
Abstract
Objective
The European League Against Rheumatism and the American College of Rheumatology jointly embarked on a new classification criteria for systemic lupus erythematosus (SLE) project. Its first phase involved generation of a broad set of items potentially useful for classification of SLE. This study was undertaken to add the patient perspective to an expert Delphi approach and an early patient cohort study.
Methods
A national cross-sectional study was conducted. A self-report questionnaire was published in the “Schmetterling” (Butterfly), the quarterly journal of the German SLE patient association. Individuals with SLE were asked to anonymously complete the questionnaire, which asked for demographic details, organ manifestations, autoantibodies and symptoms.
Results
A total of 339 completed questionnaires out of 2498 were returned, a response rate of 13.6%; 83.2% reported they were ANA positive and 81.7% reported joint, 66.1% skin and 33.0% renal involvement. For the time before and in the first year after their SLE diagnosis, the majority reported fatigue (89.4%), joint pain (86.7%), photosensitivity (79.4%) and myalgia (76.1%). Of interest, more than half of the patients reported fever as an early symptom (53.7%).
Conclusion
For a Caucasian European SLE patient population, the overall characteristics suggest meaningful representation. While many symptoms were reported as expected, the high percentage of patients reporting fever and the significant number of patients with unexpected gastrointestinal complaints are of particular interest. These data add to the information on early SLE symptoms informing the development process of new SLE classification criteria.
Introduction
With its high variability in autoantibody-mediated symptoms, systemic lupus erythematosus (SLE) may be difficult to classify early in the course of disease. Of the two sets of SLE classification criteria commonly used today, the Systemic Lupus International Collaborating Clinics (SLICC) 2012 criteria 1 are more sensitive than the 1982 and revised 1997 American College of Rheumatology (ACR) criteria,2,3 albeit at the expense of lower specificity. Despite their advanced sensitivity, even the SLICC criteria show suboptimal recognition of patients with early SLE. 4 Accordingly, early classification is one goal of a joint European League Against Rheumatism (EULAR)/ACR project aimed at developing even better SLE classification criteria.
The first phase of this project was designed to broadly gather potential candidate items. This was approached with an SLE expert Delphi exercise 5 and an international early SLE cohort study. 6 It has been recommended by EULAR to include the patient perspective in EULAR supported projects. 7 Based on the feasibility of previous projects with the German SLE patient organization Lupus Erythematodes Selbsthilfegemeinschaft e.V.,8,9 the SLE classification criteria steering committee decided to add this additional patient-centered study.
Both clinical routine and discussions with the SLE patient organization resulted in the impression that SLE patients usually experience the onset and diagnosis as a critical life event and that memories of this time remain remarkably accurate. Accordingly, while patients can only be approached via the patient organization later in their disease course, the focus on early disease appeared feasible.
We here accordingly report, to our knowledge, the first ever approach to directly involve a large number of patients in the item generation phase of classification criteria development for any rheumatic disease.
Patients and methods
As approved by the local ethics committee, we conducted a cross-sectional survey of German SLE patients. An anonymous self-report questionnaire was published in the “Schmetterling” (English translation: Butterfly), the quarterly journal of the Lupus Erythematodes Selbsthilfegemeinschaft, the German SLE patient association. A total of 2498 copies of the questionnaire were mailed with the quarterly journal to members of the patient association. Patients were asked for year of and age at their initial diagnosis.
The questionnaire included a list of typical organ manifestations (skin, joints, renal, central nervous system (CNS), blood count, anti-phospholipid syndrome and fibromyalgia) and autoantibodies (ANA, anti-dsDNA, anti-Ro/SSA, anti-La/SSB, anti-Sm, anti-U1RNP and anti-cardiolipin). In addition, a list of characteristic symptoms (Raynaud’s, fatigue, fever, joint pain, myalgia, pleuritic pain, skin bleeding, skin rash, photosensitivity, leg edema and thrombosis) was provided. No specific definitions were given for any of these symptoms, but the terms were translated into simple descriptors (e.g. “blue/white fingers” for Raynaud’s, “muscle pain” for myalgia, and “pain when breathing” for pleuritic pain) where possible. In addition, patients were asked to add additional symptoms in free text.
