
Abstract
Objective
The objective of this paper is to investigate the utility of serum procalcitonin (PCT) and C-reactive protein (CRP) as markers of infection in systemic lupus erythematosus (SLE) patients.
Patients and methods
Sixty-nine SLE patients with symptoms and signs of infection proved by culture and/or a favorable response to antibiotics and 69 SLE patients without infection were included. Serum PCT and plasma high-sensitivity CRP were assessed by an enzyme-linked immunosorbent assay.
Results
SLE patients with infection had a significantly higher level of CRP than those without infection ((median (IQR) 104.5 (25.5–100.9) and 10.3 (5.4–23.1) mg/l, respectively), p<0.001).
Conclusion
Serum PCT could not differentiate SLE patients with or without bacterial infection in this study, while the utility of CRP as a marker of infection has been confirmed.
Introduction
Infections are a major cause of morbidity and mortality in systemic lupus erythematosus (SLE) patients. 1 Clinical features of infection may mimic those of active lupus, making it difficult to detect the coexistence of infection. Active lupus requires immunosuppressive therapy, whereas infection requires antibiotics and reduction of the doses of immunosuppressive drugs, a dilemma that necessitates proper timely diagnosis. 2
C-reactive protein (CRP) production is an acute-phase reactant that has been proven useful for the detection of infection in immunocompromised individuals, and in the few specific diseases characterized by modest acute-phase responses such as SLE and ulcerative colitis. 3 In some SLE manifestations, however, notably arthritis and serositis, CRP levels may rise. 4
Procalcitonin (PCT) is a 116 amino acid peptide with a sequence identical to the prohormone of calcitonin. PCT itself, however, has no known hormonal activity. Under normal metabolic conditions, PCT is found only in the C cell of the thyroid gland. Plasma PCT levels in healthy humans are negligible. 5 In systemic bacterial infections, PCT is secreted from all parenchymal tissues and different cell types of the body and its levels increase as early as within three hours, and persist for several days. PCT levels > 0.5 ng/ml strongly suggest the presence of bacterial infection, on the other hand, PCT levels are not reliable in the diagnosis of viral or fungal infections. 6
The ability of PCT to differentiate systemic bacterial infection from lupus flares in SLE is controversial.7–12 Also, regarding the sensitivity and specificity of PCT and CRP in the diagnosis of infection in SLE patients, there has been debate as to whether PCT is superior,8,11 inferior 9 or comparable to CRP. 13
The aim of this work is to investigate the utility of serum PCT and CRP as markers of infection in SLE patients.
Patients and methods
Participants
A prospective study was conducted between July 2014 and August 2015, in which 138 consecutive SLE patients with or without infection (94.9% females) aged 14–59 years were recruited from the follow-up clinic or the inpatient ward of the Rheumatology and Rehabilitation Department, Cairo University Hospital. Diagnosis of SLE was based on the Systemic Lupus International Collaborating Clinics classification criteria (SLICC) for SLE. 14 Two groups of patients were studied. The first group consisted of 69 patients with symptoms and signs of infection proved by culture and/or a favorable response to antibiotics, whereas the second group consisted of 69 patients with no evidence of infection. Patients with severe trauma, major burns or major surgery; viral, parasitic, fungal infections; or an uncertain diagnosis of infection and end-stage liver disease were excluded. All patients gave informed consent to participate in the study. The protocol of the study has been approved by the local ethics committee and conforms to the provisions of the Medical Association of Helsinki.
Methods
Patients underwent full history taking, clinical examination and laboratory investigations including complete blood count, serum alanine aminotransferase, aspartate aminotransferase, albumin, creatinine, serum complement components C3 and C4, urine analysis and 24-hour urinary proteins. Disease activity was assessed using the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and organ damage using the SLICC/American College of Rheumatology Damage Index (SLICC/ACR DI). 15
In patients with infection, serum samples were obtained within the first 48 hours of symptoms suggestive of infection before initiation of antibiotics. Serum PCT was measured using the Glory Science Co PCT enzyme-linked immunosorbent assay (ELISA) kit (Hong Kong, China), with a detection limit of 0.04 ng/ml. PCT is not available at our hospital as a routine laboratory test for infection. PCT ELISA kits were specifically provided for this study. Positive and negative controls were included in the kit. High-sensitivity CRP was measured using the Immunospec high-sensitivity CRP ELISA kit (Los Angeles, CA, USA) with a detection limit of 0.1 mg/l. Biological samples were obtained from the site of infection and sent to the laboratory for culture and sensitivity testing. Bacterial infection was diagnosed based on clinical manifestations and positive cultures and/or response to antibiotics.
