
Abstract
Background
We aimed to identify risk factors for early complications in systemic lupus erythematosus (SLE) patients undergoing major surgery.
Methods
We conducted a retrospective comparative cohort study including patients with SLE undergoing major surgery, and non-SLE patients matched 1:1. Main outcomes were development of infectious and noninfectious complications, and 30-day postoperative mortality.
Results
A total of 382 patients (191 SLE and 191 non-SLE) were included. Postoperative complications occurred in 82 (43%) SLE patients and 58 (30%) without SLE, (p = 0.01). Variables associated with infectious complications in SLE patients: prednisone use (OR 1.81, 95% CI 1.13–2.90), anemia (OR 2.43, 95% CI 1.45–4.08), hypoalbuminemia (OR 2.58, 95% CI 1.55–4.30) and lymphopenia (OR 2.43, 95% CI 1.52–3.89), p < 0.05. Variables associated with noninfectious complications: anemia (OR, 1.93, 95% CI 1.03–3.64) and hypoalbuminemia (OR 2.11, 95% CI 1.16–3.86), p < 0.05. Variables associated with any complication: SLEDAI-2K (OR 1.1, 95% CI 1.01–1.20), nephritis (OR 10.08, 95% CI 1.21–83.63), aspirin use (OR 2.68, 95% CI 1.19–6.02, p = 0.01), low C3 (OR 2.00, 95% CI 1.06–3.80), anemia (OR 2.68, 95% CI 1.39–5.18), hypoalbuminemia (OR 3.49, 95% CI 1.83–6.66) and lymphopenia (OR 2.36, 95% CI 1.30–4.26), p < 0.05. More patients with SLE died (6% vs 1%, p = 0.02).
Conclusions
SLE patients present higher frequency of postoperative complications and mortality compared with non-SLE patients. Hypoalbuminemia, anemia, lymphopenia and aspirin use are independent risk factors.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease with variable clinical expression and severity that affects mainly women in their reproductive years.1,2 Pathophysiology is multifactorial and comprises environmental, neuroendocrine, genetic, hormonal and infectious mechanisms. 3 Mortality in SLE patients displays a bimodal pattern: Early death is associated with disease activity and severe infections, while late mortality is due to cardiovascular complications related to atherosclerosis. 1
SLE patients present traditional cardiovascular risk factors (i.e. dyslipidemia, diabetes mellitus, arterial hypertension, obesity and smoking) but also premature atherosclerosis due to chronic inflammation, characterized by monocytes/macrophages activation and production of inflammatory cytokines, such as tumor necrosis factor alpha and interferon gamma. In the Framingham Study, women with SLE aged 44–50 years showed 50 times more risk of acute myocardial infarction compared with controls. 4
Prospective studies have shown that nontraditional risk factors contribute to subclinical atherosclerosis in SLE patients. These factors include disease activity, cumulative prednisone dose, renal failure, vascular inflammation and endothelial damage, as well as antiphospholipid syndrome (APS). 5 Clinical and serologic SLE manifestations associated with increased risk of cardiovascular events include thrombocytopenia, pericarditis, lymphopenia, neurologic involvement and antiphospholipid antibodies, while the use of antimalarials has shown protective effects. 6
Cardiovascular events comprise the main cause of perioperative morbidity and mortality, especially in patients with additional risk factors such as diabetes mellitus, arterial hypertension and SLE. A retrospective study analyzed women aged > 18 years with SLE who underwent elective noncardiac surgery and compared them to women without SLE. The results showed that SLE women presented higher cardiovascular morbidity and mortality in low- and high-risk procedures, with no differences in intermediate-risk procedures. 7 Another retrospective study that analyzed Taiwanese women with and without SLE undergoing major surgery found a higher rate of early complications (<30 days) and mortality in SLE patients, and identified the presence of a severe SLE relapse (requiring hospitalization) in the prior six months as a risk factor for postoperative morbidity and mortality. 1
Given the lack of preoperative prognostic indexes in SLE patients, we aimed to identify risk factors for early infectious and noninfectious complications in SLE patients undergoing major noncardiac surgery at our tertiary care center.