For each symptom, boxes were provided to indicate the presence of the symptom before diagnosis, in the first year of the disease and at the time of completion of the questionnaire. Patients were instructed on the questionnaire as follows: “The first sheet aims at understanding your organ involvement. Please do only tick ‘Yes’ if you are sure that you have (or had) this organ problem yourself. Likewise, we would ask you to only tick specific autoantibodies when those have definitely been tested positive for you. For the symptoms, we would ask you to tick ‘Yes’ or ‘No’ for now, for the first year after your SLE diagnosis, and for the time before the diagnosis of SLE, for each specific symptom or problem. The last page is for symptoms that are not yet listed.” Questionnaires were anonymously completed and mailed to the Technische Universität Dresden Medical Center. The original questionnaire and the English translation are available as Supplement 1 and 2.
Patient characteristics

In the “All patients” column the denominator is all 339 patients that returned the questionnaire. In the “Y/N answer” column the denominator (given in parentheses) is the number of patients that gave yes or no answers.
Data from the questionnaires were extracted and analyzed in duplicate by B.M. and N.L. The free text symptoms were combined and, where adequate, subsumed under broader categories. Discrepancies where resolved by joint discussion. Descriptive statistics were performed using Microsoft Excel 2010 and GraphPad Prism 5.01. Questionnaires were included in the analysis when mailed within six months after publication.
Results
A total of 339 patient questionnaires were anonymously completed and sent to the Technische Universität Dresden Medical Center. This equates to a response rate of 13.6%. Of the respondents, 92.6% were female. The respondents’ mean age at diagnosis was 36.2 years, and their mean disease duration was 17.1 years. Patient characteristics are shown in Table 1.
Percentage of reported organ involvement at any time
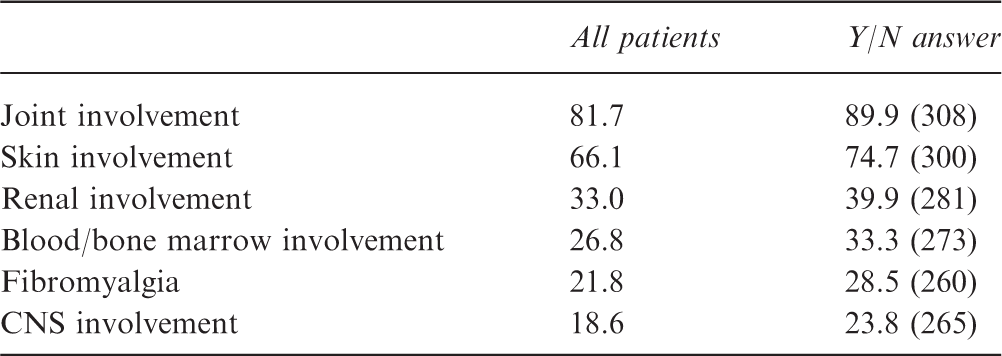
In the “All patients” column the denominator is all 339 patients that returned the questionnaire. In the “Y/N answer” column the denominator (given in parentheses) is the number of patients that gave yes or no answers.
CNS: central nervous system.