Patients with infection were further subdivided into patients with localized infection, i.e. infections in a single location in the body like cellulitis 16 and systemic infections. Systemic infections were further classified into sepsis and severe sepsis according to the International Sepsis Criteria. Sepsis is defined as the presence (probable or documented) of infection together with systemic manifestations of infection. Severe sepsis on the other hand is defined as sepsis plus either organ dysfunction or tissue hypoperfusion. Tissue hypoperfusion is defined as systolic blood pressure (SBP) < 90 mmHg, mean arterial pressure <70 mmHg, a decrease of SBP >40 mmHg or an SBP <2 standard deviations below the normal for age in absence of other causes of hypotension. 17
Statistical methods
The data were coded and entered using the statistical package SPSS, version 15. The data were summarized using descriptive statistics: median and interquartile range (IQR) for quantitative variables and number and percentage for qualitative values. Statistical differences between groups were tested using the chi square test for qualitative variables and Mann–Whitney U test for the comparison of quantitative variables. P values less than or equal to 0.05 were considered statistically significant. Receiver operator characteristic (ROC) analysis was conducted and area under the curve (AUC) was calculated to determine the optimum cut-off value of the studied diagnostic markers.
Results
Characteristics of the studied SLE patients
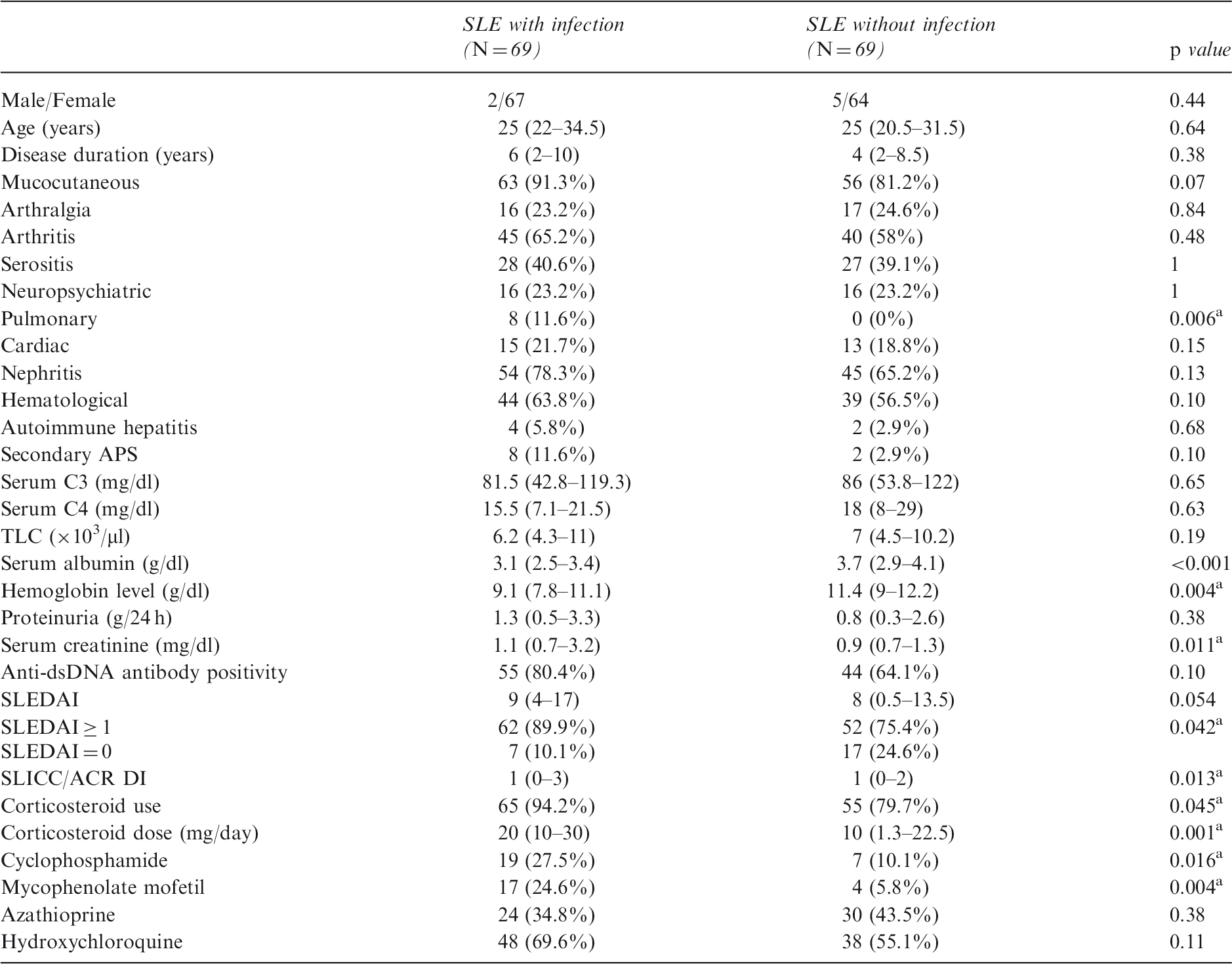
Anti-dsDNA: anti-double-stranded deoxyribonucleic acid antibody; APS: antiphospholipid antibody syndrome; C: complement factor; IQR: interquartile range; SD: standard deviation; SLE: systemic lupus erythematosus; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SLICC/ACR DI: Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index; TLC: total leukocyte count. Values are expressed as number (%) or median (IQR). aSignificant p value < 0.05.