Materials and methods
We conducted a retrospective comparative cohort study, including patients > 18 years old with an SLE diagnosis according to the American College of Rheumatology (ACR) revised criteria 8 who underwent noncardiac emergent, urgent or elective major surgery, defined as any procedure in which general or epidural anesthesia was used and hospitalization was required for at least 24 hours. 9 Surgeries were performed between January 2010 and December 2015 in the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, a tertiary care center in Mexico City.
SLE patients were matched 1:1 with patients without SLE or other connective tissue disease according to age ±5 years, gender and type of surgical procedure (e.g. appendectomy, hystero-oophorectomy). Patients with primary APS or other overlapping connective tissue diseases were excluded.
All data were abstracted from the medical records and included: demographic variables; SLE clinical characteristics at diagnosis and at the time of the surgery; disease duration and presence of secondary APS; comorbidities (obesity, smoking, arterial hypertension, diabetes mellitus, dyslipidemia, heart failure, end-stage renal disease, cancer and cerebrovascular disease); use of oral anticoagulants or aspirin; SLE treatment at the time of surgery, including dose of immunosuppressants; disease activity and damage accrued at the time of surgery using the Systemic Lupus Erythematosus Disease Activity Index-2000 (SLEDAI-2K) and Systemic Lupus International Collaborating Clinics/ACR Damage Index SLICC/ACR-DI, respectively.10,11 The presence of a severe SLE manifestation three months before surgery was considered, defined as SLEDAI-2K score > 12, a new clinical manifestation or worsening of vasculitis, lupus nephritis, thrombocytopenia < 60,000/mm3 or autoimmune hemolytic anemia that required doubling the prednisone dose, or a dose >0.5 mg/kg/day, and/or an increase of prednisone > 0.5 mg/kg/day or new onset of immunosuppresants. 12
Preoperative variables included laboratory parameters and SLE serologic disease activity markers such as anti-double-stranded DNA (anti-dsDNA), complement C3 and C4; preoperative cardiovascular risk assessment 13 and Charlson Comorbidity Index. 14 Anemia was defined as a serum hemoglobin < 12 g/dl, lymphopenia as a total lymphocyte count <1000/mm3, and hypoalbuminemia as a serum albumin < 3.5 g/dl. Intervention times, blood transfusion requirements, duration of mechanical ventilation, days in the intensive care unit (ICU), length of hospital stay, second intervention or rehospitalization were also assessed.
Main outcomes were the development of infectious or noninfectious complications and mortality 30 days after surgery. Infectious complications were identified using radiological and microbiological tests and included septic shock, pneumonia, urinary tract infection, surgical wound infection, bacteremia, cellulitis, abdominal sepsis, osteomyelitis, diarrhea and prosthetic infection. Noninfectious complications comprised thrombosis (myocardial infarction, pulmonary embolism, deep vein thrombosis and cerebrovascular event), bleeding, hemorrhagic or cardiogenic shock, arrhythmia, acute kidney injury and hypocalcemia. Causes of death were retrieved from the death certificates. Severe SLE manifestations 30 days after surgery were also considered, including thrombocytopenia, glomerulonephritis, autoimmune hemolytic anemia, diffuse alveolar hemorrhage, myocarditis, serositis, seizures and cutaneous manifestations.
The hospital institutional review board approved the study (approval reference IRE-2002-16/17-1), and compliance with the Helsinki Declaration was followed. Informed consent was not obtained because of the retrospective nature of the study.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation (SD) or median with minimum and maximum range; categorical variables are expressed as counts and percentages. Differences between groups were evaluated with the Student t test or Mann-Whitney U test for continuous variables and chi-squared or Fisher exact test for categorical variables. Univariate logistic regression analyses and multivariate analyses were performed using logistic regression to analyze associations between significant variables (p ≤ 0.10) identified from the bivariate analyses. Significant variables had to be present in at least 20% of patients with SLE to be eligible to enter the model. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated. A value of p < 0.05 was set and two-sided values are reported. All analyses were performed using Stata (Stata Corp; College Station, TX, USA), version 12.0.