Frequency of symptoms in percent before diagnosis, at the time of diagnosis and at the time of questionnaire completion
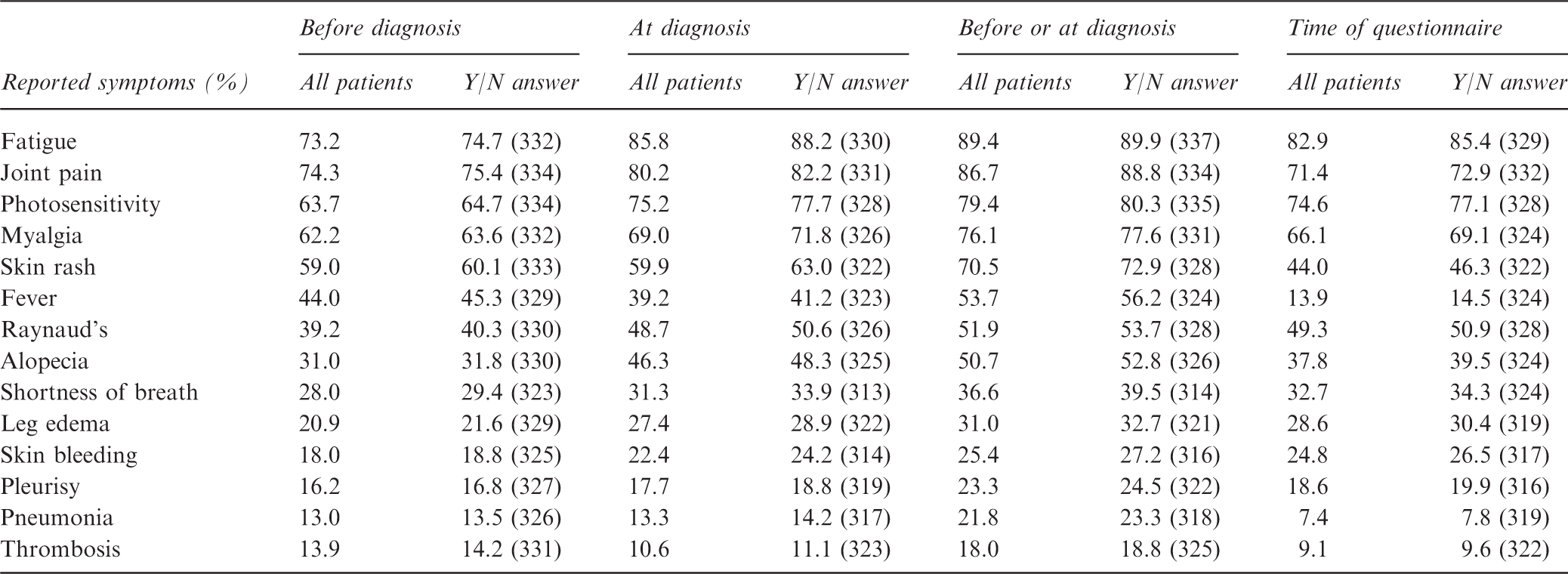
In the “All patients” column the denominator is all 339 patients that returned the questionnaire. In the “Y/N answer” column the denominator (given in parentheses) is the number of patients that gave yes or no answers.
In the check box list of symptoms in the early phase of the disease the highest percentages of reported symptoms were fatigue (89.4%), joint pain (86.7%), photosensitivity (79.4%), myalgia (76.1%) and skin rash (70.5%). All of the check box symptoms were reported at least numerically higher for the early phase of the disease, that is before or in the year after diagnosis, than for the time of the questionnaire (Table 3). Most check box symptoms were also reported more frequently in the first year after diagnosis than before diagnosis, except for fever and thrombosis. Notably, the highest differences between early and late phase symptoms were found for fever and pneumonia (Figure 1(a)), which were both reported around three times more frequently in early disease. Likewise associated with early disease were thrombosis, skin rash, alopecia and pleuritic pain. In contrast, skin bleeding, Raynaud’s, photosensitivity, fatigue and leg edema were reported with essentially unchanged frequency for late disease, defined as >90% of the frequency around diagnosis (Figure 1(b)).