Characteristics of infection
Sites of infection and isolated microorganisms in SLE patients with infection
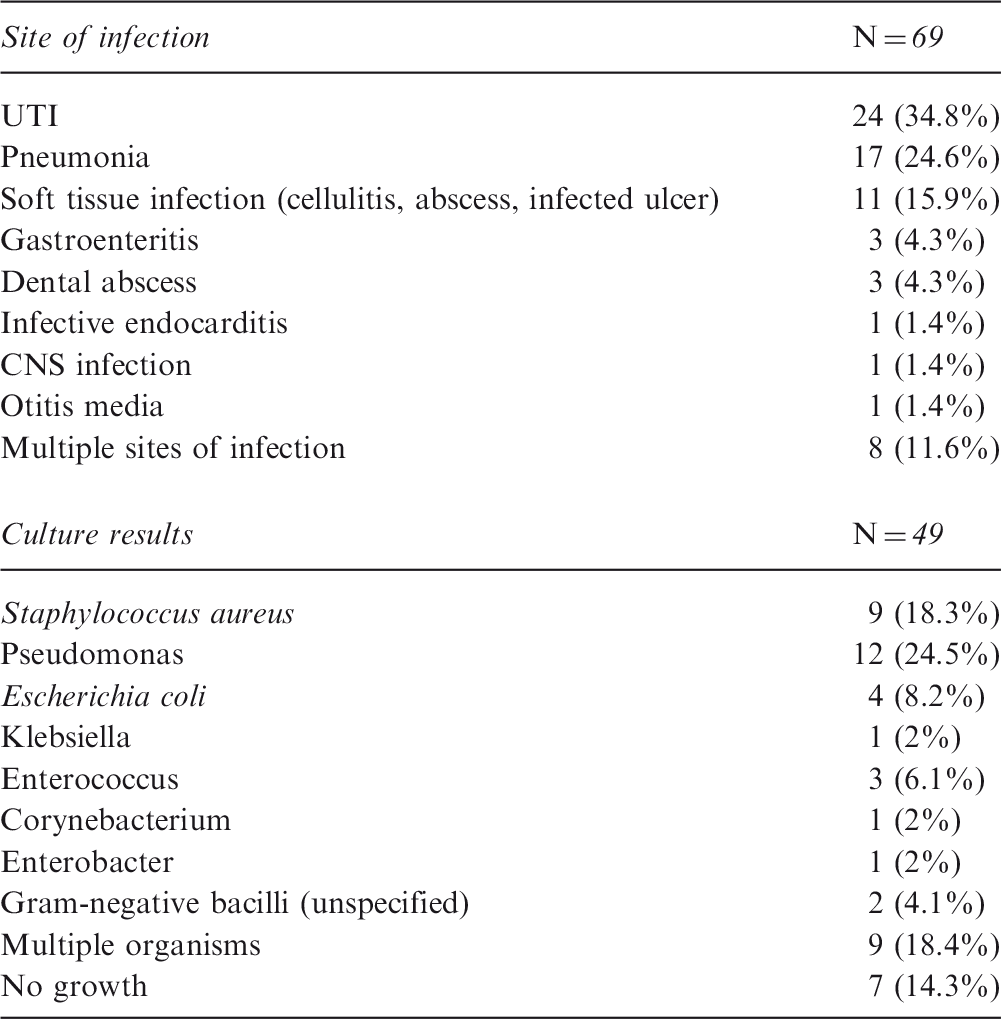
CNS: central nervous system; SLE: systemic lupus erythematosus; UTI: urinary tract infection.
Concerning the severity of infection in the 69 patients, 26 (37.7%) patients had localized infection, 26 (37.7%) had sepsis and 17 (24.6%) patients had severe sepsis. Six patients were admitted in the intensive care unit (ICU), of whom five (83.3%) patients were mechanically ventilated. Among the 43 patients with sepsis, 11 (25.6%) patients did not survive.
