
Abstract
The effect of physical activity on the immune system is still poorly understood in cases of systemic lupus erythematosus (SLE). Therefore, our aim was to investigate differences in the serum levels of cytokines (IL-2, IL-5, IL-6, IL-8, IL-10 and TNF-α) and the numbers of CD11b + and CXCR2 + neutrophils and lymphocytes in women with SLE undergoing drug treatment, without (n = 9) or with (n = 5) 4 months of kinesiotherapy. Parameters related to functional capacity were also analyzed. In the case of the patients who were not submitted to kinesiotherapy, there were reductions in the levels of IL-5, IL-6 and IL-10, and an increase in the number of CD11b + leukocytes, in addition to an increase in abdominal circumference after the monitoring time. Patients submitted to kinesiotherapy did not present changes in serum cytokines or in the numbers of CD11b + and CXCR2 + neutrophils and lymphocytes, but there were increases of flexibility and strength, as well as a reduction in pain sensation after the monitoring time. In conclusion, kinesiotherapy was able to increase flexibility and reduce pain in SLE patients without influencing immune parameters.
Keywords
Introduction
In systemic lupus erythematosus (SLE), the joint, renal, central nervous and cardiopulmonary systems are usually compromised, and systemic manifestations can trigger symptoms such as fatigue, malaise, fever, nausea, anorexia and weight loss, 1 consequently reducing quality of life and, in some cases, leading to death. The most common cause of mortality is cardiovascular disease, followed by infections associated with SLE. In addition, advances in treatment are not able to prevent deaths associated with comorbidities. 2
Patients under treatment for SLE present increased levels of cytokines such as IL-2, IL-6, IL-10 and chemokine CXCL8 (IL-8), 3 but even with the increase of these cytokines, there are reductions in leukocyte function as well as phagocytosis, mainly due to the effects of glucocorticoids (monocytes and neutrophils) associated with bacterial infections, morbidity and mortality.4,5
In both patients with autoimmune diseases and healthy people, a relationship has been found between the practice of aerobic resistance exercises and acute and chronic changes in the immune response, with improvements in terms of symptoms, morbidity and the side effects of drug treatment. Some of these changes are triggered by physiological adaptations related to the inflammatory response, 6 autonomic and cardiorespiratory responses, 7 and serum cytokines. 8 Aerobic training programs have been linked with immunomodulatory effects such as the reduction of circulating levels of TNF-α, IL-6 and IL-10 in patients treated for SLE, with the levels becoming closer to those of normal controls. 9 Supervised physical training has been shown to be effective in increasing aerobic capacity in groups of patients with SLE. 10
Moderate- or low-intensity physical exercise is considered a safe and effective adjuvant treatment for improving morbidity and quality of life in SLE patients. 11 There are various types of physical exercise protocols, but only a limited number of studies have involved continuous and progressive exercise protocols practiced for more than 12 weeks, or have investigated the consequences of this practice in patients with SLE under drug treatment. 12
The objective of the present study was to check parameters related to functional capacity, quality of life and serum levels of immune system markers in SLE patients under drug treatment, at the beginning and end of a 4 month monitoring time, in order to determine the consequences of a physical exercise protocol (kinesiotherapy) in terms of disease activity, SLE-related cytokines, and other components related to the innate and adaptive immune responses.
Materials and methods
Recruitment of patients and procedures
This was a prospective, analytical, uncontrolled, longitudinal experimental study. We evaluated 14 women diagnosed with SLE, following the guidelines established by the American College of Rheumatology, 13 at the Rheumatology Clinic of the Federal University of Triângulo Mineiro (UFTM), without considering the severity of the disease or the duration of treatment. The patients were divided into two groups, based on the willingness of the individuals to engage in the proposed activities. The first group (n = 9) consisted of women with SLE, under drug treatment, who were not submitted to any type of regular physical activity during the monitoring time. The second group (n = 5) comprised women with SLE, under drug treatment, who underwent intervention with a kinesiotherapy protocol during the monitoring time.
