
Abstract
Aim
The aim of this study was to evaluate the clinical response to combined therapy with hydroxychloroquine and mepacrine in patients with systemic lupus erythematosus and refractory joint and/or skin disease.
Methods
Mepacrine was added to 46 systemic lupus erythematosus patients unresponsive to treatment with the following drug combinations: hydroxychloroquine + prednisone + immunosuppressive drugs (n = 24), hydroxychloroquine + prednisone (n = 16), hydroxychloroquine + prednisone + retinoids (n = 2), hydroxychloroquine alone (n = 1), hydroxychloroquine + one immunosuppressive drug (n = 1), hydroxychloroquine + prednisone + one immunosuppressive drug + belimumab (n = 1) or hydroxychloroquine + prednisone + belimumab (n = 1). The outcome variable was the clinical response, either complete or partial, based on clinical judgement. The Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) and the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) score were additionally used.
Results
A total of 91% patients showed complete/partial response, with similar rates among those with joint or skin disease. In patients with cutaneous activity, a statistically significant decrease in the CLASI was seen. There also was a statistically significant decrease in the SLEDAI. The mean daily dose of prednisone decreased from 5.8 to 3.4 mg/d (p = 0.001). Prednisone could be discontinued in 20% of patients. No serious adverse events were seen. Smoking was the only predictor of complete response.
Conclusion
In the setting of refractory skin and/or joint disease, the addition of mepacrine to previous therapy including hydroxychloroquine was safe and effective in reducing disease activity and decreasing prednisone doses. The fact that smokers responded better opens the door to further studying the combination of mepacrine–hydroxychloroquine as a first-line therapy in such patients.
Keywords
Introduction
Mepacrine (MC) (also known as atabrine or quinacrine) is an acridine derivate synthesized in the early 1930s as the first synthetic antimalarial drug. 1 At the time of World War II, MC was massively used to treat malaria in the Pacific front. In 1951, after the empirical observation of improvement of skin and joint manifestations in many US and British soldiers with rheumatic diseases, Page published his experience in treating 18 lupus patients with MC, most with limited cutaneous disease. Clinical response was observed in 17 of them, being described as good or excellent in 14. 2 In addition, MC has no significant potential for macular toxicity. 1 However, after the discovery of chloroquine (CQ) and hydroxychloroquine (HCQ), the use of MC in lupus almost vanished. 1
Almost two decades ago, Toubi et al. reported the efficacy and prednisone sparing effect of MC addition to six patients with active systemic lupus erythematosus (SLE) on HCQ. 3 However, there is a striking lack of data defining the actual role of this combination in SLE.
Over the last few years, we have increasingly used MC in lupus; first, in patients with contraindications to HCQ and, later, combined with HCQ in patients with non-major organ activity unresponsive to therapy. With this background, we aim to analyze the outcome of SLE patients with persistent skin and/or joint disease following the addition of MC to a previous regime containing HCQ.
Patients and methods
Study design and patients
We conducted a retrospective analysis of prospectively acquired data from the Hospital Universitario Cruces and Hospital Clínico San Cecilio longitudinal SLE cohorts, all fulfilling ACR or SLICC criteria.4,5 Patients with refractory skin and/or joint disease were included if they were treated with MC as an add-on therapy for cutaneous and/or articular lupus involvement unresponsive to treatment with HCQ, alone or combined with other drugs.
All patients had given informed consent. The institutional review boards of both participating centres approved the study in compliance with the Declaration of Helsinki.
Baseline variables of the study
The following variables were recorded: gender, age, disease duration, smoking status, organ involvement, autoantibody profile, hypocomplementemia and treatments received when MC was added to baseline therapy. According to the lack of control (no-mepacrine) group, all the authors evaluating response were aware of the treatment received by the patients.
End points
The main end point was clinical response: complete response (CR), partial response (PR) – more than 50% improvement of skin or articular involvement – or no response (NR), based on the clinical assessment of the attending physician. No tender/swollen joint count was used to evaluate articular response, which was assessed based on patients’ reported joint pain and physicians’ qualitative evaluation. Patients reporting persistent joint pain and/or morning stiffness were not considered to have achieved CR even in the absence of visible inflammation. In addition, the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) 6 was calculated at time 0 (t0, the time of MC prescription), 6 months (t6) and 12 months (t12). For patients with skin disease, the Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) was calculated at t0, t3, t6, t12 and tend.7,8 The reduction of the daily dose of prednisone was also analyzed and adverse events were recorded.