Analysis of CRP and PCT as markers of infection in SLE
SLE patients with infection had a significantly higher level of CRP than those without infection (median (IQR) 104.5 (25.5–100.9) and 10.3 (5.4–23.1) mg/l, respectively), p < 0.001. Further subgroup analysis revealed significantly higher CRP in patients with systemic infection compared to those with localized infection (median (IQR) 100.1 (88.8–102.3) and 23.8 (12.4–66.1) mg/l, respectively), p < 0.001 (Figure 1).
Among patients with active disease (SLEDAI ≥ 1, n = 114), CRP level was significantly higher among patients with infection (median (IQR) of 99.3 (45.6–101.6); versus 12.1 (5–31.7) mg/l in those without infection, p < 0.001) while among patients in remission (SLEDAI = 0, n = 24), there was no significant difference between both groups with median (IQR) CRP levels of 19.6 (5.5–91) and 17.2 (5.8–26.6) mg/l in patients with and without infection, respectively, p = 0.19. Among the seven patients in remission with evidence of infection, five patients had localized infection and two had systemic infection.
Comparing CRP levels between sepsis survivors (n = 32) and non-survivors (n = 11) showed no statistically significant differences (median (IQR) were 99.2 (63.8–102.3) and 100.9 (100.1–102.2) mg/l, respectively, p = 0.29).
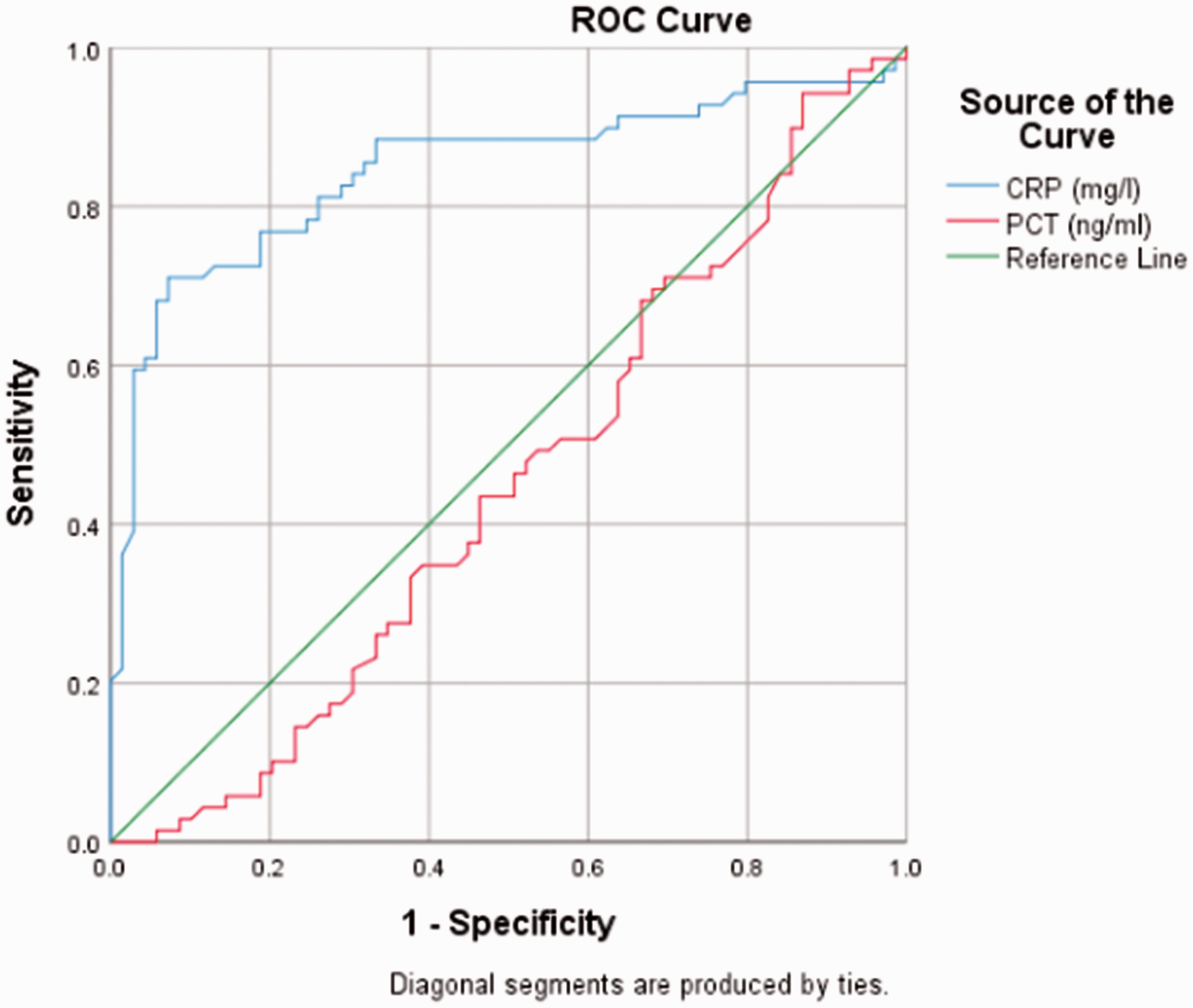
The AUC 95% confidence interval (CI) for CRP was 0.85 (0.78–0.92). The cut-off value for CRP was 19.2 mg/l, at which sensitivity (81.2%) and specificity (73.9%) had the best combination. At this value the test had a positive likelihood ratio of 3.11 and a negative likelihood ratio of 0.25 (Figure 2).