All the subjects included in this study were submitted to functional and disease severity evaluation, using the SLE disease activity index (SLEDAI). In addition, peripheral blood (serum and plasma) samples were collected for determination of cytokines, phagocytosis index (PI), and counts of CD11b + and CXCR2 + neutrophils and lymphocytes. Paired comparisons of the data at the start and end of the monitoring time were performed for each group. The patients were included in the study after explaining the work and obtaining written informed consent. The study was approved by the research ethics committee of UFTM (protocol number 1746). The assessments before and after the kinesiotherapy exercise protocol were always performed by the same evaluator.
Functional capacity evaluation
Functional capacity was determined using evaluation of posture, anthropometry, quality of life, strength, flexibility, walking and balance.
For classical postural evaluation, a posture chart was used, with simultaneous analysis by two evaluators to investigate possible alterations that could influence the execution of the tests and the proposed activities. 14
The anthropometric measurements included height (using a Micheletti stadiometer), body mass (using a G-Tech, model Glass 3 FWB weighing machine) and skin folds of the right body side (tricipital, subscapular, axillary, thoracic, suprailiac, abdominal and thigh, using a CESCORF adipometer). Body circumferences were measured using a tape measure and included abdominal, hip, thoracic, right and left thighs, right and left legs, and right and left arms. For adipometry and analysis of body circumferences, three measurements were performed at each site, with calculation of the arithmetic mean.15,16 The percentage of body fat was calculated using Physical Test® software in order to analyze the gain or loss after the exercise program.
Quality of life was assessed by means of the Medical Outcomes Study 36 questionnaire (SF-36 short health survey form), with transformation of the raw scores into quantitative values. 17
Walking and balance tests were performed using the Tinetti gait and balance evaluation test, for the detection of risk factors for falls. In this test, the maximum total quantitative score is 28 points, with values below 19 points and between 19 and 24 points indicating high and moderate risk of falls, respectively.18,19
Flexibility tests were performed using a Sanny fleximeter to determine the retraction of the upper and lower fibers of the pectoralis major muscle, with the results being expressed in degrees (°). 20 The sit-and-reach test with the door closed (Wells test) was used to quantify the flexibility of the posterior limb chain of the lower limbs, with the results being expressed in centimeters (cm). 21
Muscular strength was evaluated by the 10 maximal repetitions test (10 RM). The muscular strength of the upper limbs was assessed using a bench press (employing barbell plates, with the patient in dorsal decubitus). The muscular strength of the lower limbs was assessed by knees extension and flexion (using leg extension and lying leg curl machines). After 5 min of familiarization with the movements, the patient was instructed to raise a maximum weight, according to her own perception. A verbal command was given to perform the first movement, after which the repetitions were performed without verbal stimuli.22,23
Blood collection and determination of cytokine levels, PI, and numbers of CD11b + and CXCR2 + neutrophils and lymphocytes
Sera were obtained by centrifugation (180 × g, 15 min) of peripheral venous blood samples collected at the beginning of the study and after monitoring time (4 months). The samples were obtained prior to any physical exercise test.
Serum levels of TNF-α, IL-2, IL-5, IL-6, IL-8 and IL-10 were determined by ELISA, following the manufacturer's recommendations (OPD, Sigma, St. Louis, MO). The data were expressed in picograms of cytokine per milliliter of serum (pg ml−1).
Evaluation of the PI of neutrophils (at 2 × 106 ml−1) was performed considering the ability to phagocytize opsonized zymosan with human plasma (10 particles/cell) over a period of 1 h at 37 ℃ (under 5% CO2). The PI was obtained considering the percentage of phagocytic cells and the number of internalized particles.