Results
Types of surgeries and surgical risk
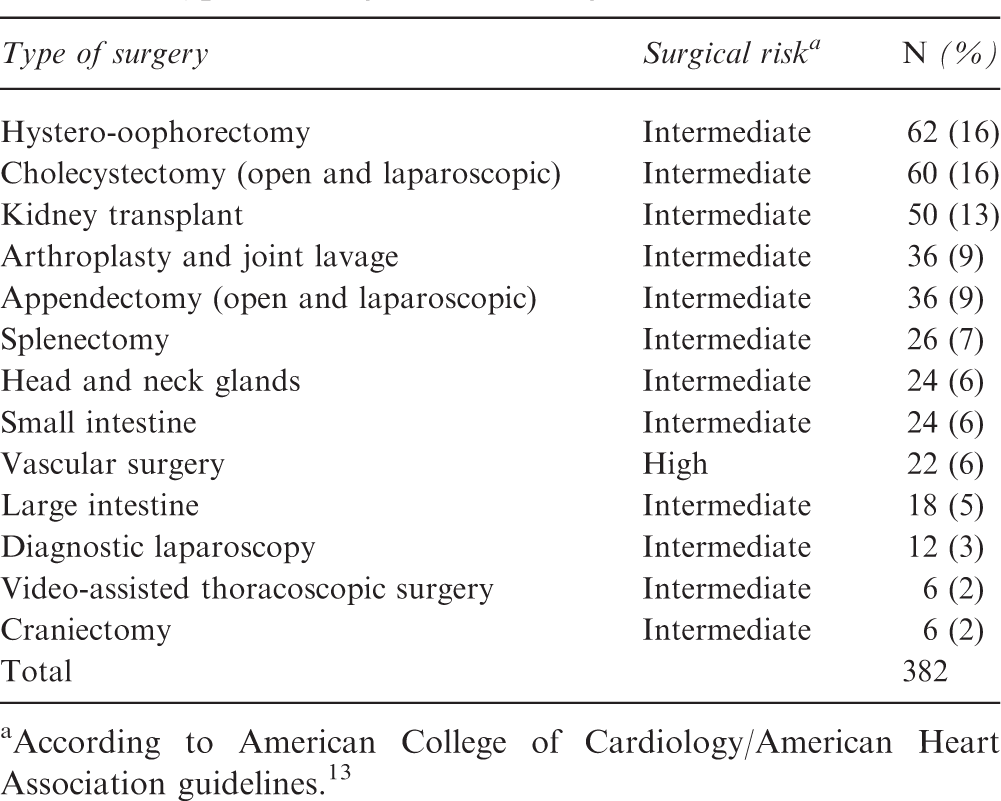
According to American College of Cardiology/American Heart Association guidelines. 13
Characteristics of SLE patients
Characteristics of SLE patients
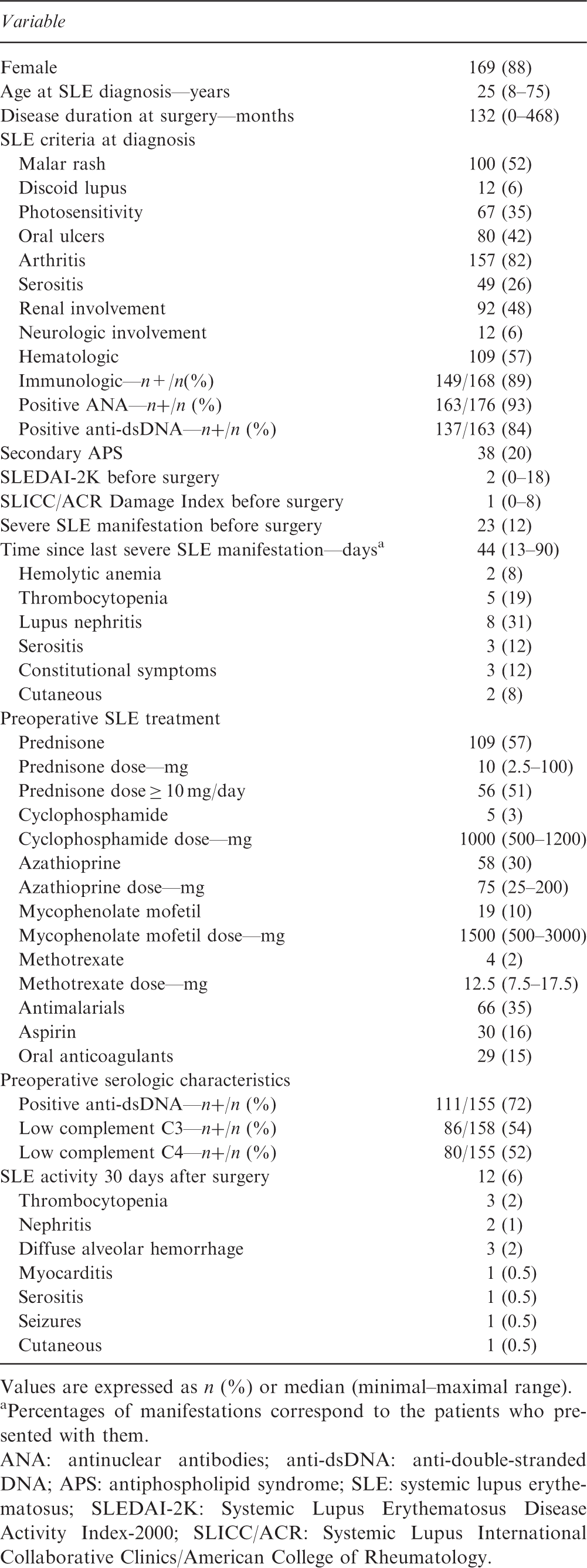
Values are expressed as n (%) or median (minimal–maximal range).
Percentages of manifestations correspond to the patients who presented with them.
ANA: antinuclear antibodies; anti-dsDNA: anti-double-stranded DNA; APS: antiphospholipid syndrome; SLE: systemic lupus erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index-2000; SLICC/ACR: Systemic Lupus International Collaborative Clinics/American College of Rheumatology.
Comparative analysis of patients with and without SLE
There were no differences regarding gender or age; SLE patients showed more frequency of hypertension, dyslipidemia and cerebrovascular disease compared to non-SLE patients (41% vs 31%, p = 0.05; 30% vs 20%, p = 0.02, and 6% vs 1%, p = 0.02, respectively). No differences were found between groups in preoperative risk assessment depending on the type of procedure (low, intermediate or high-risk), nor in the surgical indication (elective, urgent or emergent procedures). Preoperative Charlson Comorbidity Index estimated lower 10-year survival in SLE patients compared to non-SLE patients (85% vs 90%, p < 0.001).
As expected, SLE patients were more frequently receiving corticosteroids and immunosuppressants than non-SLE patients (57% vs 13%, p < 0.001, and 44% vs 7%, p < 0.001, respectively). Moreover, differences were found in preoperative laboratory tests between groups, with more frequency of anemia, hypoalbuminemia and lymphopenia in SLE patients compared to non-SLE patients (68% vs 55%, p = 0.01; 31% vs 16%, p = 0.001, and 54% vs 19%, p < 0.001, respectively).
Characteristics of patients with and without SLE

Values are expressed as n (%) or median (minimal–maximal range).
Mean (SD).
ESRD: end-stage renal disease; SLE: systemic lupus erythematosus. Boldface values represent significant p values.