C-reactive protein (CRP) levels in systemic lupus erythematosus patients according to infection status. Receiver operator characteristic (ROC) curve for C-reactive protein (CRP) and procalcitonin (PCT) in systemic lupus erythematosus patients.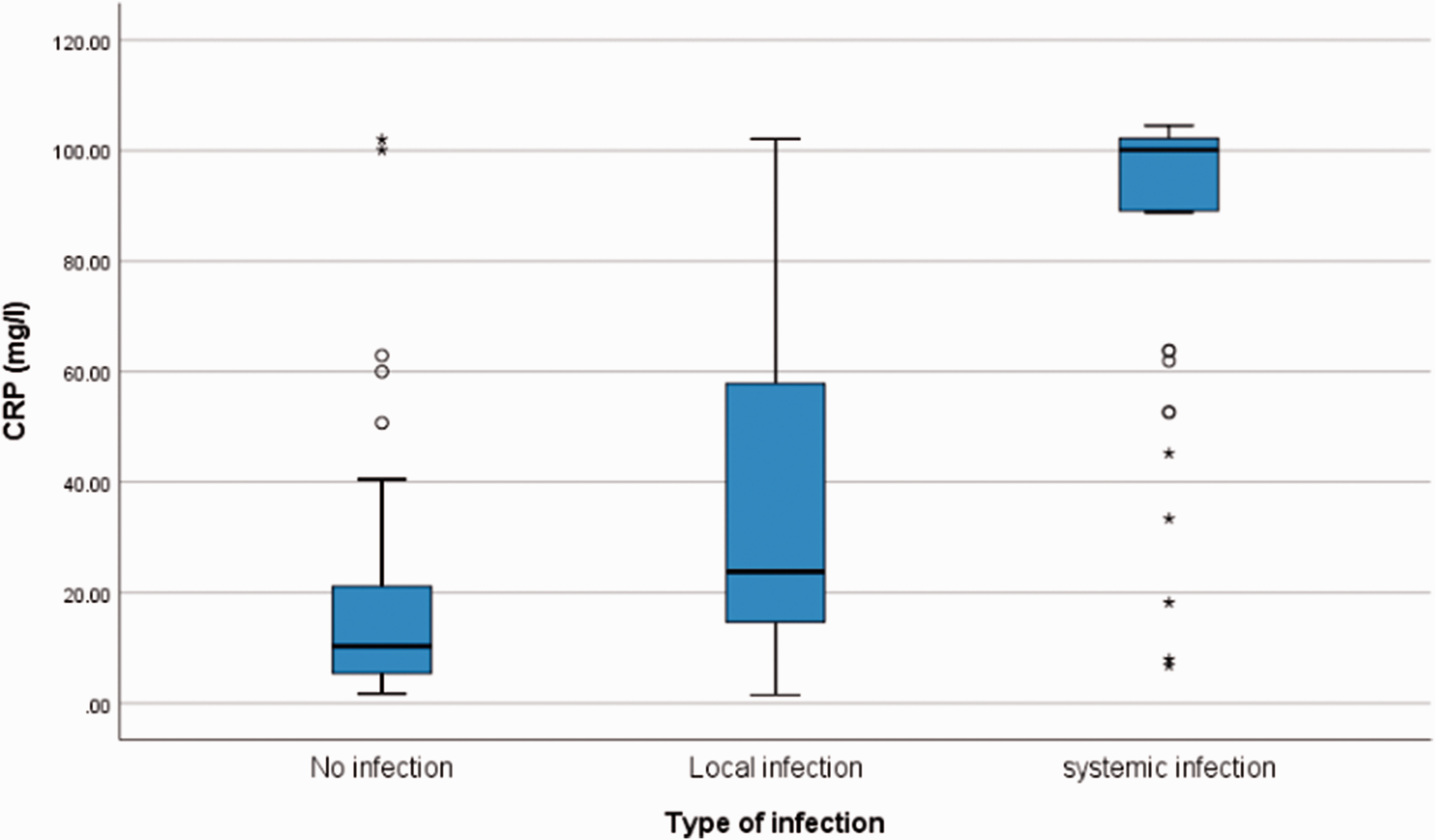
On the other hand, there was no significant difference in PCT levels between SLE patients with infection and those without (median (IQR) of 0.25 (0.22–0.37) and 0.27 (0.22–0.38) ng/ml, respectively), p = 0.062. Subgroup analysis revealed no significant difference between PCT levels in patients with localized compared to those with systemic infection (median (IQR) 0.25 (0.21–0.37) and 0.26 (0.23–0.36) ng/ml, respectively, p = 1.0), Figure 2.