The numbers of CD11b + and CXCR2 + neutrophils and lymphocytes were quantified using a FACSCalibur flow cytometer and CellQuest™ software (Becton Dickinson, San Jose, CA), with acquisition of 10,000 cells in each experiment. Phycoerythrin (PE)-conjugated anti-CD11b antibody, PE/Cy5-conjugated anti-CXCR2 antibody (BD Pharmingen, San Diego, CA) and control antibodies (PE- or PECy-5-conjugated IgG2b; BD Pharmingen) were used. Neutrophils and lymphocytes were separated by size (Forward Scatter-FSC) and granularity (Side-Scattered light-SSC). Data are expressed as the absolute number or the percentage of neutrophils and lymphocytes positive for CD11b and/or CXCR2 expression.
Kinesiotherapy program
The kinesiotherapeutic intervention was performed over a period of 4 months, three times a week, with each patient being attended individually by the same physiotherapist, in sessions lasting 50 min. The activities were divided into warm-up, strengthening and stretching.
The warm-up consisted of active movement and self-stretching of the upper limbs, trunk and lower limbs, performed for 5 min in an orthostatic position. The muscular strength training of the upper and lower limbs consisted of resistance exercises with barbell plates and dumbbells, with voluntary ventilation, performed in three sets of 10 repetitions, with a load of 70%; according to the 10 RM test there were increases of between 2 and 10% of the maximum current load, for one or two additional repetitions. Stretching in the final minutes consisted of passive stretching of the posterior chain of the lower limbs with the patient in dorsal decubitus, neck stretching with the patient seated, and stretching of the upper limbs also with the patient seated. Each movement was performed three times and was maintained for 30 seconds.
The aerobic training was added after the first month and consisted of 10 min on a stationary electromagnetic bicycle with the load regulated as desired by the patient. The patient was instructed to maintain 60 rotations per minute and the load could be intensified every 3 min, without the goal of increasing performance in this exercise, but increases of from 5 to 10%, in terms of time and load, were made whenever possible, depending on the willingness of the patient.
In all the resistance and ergometric exercises, the load increases were based on the training strategies suggested by the American College of Sports Medicine24,25 and by the SLE Consensus. 26
Disease activity index
The revised SLEDAI questionnaire, also known as SLEDAI-2K, was applied by medical professionals of the Rheumatology Department of UFTM. The questionnaire score ranges from 0 to 105 and includes 24 items (16 clinical and 8 laboratory). The scores are evaluated as follows: <2, inactive disease; 2–12, moderate-severity disease; >12, severe illness. 28 The questionnaire was applied and evaluated at the time of inclusion in the study and at the end of the monitoring time, for both patient groups.
Statistical analysis
SigmaStat 2.03 software was used for statistical analysis. The normality of the data was evaluated by the Kolmogorov–Smirnov test and the distribution of the variables was determined by the F-test, using the results obtained before and after the monitoring time, for each group. Differences between the two groups were evaluated using the paired t-test or the Wilcoxon test, for normally and non-normally distributed data, respectively. Statistical significance was considered for p ≤ 0.05.
Results
Participants
Clinical findings of the non-submitted and submitted patients to kinesiotherapy before and after monitoring time

Data expressed as median (25–75%) or mean ( ± SD). Mann–Whitney test.
SD: standard deviation; SLEDAI: systemic lupus erythematosus disease activity index.
At the start of the trial, no significant differences were found between the two patient groups in the initial SLEDAI evaluation (p = 0.888; Mann–Whitney test) or for any of the other clinical parameters (Table 1).