Prevalence of predefined symptoms reported for early and late disease. (a) Symptoms reported more frequently for early disease; and (b) Symptoms reported for late disease at >90% of the frequency of early disease.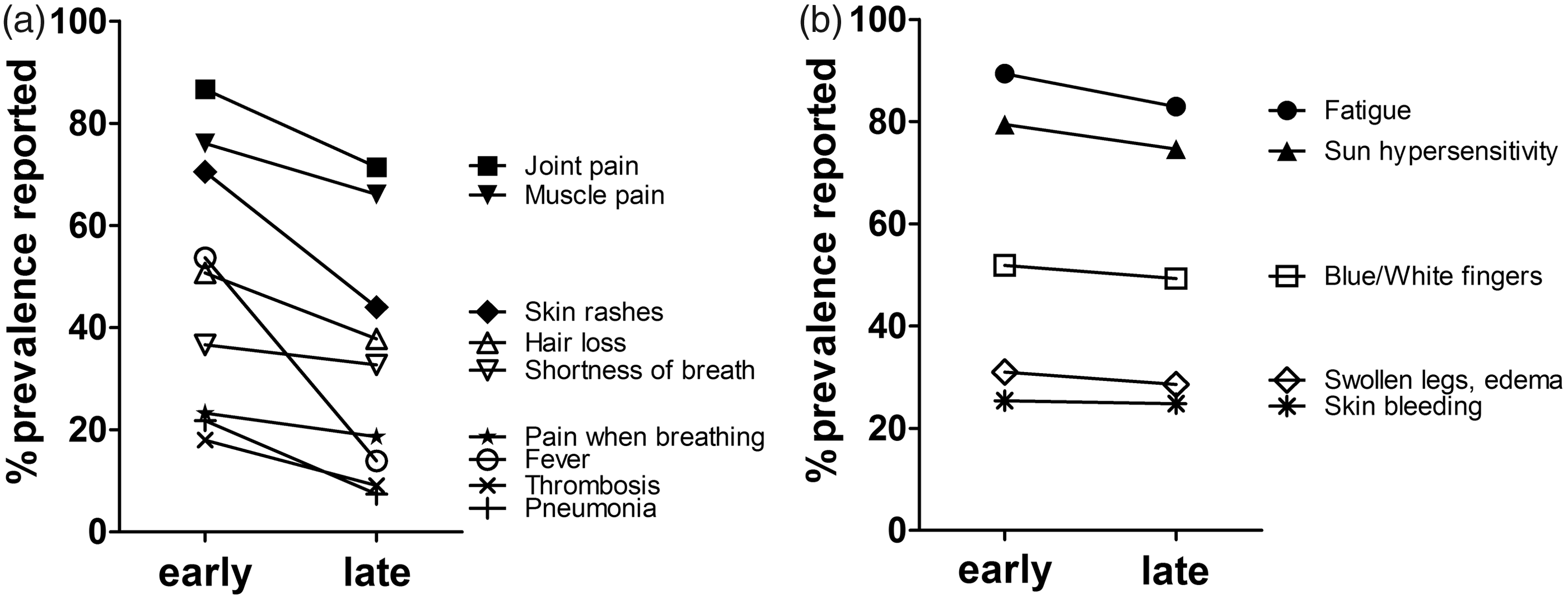
Free text symptoms beyond those predefined in the questionnaire

Please note that these patients volunteered these complaints without being reminded of such a possibility, which presumably led to relative underrepresentation.