Procalcitonin (PCT) levels in systemic lupus erythematosus patients according to infection status.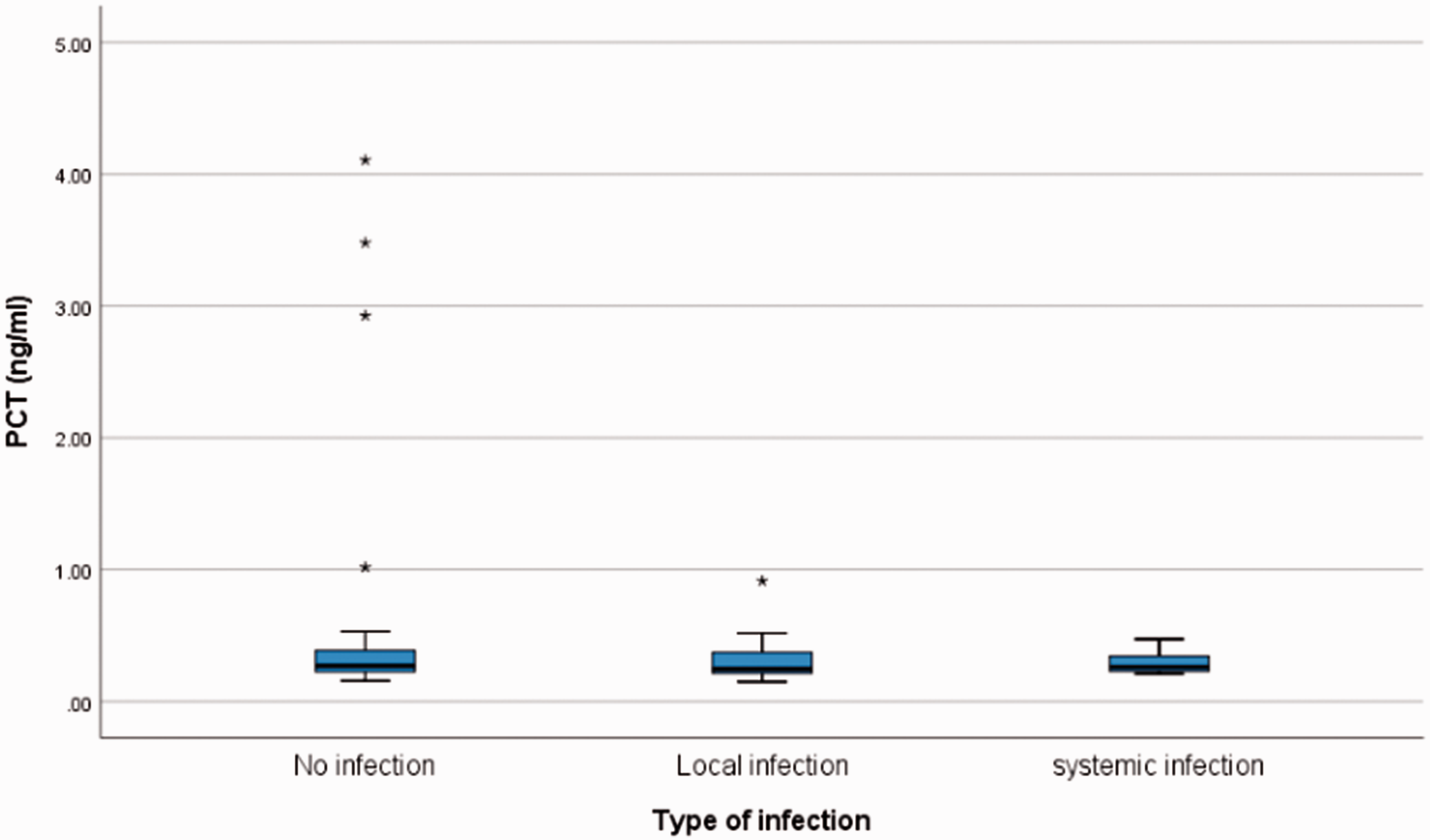
Among patients with positive culture, there was also no difference in PCT values between patients with gram-positive and gram-negative bacteria (median (IQR) 0.29 (0.23–0.37) and 0.24 (0.21–0.34) ng/ml, respectively, p = 0.16). The AUC and 95% CI for PCT were 0.55; and 0.51–0.70, respectively, denoting that PCT is not a successful marker for the diagnosis of infection in SLE patients (Figure 2).