Comparison of the functional capacities of the groups with and without kinesiotherapy treatment
Strength and flexibility test values of the non-submitted and submitted patients to kinesiotherapy, before and after monitoring time
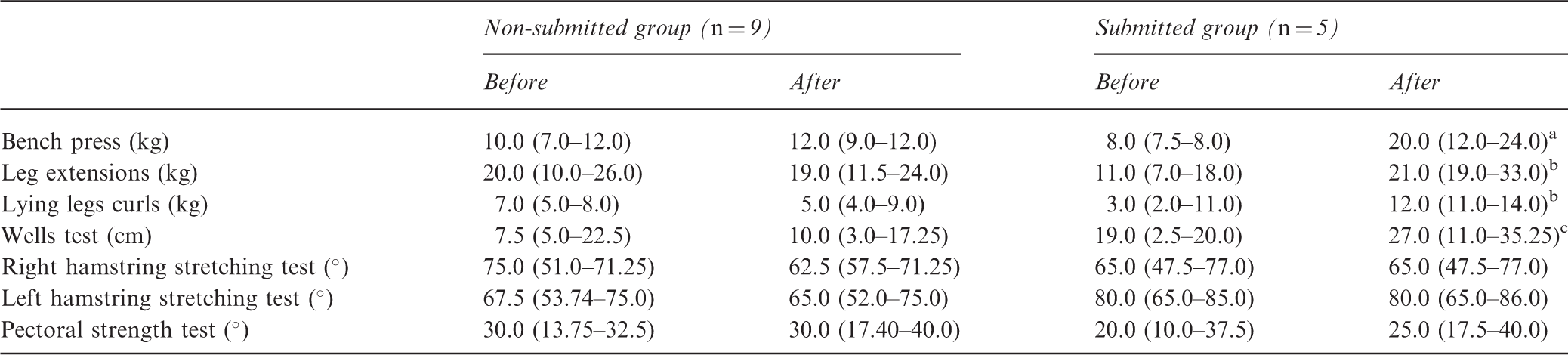
Data are expressed as medians and interquartile ranges (25–75%, Wilcoxon test).
p = 0.068.
p = 0.062.
p < 0.001.
Values of the items evaluated by the Medical Outcomes Study 36 questionnaire for non-submitted and submitted patients to kinesiotherapy before and after monitoring time
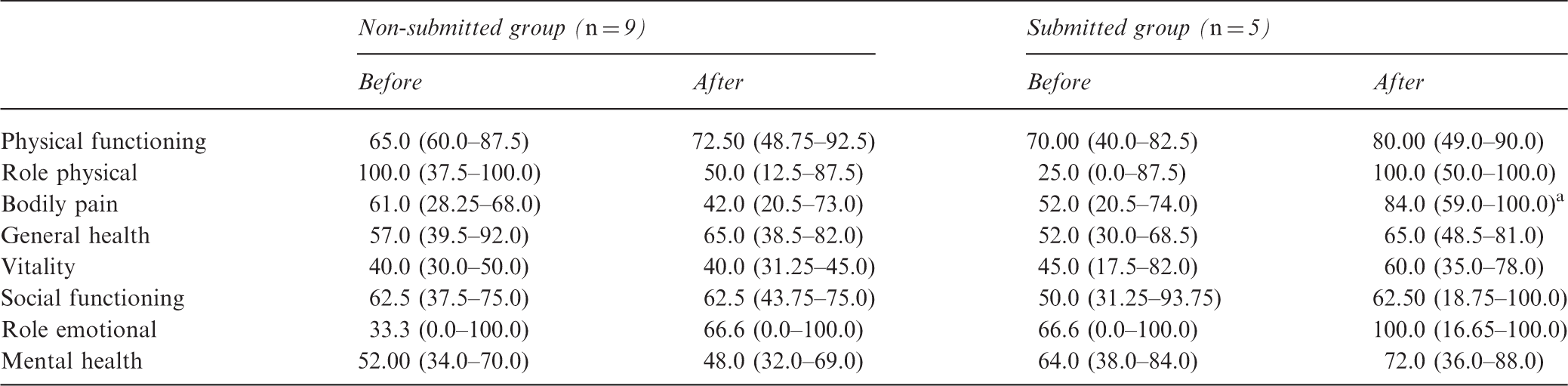
Data are expressed as medians and interquartile ranges (25–75%).
p = 0.02, t-test.