Statistical analysis
Descriptive data were generated, using percentages, means and standard deviations (SD) as appropriate. We calculated the proportion of responding patients (CR and CR/PR) in the whole cohort and according to indication (cutaneous, articular or both). In addition, CLASI scores at t3, t6, t12 and tend were compared with CLASI t0, and SLEDAI t6 and t12 were compared with SLEDAI t0 by paired student t-test.
In order to identify potential predictors of response, univariate binary logistic regressions were performed with CR and CR/PR as the dependent variables. Independent variables included age, gender, autoantibodies, hypocomplementemia, indication for MC, baseline SLEDAI, prednisone dose, treatment with methotrexate, azathioprine and mycophenolate and smoking status. Variables with a p ≤ 0.1 in the univariate analysis were candidate predictors for the multivariate logistic regression analysis.
All the calculations were made using SPSS 20.0 (SPSS Inc.).
Results
Baseline features
Baseline features
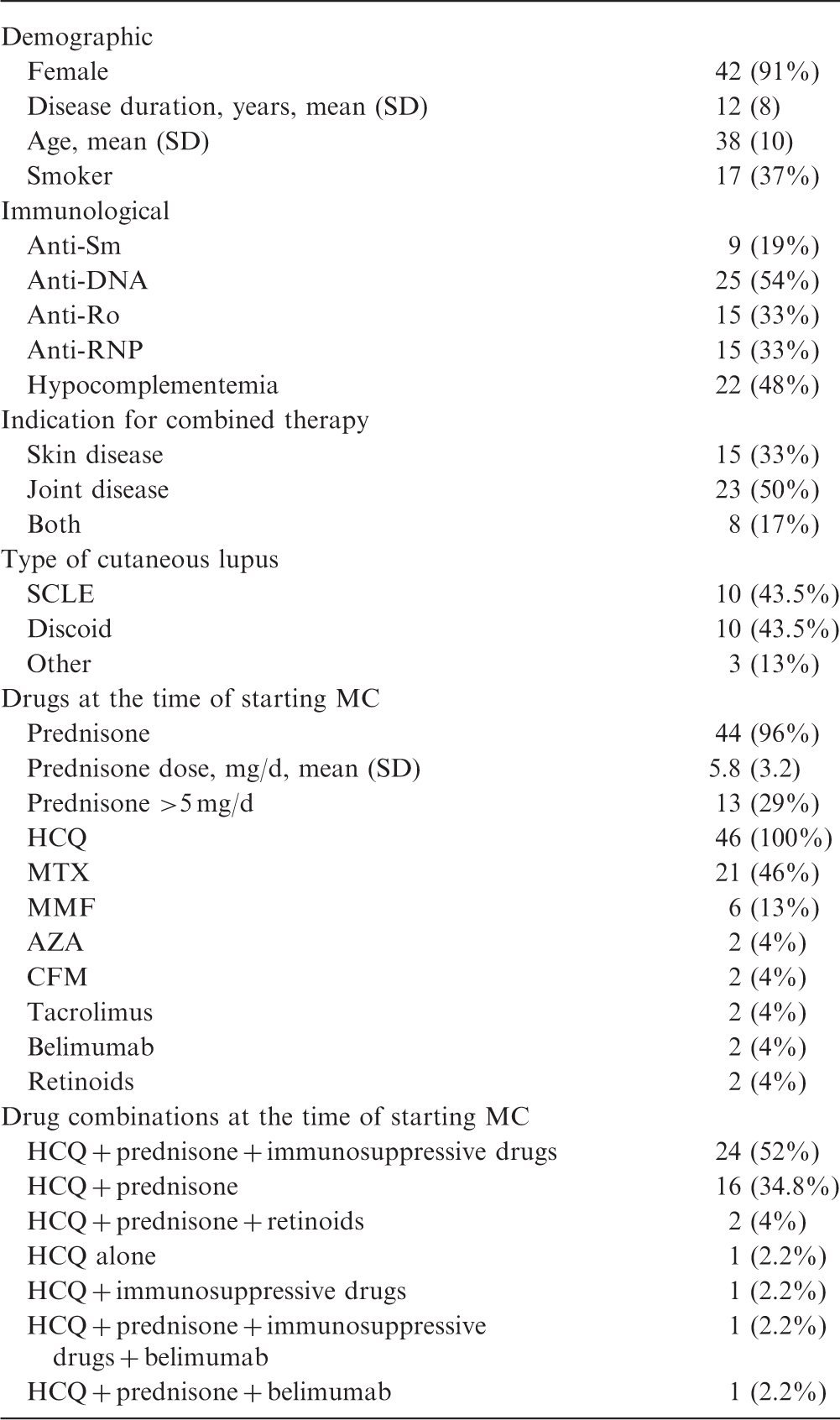
SD: standard deviation; SCLE: subacute cutaneous lupus erythematosus; MC: mepacrine; HCQ: hydroxychloroquine; MTX: methotrexate; MMF: mycophenolate mofetil; AZA: azathioprine; CFM: cyclophosphamide.