Among patients with active disease, the median (IQR) PCT level was 0.26 (0.22–0.37) and 0.25 (0.22–0.38) ng/ml in patients with and without infection, respectively, p = 0.067. Among patients in remission, the median (IQR) PCT levels were 0.21 (0.20–0.44) and 0.3 (0.23–0.44) ng/ml in patients with and without infection, respectively, p = 0.88.
Characteristics of SLE patients with PCT ≥0.5
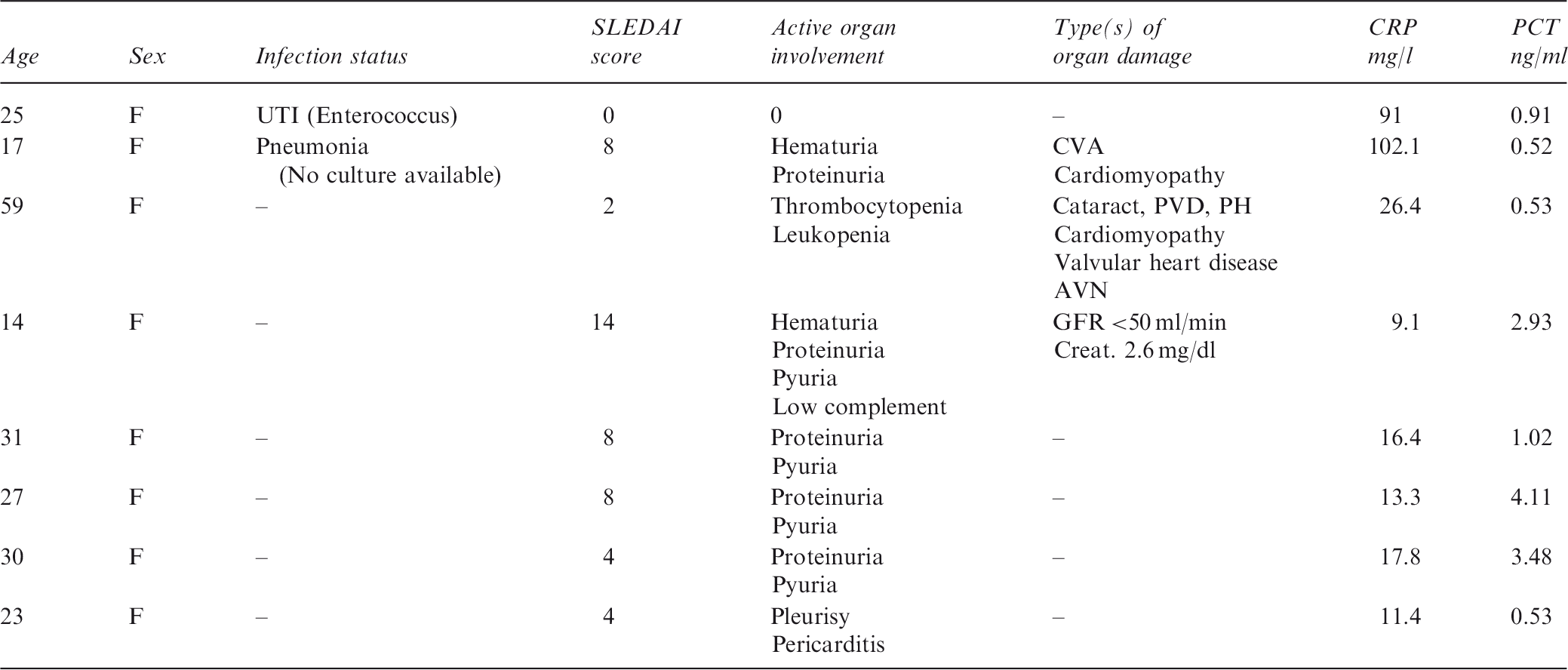
AVN: avascular necrosis; CVA: cerebrovascular accident; Creat.: creatinine; F: female; GFR: glomerular filtration rate; PH: pulmonary hypertension; PVD: peripheral vascular disease; SLE: systemic lupus erythematosus; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; UTI: urinary tract infection.