At the end of the monitoring time, the results of the muscle strength tests revealed no statistically significant differences between the groups. Nonetheless, the kinesiotherapy group showed an improvement of 57.6% in the supine muscle strength test, while an increase of only 16.98% was obtained for the non-kinesiotherapy group. In the leg extensor test, muscular strength increased by 48.8% in the group submitted to kinesiotherapy, while the non-kinesiotherapy group showed an increase of only 5.3%. In the lying legs curl test, muscle strength increased by 49.12% in the kinesiotherapy group, but by only 12.3% in the non-kinesiotherapy group. The results of the strength and flexibility tests conducted at the start and end of the monitoring time are presented in Table 2.
The non-kinesiotherapy group showed a significant increase in abdominal circumference (p = 0.039; Wilcoxon test) at the end of the monitoring time. No statistically significant changes were observed in the other anthropometric parameters (Supplementary Table 1).
In the SF-36 evaluation, there was no statistically significant difference between the groups at the start of monitoring time. At the end of the monitoring period, the kinesiotherapy group showed improvements for most of the parameters evaluated, although only bodily pain presented a statistically significant difference (p = 0.02; Wilcoxon test; Table 3). The group submitted to kinesiotherapy initially presented an index value of 52 on the SF-36 scale for the bodily pain parameter. After 4 months, an index value of 85 was obtained for this group, reflecting an improvement in terms of pain sensation.
Comparison of cytokine levels and numbers of circulating cells in the kinesiotherapy and non-kinesiotherapy groups
Serum cytokine levels of the non-submitted and submitted patients to kinesiotherapy before and after the monitoring time
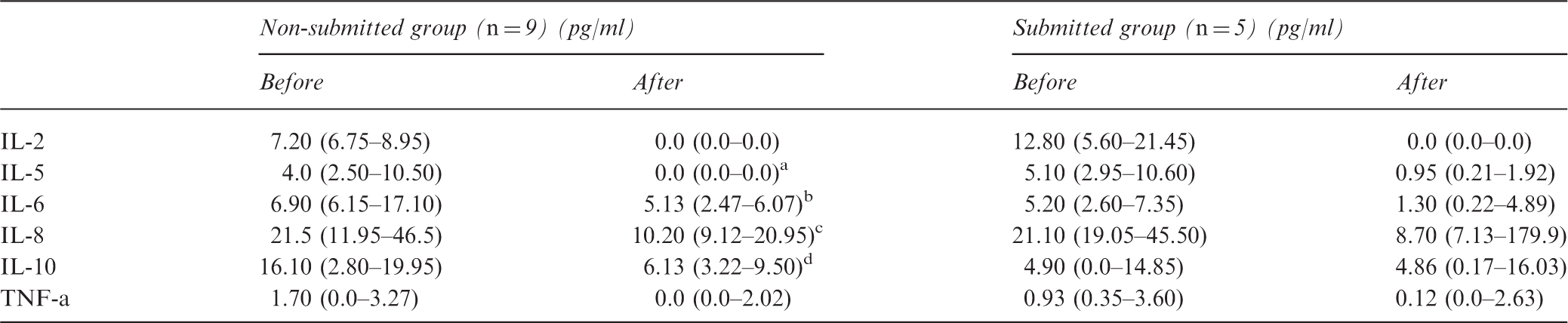
Data are expressed as medians and interquartile ranges (25–75%, Wilcoxon test).
p = 0.003.
p = 0.007.
p = 0.054.
p = 0.034.
Additionally, after 4 months, in the non-kinesiotherapy group, there were increases in the percentage and absolute number of CD11b + lymphocytes at the end of the period (Figure 2(c) and (d)), which was not detected in the kinesiotherapy group. The CD11b + circulating neutrophils did not present alterations regarding their serum number in both groups in the evaluated period (Figure 2(a) and (b)). Neither of the patient groups showed any changes in CXCR2 + neutrophils or lymphocytes levels (data not shown).
