8 Our study further obtained that nonorgan-involved flares like mucocutaneous flares had little contribution to the accumulation of organ damage, and it might be the result of both milder damage caused by nonorgan-involved flares and less intensive treatment adjustment for these conditions.
Compared with a previous study by Nikpour et al., the major types of flares were similar. 21 In our study, renal, hematologic, and neuropsychiatric flares were the top three organ-involved flares, implying that we should focus on the detection, management, and prevention of these types of flares, thereby reducing further irreversible damage for Chinese SLE patients.
Previously, two case-control studies, from the Lupus in Minorities: Nature versus Nurture (LUMINA) and the Toronto group, have proposed that hydroxychloroquine (HCQ) use was significantly associated with less organ damage.22,23 However, in our study, 86% of the patients were treated with HCQ at baseline, making us unable to further study the potential influence of HCQ use on organ damage and mortality. As most of the patients were treated with HCQ in our study and because of the uncertain influence extent of HCQ on organ damage accrual, we neglected the potential impact of HCQ on organ damage this time.
Our study is a prospectively designed study with intact baseline data. However, the follow-up data were partially collected by retrospectively reviewing the clinical records and telephone interview. Therefore, clinical data might be incomplete for certain patients, especially in part of the study of flares. In future, we need more prospective studies to focus on the study of flares to further explore possible predicting factors and prevention strategies for flare and new damage, thus improving the long-term prognosis for Chinese SLE patients. Moreover, as our study is not an inception cohort study, we cannot avoid the influence of disease course at entry and may underestimate the long-term survival rates, and we need larger cohort and inception cohort studies to further verify our results in the future.
Conclusion
Long-term survival rates of Chinese SLE patients have improved greatly to be consistent with previously reported ones both for Chinese and Caucasians. Organ damage, severe organ involvement, and prolonged remission could be a treating target for management of Chinese SLE patients. Early diagnosis, paying more attention to severe organ involvement and preventing organ-involved flares and new organ damage will be crucially important and worth close attention in the management of Chinese SLE patients. Ultimately, the core concepts of T2T in SLE, including targeting remission and preventing organ damage, were applicable in the clinical practice for Chinese SLE patients, and we need to further seek possible strategies to reach these goals.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Chinese National High Technology Research and Development Program, Ministry of Science and Technology (2012AA02A513), and the Chinese National Key Technology R&D Program (2017YFC0907601, 2017YFC0907602, 2017YFC0907603), Ministry of Science and Technology (2008BAI59B02).