The initial dose of MC was 100 mg/d in 35 patients and 100 mg/48 h in 11 patients. As per protocol, all patients were on HCQ, with only one patient taking this in monotherapy. Forty-four (96%) were also taking prednisone (mean dose 5.8 mg/d), with 13 patients (29%) receiving doses >5 mg/d. Twenty-seven patients (59%) were taking at least one immunosuppressive drug. Additionally, two patients were receiving retinoids and two were on belimumab. Table 1 shows the combinations of drugs at t0.
Clinical response
The mean (SD) follow-up was 33 (32) months, with all patients completing at least 12 months of follow-up. The global rates of CR and CR/PR were 48% (22/46) and 91% (42/46), respectively. The rates of CR and CR/PR in articular activity among patients with only articular involvement were 43% (10/23) and 91% (21/23) respectively. In patients with only skin disease, 60% (9/15) and 87% (13/15), respectively, achieved CR and CR/PR in cutaneous manifestations. Among the eight patients with both cutaneous and articular activity, the rates of CR and CR/PR were 25% and 100%, respectively. In patients with skin disease (alone or in combination), the response rates were higher for the 10 patients with subacute cutaneous lupus erythematosus (SCLE) (CR 60%, CR/PR 100%) than for the 10 patients with discoid lupus (CR 30%, CR/PR 80%).
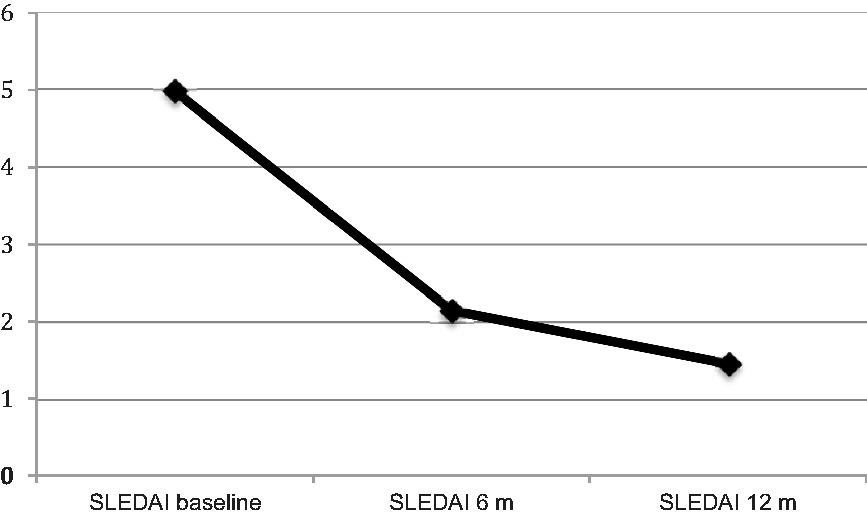
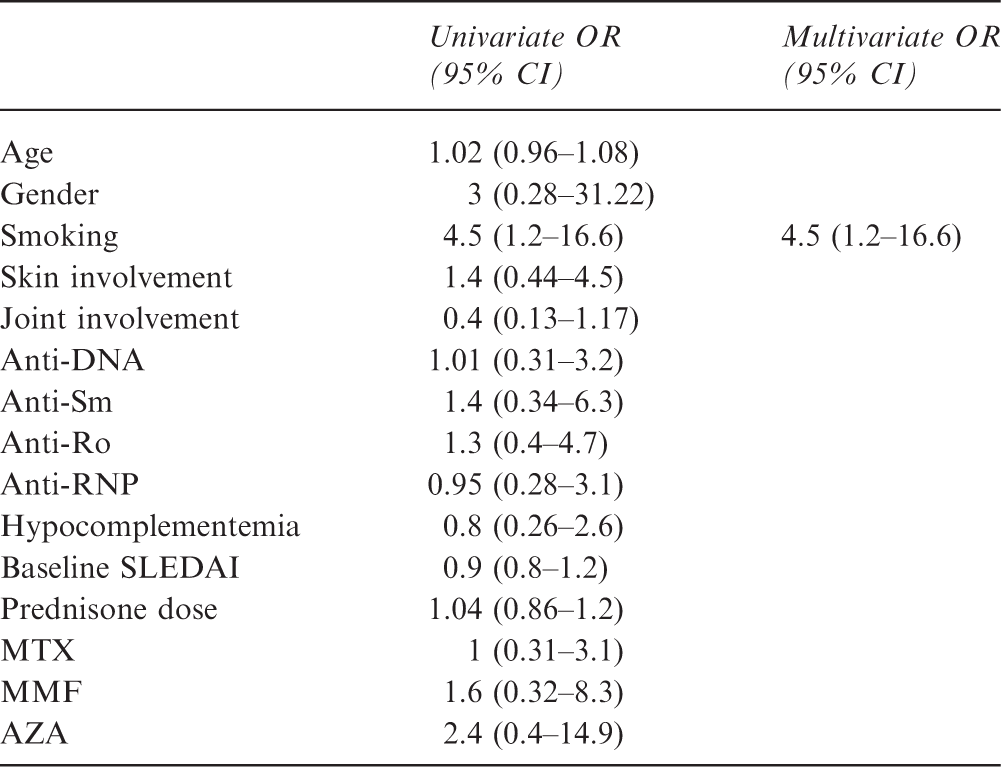
Consistently, the CLASI significantly improved at all the pre-specified points (see Figure 1): CLASI t0–CLASI t3 3.4 (95% confidence interval (CI) 1.5–5.3); CLASI t0–CLASI t6 5.8 (95% CI 2.3–9.3); CLASI t0–CLASI t12 6.1 (95% CI 2.2–10.1); CLASI t0–CLASI tend 6.5 (95% CI 