Time line of monitoring and intervention description for pharmacological therapy and pharmacological therapy + kinesiotherapy groups. The longitudinal line represents the elapsed time. The vertical lines represent the months of monitoring and respective interventions.
No significant differences were observed in the PI values before and after the monitoring time, for either group (Wilcoxon test, p = 0.125). However, the percentage analysis indicated increased phagocytosis in kinesiotherapy patients after the monitoring time. The kinesiotherapy group presented an increase of 90.92% in the median PI value, while the non-kinesiotherapy group showed a reduction of 63.26%.
(a) to (d) Graphs represent the percentage and absolute values of circulating CD11b + neutrophils and lymphocytes in systemic lupus erythematosus non-submitted and submitted patients to kinesiotherapy before and after the monitoring time. The horizontal lines represent the medians and 25 and 75% percentiles. Graphics (c) and (d); *p = 0.03 (Wilcoxon test).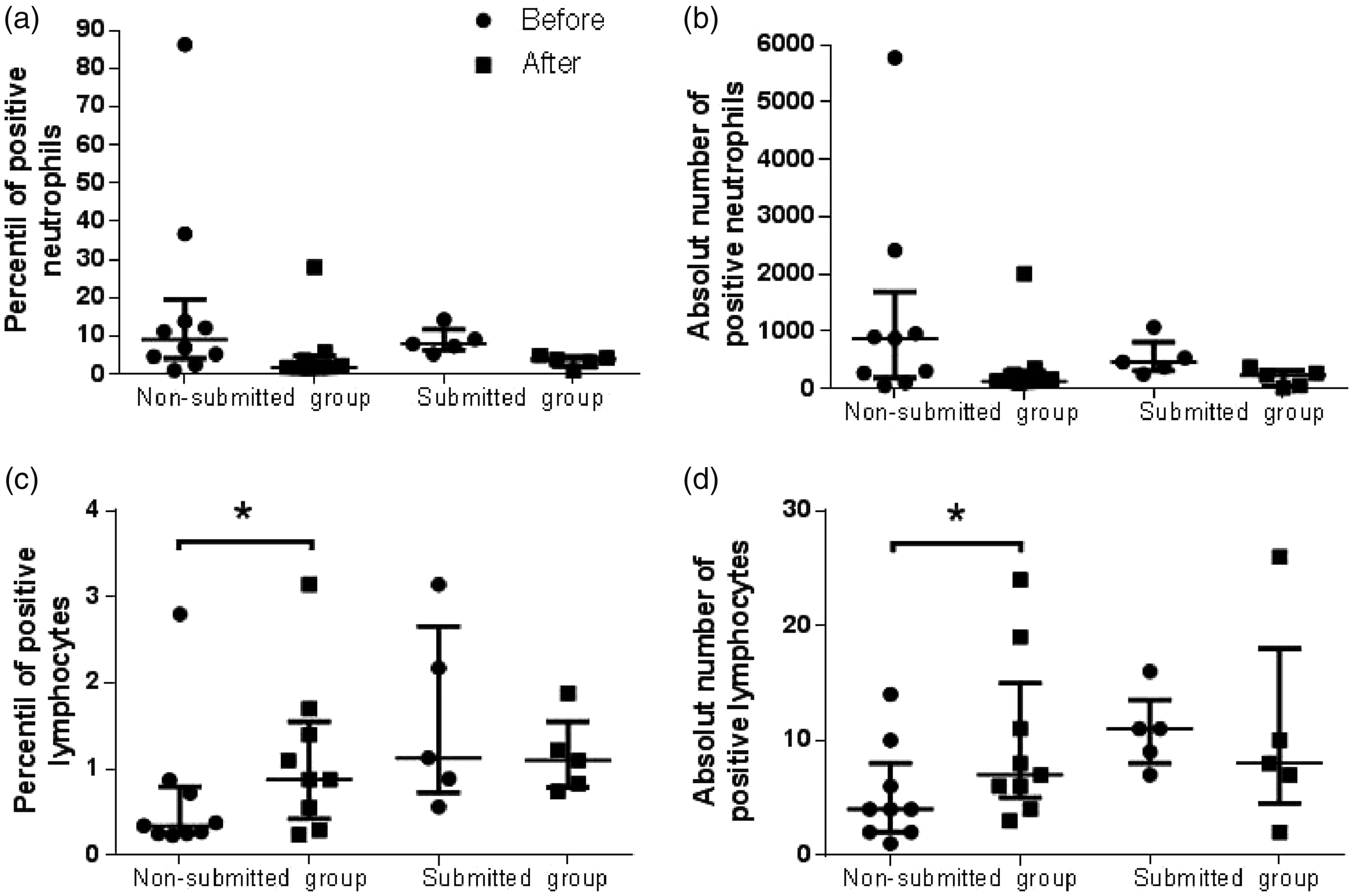
Discussion
Functional capacity is a broad term that involves physical and psychological abilities, and can be evaluated in different ways. 16 In the present work, the functional parameters considered were quality of life, body balance, walking capacity, flexibility and strength, obtained in the form of numerical data.