Discussion
In acute inflammation PCT rises in response to bacterial endotoxin and inflammatory cytokines. Tumor necrosis factor (TNF) alpha rises first, followed by interleukin-6, then PCT, which precedes CRP secretion. PCT is considered a secondary mediator in the inflammatory cascade that can intensify but not initiate the inflammatory cascade in sepsis. 18 The level of PCT secreted depends on the level of TNF alpha produced, being higher in gram-negative infections and malaria while infections in which other inflammatory pathways are activated do not increase PCT levels. PCT is usually not elevated in localized forms of infection such as abscesses and with intracellular organisms such as viral infections or mycobacteria. 19 PCT elevation at the onset of sepsis was found to be lower in patients with a recent history of previous sepsis (secondary sepsis) than in those experiencing their first episode of systemic infection, regardless of the severity of the disease, possibly due to sepsis-related alteration of the systemic immune response. 20
Several studies demonstrated the ability of PCT to differentiate between SLE patients with infection and those in flare.7–11 Among SLE patients with infection, PCT levels were higher among those complicated by sepsis.8,9,11 The proposed cut-off levels of PCT to diagnose bacterial infection in SLE patients varied from 0.025 to 0.74 ng/ml in different studies with sensitivities ranging from 38% to 89.5% and specificities ranging from 78% to 100%.8,9,11,13
On the contrary, in a study conducted by Lanoix et al., 12 5/60 SLE patients had systemic infection and PCT was normal in all of them. In the present study, PCT levels were not significantly different between SLE patients with or without infection and were not different between those with localized or systemic infections. Furthermore, eight patients had a PCT ≥ 0.5 ng/ml; only two of these patients had a localized form of infection, and seven had manifestations of active disease. Although in a systematic review PCT levels ≥0.5 μg/l were suggested to strongly indicate bacterial infection in the context of SLE, 21 a recent meta-analysis found that serum PCT levels were not significantly different between SLE patients with infection and those without, while subgroup analysis revealed elevated PCT levels with infection in Asian studies. 22
The reason why PCT did not rise with systemic infections in the studied patients is unknown to us; however, other investigators reported that 15%–37.9% of patients diagnosed with sepsis, including cases with severe sepsis and septic shock, had persistently low PCT levels.23–25 The heterogeneity of the infectious organisms, inclusion of culture-negative sepsis and patients with multiple organisms in culture could have accounted for the low PCT levels in this study. The timing of PCT testing is important. It has been reported that up to 22.7% of severe sepsis patients had initially low PCT levels; 23 moreover, after a PCT peak, patients with a sepsis-related lethal outcome showed a decline in PCT levels in the last days of their ICU stay. 26
Although infrequent, elevated PCT has been reported in some SLE patients with disease flare in the absence of infection.11,12,27,28 Elevated PCT levels were found in 41/49 patients with SLE-associated macrophage activation syndrome, a life-threatening, sepsis-like hyperinflammatory condition. 29
CRP is the most critical marker in differentiating between infection and disease flare up in SLE 2 and has recently been proposed to be included in an algorithm to diagnose infection in febrile SLE patients. 30 The elevation of CRP level with infection in SLE patients was not significantly affected by regular corticosteroid or immunosuppressant use or the daily corticosteroid dose. 31
In the present study, we found that CRP was higher among SLE patients with infection compared to those without infection, which is in agreement with other investigators.9–13 Moreover, CRP level was found to be higher in patients with systemic infection compared to those with localized infections, which was not confirmed in other studies.8,9,11 Among patients with active disease, but not among those in remission, CRP levels were higher with infection. Similar results were obtained by Bador et al. 13 A possible explanation could be that in the present study, among the patients in remission and co-existing infection, most infections were of the localized type without marked elevation of CRP.
In the present study a cut-off value of 19.2 mg/l is suggested, at which the sensitivity for the diagnosis of infection was 81.2% and the specificity was 73.9%. Other investigators proposed cut-off values ranging from 7.1 to 161 mg/l to diagnose infection in SLE patients with sensitivities ranging from 55% to 100% and specificities ranging from 62.7% to 90%.8,9,11,32
CRP has been shown to be among the promising biomarkers that predict sepsis survival; 33 however, Devran et al. 34 reported that CRP level assessed on the third day of the ICU stay, but not initial CRP, was a predictor of mortality in patients with severe sepsis. No statistically significant differences were found in CRP levels between sepsis survivors and non-survivors in the present study; a possible explanation could be that CRP levels were available at baseline evaluation only.
Conclusion
PCT was not useful for the diagnosis of infection in SLE patients while CRP levels ≥19.2 mg/l identified the presence of infection with a sensitivity of 81.2% and a specificity of 73.9%.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.