Discussion
The overall patient characteristics are consistent with a Caucasian European patient population. The percentage of female patients and the age at diagnosis are similar to published cohorts.6,10,11 The participants had mostly long-standing disease with mean disease duration of 17.1 years. The prevalence of anti-dsDNA antibodies and anti-Ro/SSA antibodies was in the expected range. Although in a systematic literature review, 98% of SLE patients are positive for ANA on HEp-2 cells, 12 the fact that more than 4 in 5 patients (83.2%) were certain to be ANA positive is likewise reassuring. Still, underreporting of laboratory values (without symptoms) would be expected. Indeed, blood or bone marrow involvement was reported by 26.8% in this study only, as compared to 74% leukopenia in the international early lupus cohort study within this project, 13 80% in the Spanish Society of Rheumatology SLE registry (RELESSER) cohort and 59% in the ACR 1982 cohort.3,11
Percentage of symptoms reported in this study compared to four published SLE cohorts
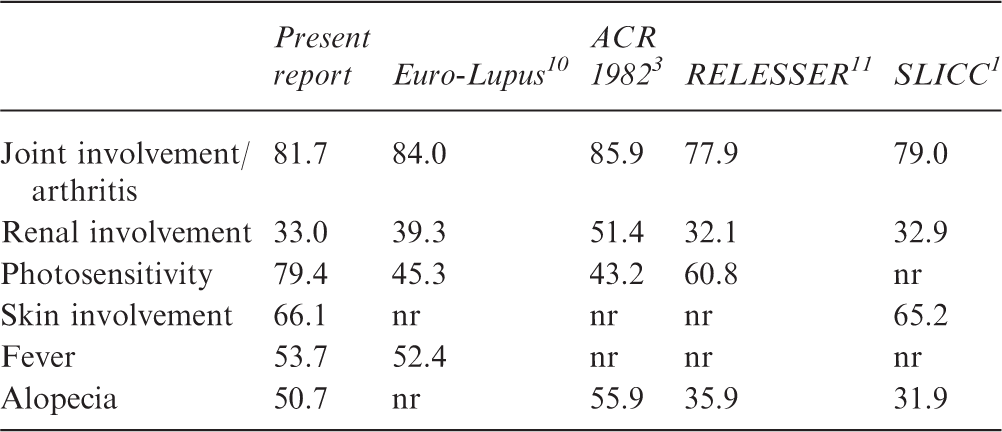
ACR: American College of Rheumatology; Euro-Lupus: European Working Party on SLE cohort; nr: not reported in this cohort; RELESSER: Spanish Society of Rheumatology SLE registry; SLE: systemic lupus erythematosus; SLICC: Systemic Lupus International Collaborating Clinics.
Many of the inflammatory manifestations of SLE are known to decrease over time. 14 This is in part attributed to treatment effects. Such reduction in inflammatory symptoms is also evident from the present study, as most symptoms were reported with lower frequency at the time of the questionnaire. Among the symptoms less commonly present over time were rash, alopecia, joint pain and myalgia. While fever may also be due to infections associated with high level immunosuppression, 16 non-infectious fever apparently is quite common in early SLE, and may indeed be a distinguishing feature. 6 As a possible limitation to this finding, fever might be overreported by patients since no specific definition was given and no objective method was required.
These data accordingly suggest face validity of the patients’ memory and mostly correct patient attribution of their symptoms to SLE. This may have been aided by the fact that patients organized in SLE patient groups are particularly well-informed and may have reflected on their symptoms quite early in their disease. Under these circumstances, it is interesting that approximately 5% of the patients volunteered gastrointestinal complaints, which were not expected and therefore not asked for. None of the published SLE cohorts compared in Table 5 included gastrointestinal symptoms. In combination with an earlier patient Delphi similarly showing gastrointestinal complaints in SLE patients, 9 these yet unclear symptoms should be placed on the scientific agenda.
Taken together, this first attempt to directly include patient reported symptoms into an SLE classification criteria approach was successful in providing relevant data on candidate criteria items relevant for early SLE. The majority of symptoms and manifestations recalled by the SLE patients in this study were in line with published literature. Importantly, however, the frequencies of fever and gastrointestinal complaints were unexpectedly high and need consideration. Non-infectious fevers are apparently quite common in early active SLE, and may be a useful SLE criterion.
Supplemental Material
Supplemental material for Early symptoms of systemic lupus erythematosus (SLE) recalled by 339 SLE patients
Supplemental material for Early symptoms of systemic lupus erythematosus (SLE) recalled by 339 SLE patients by N Leuchten, B Milke, B Winkler-Rohlfing, D Daikh, T Dörner, S R Johnson and M Aringer in Lupus
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the SLE classification criteria project, of which this study is a part, has been jointly supported by the European League Against Rheumatism (EULAR) and the American College of Rheumatology (ACR).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.