2.9–10.1). There was also a significant reduction in the SLEDAI (see Figure 2): SLEDAI t0–SLEDAI t6 2.8 (95% CI 1.9–3.7); SLEDAI t0–SLEDAI t12 3.5 (95% CI 2.6–4.4). The “arthritis” item of the SLEDAI improved in 14/23 (60%) of patients with only articular activity; the “rash” item of the SLEDAI improved in 8/15 (53%) patients with only cutaneous activity; among the eight patients with both joint and skin activity, 50% improved the cutaneous item, 12.5% the articular item and 37% both. MC therapy favoured a significant decrease of the mean daily dose of prednisone from 5.8 mg/d at t0 to 3.4 mg/d at tend (p = 0.001). Accordingly, only two patients (4%) were on prednisone doses >5 mg/d (7.5 and 10 mg/d, respectively) at tend vs. 29% at t0 (p = 0.001). Prednisone was discontinued in 20% patients. In the logistic regression analysis, smoking was the only predictor of CR (Table 2). No predictors of CR/PR were identified.
Mean CLASI (Cutaneous Lupus Erythematosus Disease Area and Severity Index) scores over time. Mean SLEDAI (Systemic Lupus Erythematosus Disease Activity Index) scores over time. Logistic regression analysis (dependent variable, complete remission) MTX: methotrexate; MMF: mycophenolate mofetil; AZA: azathioprine; OR: odds ratio; CI: confidence interval.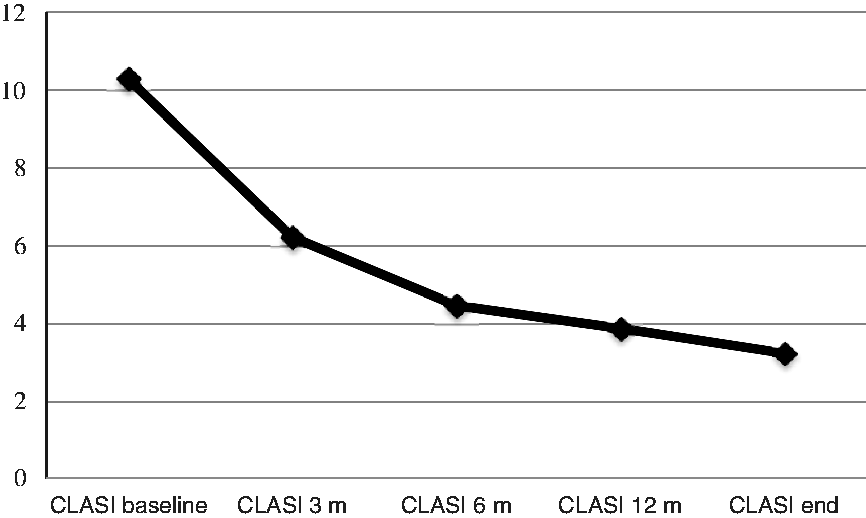
Safety
Three patients experienced adverse events (liver enzymes elevation, pruritus and dyspepsia), all of them mild and reversible upon drug withdrawal (two cases) or with reducing MC dose (one case). All patients followed the scheduled yearly retinal exams by skilled ophthalmologists, with no signs of antimalarial toxicity found in any of them during the course of the study.