Previous collection was made of personal data, information about current and previous diseases, and the location and intensity of pain. These data allowed the grouping of individuals with the same clinical manifestations. Consequently, despite the limited number of patients, the two groups of women with SLE could be considered homogeneous in terms of clinical parameters, functional capacity and SLEDAI.
The practice of physical exercise plays an important role in the rehabilitation of patients with SLE, notably for the prevention and/or treatment of cardiovascular disorders related to a sedentary lifestyle and the adverse effects of drug treatment.11,12 However, few studies have shown the effects of a training period on the levels of cytokines and/or immune cell receptors in patients with SLE, 8 and no previous studies have linked the serum parameters evaluated in this work to the effects of kinesiotherapy on the immune systems of individuals with this disease. Therefore, this work was based on previous studies of immune response patients that have reported that in SLE, the immune response is characterized by hyperactivity of B lymphocytes and imbalanced production of cytokines including TNF-α, IL-2, IL-6 and IL-10,3,27–35 considering the importance of clinical aspects of the disease in a remission period and the type of treatment.
In previous work by our group, increased levels of circulation IL-6 and IL-10 were observed in patients in remission and undergoing treatment, compared to controls without the disease. 29 In the present work, all the patients had reductions in IL-6 and IL-10 but these were only significant in the non-kinesiotherapy group. This showed that immunosuppressive therapy was effective in reducing the levels of disease markers. But the role of IL-10 in autoimmune diseases is controversial. Expression of this cytokine is associated with the anti-inflammatory and immunosuppressive response,20,31 but it is overexpressed in patients with lupus and has been reported as a molecule that promotes the disease, although there is no real evidence of its role.32,36 IL-10 can act in the inhibition of IL-1b, inhibition of eicosanoid production and targeting for the regulatory T cell response; 32 therefore, although these studies evidenced a disease improvement, they did not assess the sensation of pain in patients. The maintenance of this cytokine during treatment, even in patients in the non-active phase of the disease, may be a factor that favors stability in general inflammatory reactions, including sensation of pain.33–36 In this study, no correlation was found between IL-10 levels and bodily pain (Spearman test, data not shown). However, the possible maintenance of IL-10 as a mechanism of analgesia cannot be disregarded.
Other aspects related to pain in SLE patients seen in this study are flexibility and strength. In SLE patients, bodily pain may be associated with primary fibromyalgia, 37 muscle fatigue, 38 and/or changes in physical and mental aspects,39,40 so the improvements in flexibility and strength in the kinesiotherapy group probably influenced not only pain reduction, but also the other aspects related to quality of life evaluated by the SF-36 test. The lack of significance of the improvements in the SF-36 scores and in the strength tests was due to the small number of patients in this study. Clinical evidence has been reported for anti-inflammatory effects of stretching exercises, and they have been found to be as effective as mefenamic acid in the treatment of primary dysmenorrhea, 41 although no studies have related these effects to IL-10.