Discussion
The earliest evidence on MC efficacy in lupus dates from the 1940s, with several studies showing beneficial results in about 70% of patients, mainly with skin or articular manifestations.1,2 Later, the observation of a synergistic effect of HCQ and MC led to the marketing of a US Food and Drug Administration (FDA)-approved pill containing HCQ, CQ and MC. 9 However, after its withdrawal in the early 1970s, 1 MC became almost an anecdotal drug for SLE.
In 2000, the study by Toubi et al. 3 reported the use of combined MC–HCQ treatment in six patients with active lupus and major organ involvement. All were under HCQ and prednisone, ranging from 15 to 30 mg/d, and two patients were also taking immunosuppressive drugs (one azathioprine and one methotrexate). The authors reported CR in five out of six patients and a steroid-sparing effect. Other authors reported good results for combined therapy with MC plus HCQ or CQ in patients with refractory cutaneous lupus.10–13 These studies put MC therapy for SLE in the spotlight again.
We have added MC to previous treatments, including HCQ in all cases, in patients with SLE and refractory skin and/or joint activity, with or without concomitant organ involvement. Globally, more than 90% of patients showed a significant clinical improvement after the addition of MC, 48% of them achieving CR, with similar response of cutaneous and articular activity. Considering the high frequency of immunosuppressive drugs at baseline, we believe that MC, as an add-on treatment, was helpful in controlling disease activity in a difficult clinical setting. As a result, a significant reduction of prednisone doses to <5 mg/d could be accomplished in all but two patients, with one in five patients discontinuing steroid therapy.
An interesting finding of this study is that active smoking was a predictor of CR to MC. The influence of smoking in the severity of cutaneous lupus and the reduced response of smokers to antimalarials has been consistently reported.14–16 Hydrocarbons contained in tobacco smoke can induce certain isoforms of P450-cytochrome (CYP), which could accelerate HCQ metabolism. However, HCQ and MC have different metabolic pathways: HCQ is mainly metabolized by CYP 2D6, 3A4, 3A5 and 2C8, whilst CYP 3A4/3A5 is the predominant isoform in MC metabolism. 17 Whether this differential enzymatic degradation could explain our findings is a matter for future studies. Anyhow, our results could open the door for a possible use of MC as a first-line antimalarial in smoking SLE patients with predominant cutaneous and/or articular symptoms.
Our study is limited by the retrospective analysis and the relatively limited sample size, although this is the largest series of combined MC–HCQ therapy in patients with SLE,3,10–13 coming from two well characterized longitudinal lupus cohorts. Although the evaluation of response was based on the clinicians’ judgement, the parallel significant reduction of both the CLASI and SLEDAI scores reinforces our results. The glucocorticoid-sparing effect was also relevant, with 96% patients being below the safe cutoff of 7.5 mg/d of prednisone at the end of the follow-up. 18 MC was added to the therapeutic regime at the attending physician’s discretion; thus, the baseline therapeutic combinations were heterogeneous. However, the combination of HCQ + prednisone + immunosuppressives was used in more than 50% patients, 2 patients were on belimumab and only one patient was with HCQ monotherapy.
In summary, the addition of MC to HCQ-containing regimes was effective in controlling disease activity and reducing prednisone doses, well tolerated and without serious adverse reactions. We believe that these results support the use of the combined antimalarial treatment, not only as a possible initial treatment for skin and/or joint disease but also in those patients with persistent symptoms despite intensive immunosuppressive therapy. Our results could also open the door for investigating the use of MC–HCQ as a first-line therapy in smoking SLE patients with predominant cutaneous and/or articular symptoms.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.