The function of CD11b in cell migration and protein binding is still unclear and it has contradictory functions in SLE. Studies indicate that genetic alterations resulting in the deficiency of CD11b may be an important mechanism for the onset of the disease, with increased levels of interferon-I in animal models and in patients with SLE42,43 resulting in a failure to downregulate IL-6 expression in macrophages, 44 but it this corroborates a deficiency in mediating phagocytosis and cell recruitment. 45 Therefore, it is possible that some mechanisms are involved with changes in CD11b for disease, 46 but it is still not possible to relate any benefits related to a rise in the number of CD11b + lymphocytes, as observed in our previous study 28 and in this study. Despite the increase in CD11b + lymphocytes occurring in the non-kinesiotherapy group, the phagocytosis appears to have increased in the kinesiotherapy group. This would represent a positive result of the kinesiotherapy, with improvement of innate immunity. Therefore, further studies should be performed with a greater number of patients.
The CXCR2 receptor for chemokines CXCL1-3 and CXCL5-8 is quite non-specific and is mainly expressed on the lymphocyte surface, participating in activation of the cell migration process, with proinflammatory roles in the recruitment of neutrophils, monocytes and macrophages to sites of infection. 47 This chemokine receptor also has unique functions in the promotion of IL-8-mediated angiogenesis in cancer. 48 The absence of changes in the numbers of neutrophils and circulating CXCR2 + lymphocytes during the follow-up period, for both groups, could indicate that this receptor is not associated with the disease during its inactive phase, as we have seen in an earlier study, in contrast to the active disease period. 28
Additional studies of the various physical exercise protocols applied to individuals with autoimmune diseases should aim to improve the techniques, for the purposes of rehabilitation and the reestablishment of quality of life. This study presents only a small number of the immunological parameters that should be evaluated for physical activity in patients with SLE and other aspects that should be considered as endocrine responses. 49
This rehabilitation technique could be effective in improving the quality of life and functional aspects of individuals suffering from other autoimmune diseases, 50 and the present findings could substantiate, for the first time, that kinesiotherapy is an immunologically safe treatment; however, it should be applied to a larger number of patients in order to confirm the relationship between the immune response and reduction of pain.
Conclusions
The kinesiotherapy protocol employed in this work was safe and effective in increasing flexibility and reducing pain sensation, when applied to a limited number of patients with SLE, under drug treatment, during the inactive phase of the disease. Kinesiotherapy resulted in the maintenance of serum levels of IL-10 and the number of circulating CD11b + lymphocytes, which was considered beneficial for patients with SLE who underwent the proposed therapy.
Supplemental Material
Supplementary Table 1 -Supplemental material for Increased flexibility, pain reduction and unaltered levels of IL-10 and CD11b + lymphocytes in patients with systemic lupus erythematosus were associated with kinesiotherapy
Supplemental material, Supplementary Table 1 for Increased flexibility, pain reduction and unaltered levels of IL-10 and CD11b + lymphocytes in patients with systemic lupus erythematosus were associated with kinesiotherapy by R Pessato Timóteo, A Ferreira Silva, D Côbo Micheli, E F Candido Murta, M Freire, R Botelho Teodoro, F M Lima, B Martins Tavares Murta and D Bertoncello in Lupus
Footnotes
Acknowledgements
We especially thank the patients who participated in the study. We also thank all the professionals of the Rheumatology discipline at Universidade Federal do Triângulo Mineiro for supporting this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial report for the research, authorship and/or publication of this article: the Financiadora de Estudos e Projetos (grant number 1086/06), Fundacão de Amparo à Pesquisa do Estado de Minas Gerais (grant number 52-11), Conselho Nacional de Desenvolvimento Científico e Tecnológico (grant number 507783/2010-7) and Fundacão de Ensino e Pesquisa de Uberaba (grant number 578/2008).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.