Early postoperative complications
Overall, postoperative complications occurred more frequently in SLE patients, with 82 (43%) patients presenting any complication compared to 58 (30%) without SLE (p = 0.01). Median time to development of any complication was three days after surgery in both groups. No significant differences were found in the occurrence of infectious or noninfectious complications considered individually. A tendency for more infectious complications was observed in 58 (30%) of SLE patients compared to 41 (21%) of non-SLE patients (p = 0.06), while noninfectious complications were present in 33 (17%) and 24 (13%), p = 0.25, respectively. More than one complication (infectious or noninfectious) was present in 21 (11%) of SLE patients and in 13 (7%) of non-SLE patients (p = 0.20).
No difference between groups was found in the percentage of patients who developed septic shock as a consequence of an infection (5% in SLE vs 4% in non-SLE, p = 0.62). The most frequent infectious complication was abdominal sepsis in both groups, present in 8% of all patients, and no differences were observed in specific sites of infections. Escherichia coli was the most common microbiological agent identified in patients with SLE suffering postoperative infections.
Acute kidney injury was the most frequent non-infectious complication, present in 5% of SLE patients vs 4% of non-SLE (p = 0.81), and no differences were found between specific noninfectious complications except for hypocalcemia (absent in SLE patients vs 5% of non-SLE, p = 0.01). Table 3 shows specific infectious and noninfectious complications.
Univariate logistic regression analysis for any postoperative complication identified anemia (OR 2.93, 95% CI 1.84–4.67, p < 0.001), hypoalbuminemia (OR 3.59, 95% CI 2.18–5.89, p < 0.001), lymphopenia (OR 2.82, 95% CI 1.83–4.37, p < 0.001) and Charlson comorbidity index (OR 0.98, 95% CI 0.97–0.99, p = 0.03) as variables associated with any complication in SLE patients. These variables, except Charlson Comorbidity Index, were retained in the multivariate analysis: anemia (OR 2.01, 95% CI 1.19–3.39, p = 0.008), lymphopenia (OR 2.3, 95% CI 1.44–3.72, p = 0.001) and hypoalbuminemia (OR 2.57, 95% CI 1.49–4.43, p = 0.001).
Prednisone use (OR 1.81, 95% CI 1.13–2.90, p = 0.01), anemia (OR 2.43, 95% CI 1.45–4.08, p = 0.001), hypoalbuminemia (OR 2.58, 95% CI 1.55–4.3, p < 0.001) and lymphopenia (OR 2.43, 95% CI 1.52–3.89, p < 0.001) were variables associated with infectious complications in SLE patients (univariate logistic regression). Lymphopenia (OR 2.19, 95% CI 1.31–3.64, p = 0.002), hypoalbuminemia (OR 1.90, 95% CI 1.08–3.34, p = 0.025) and anemia (OR 1.88, 95% CI 1.05–3.37, p = 0.032) were retained as variables independently associated with these complications in the multivariate analysis.
Univariate logistic regression analysis for noninfectious complications in SLE patients also identified anemia and hypoalbuminemia (OR 1.93, 95% CI 1.03–3.64, p = 0.03, and OR 2.11, 95% CI 1.16–3.86, p = 0.01, respectively), and only hypoalbuminemia (OR 2.08, 95% CI 1.12–3.86, p = 0.02) was independently associated with these complications according to the multivariate analysis.
Mortality
Eleven patients (6%) with SLE died during the postoperative period, compared with two (1%) non-SLE patients (p = 0.02). The median of days from surgery to death was four (1–25) in SLE patients and six (1–10) in non-SLE patients (p = 1.00). Causes of death in the 11 patients with SLE were: septic shock in four, acute myocardial infarction in three, hemorrhagic shock in three, and acute liver failure due to hepatitis A infection in one. Septic shock was the cause of death in the two non-SLE patients.
SLE patients with and without postoperative complications
Characteristics of SLE patients with and without postoperative complications
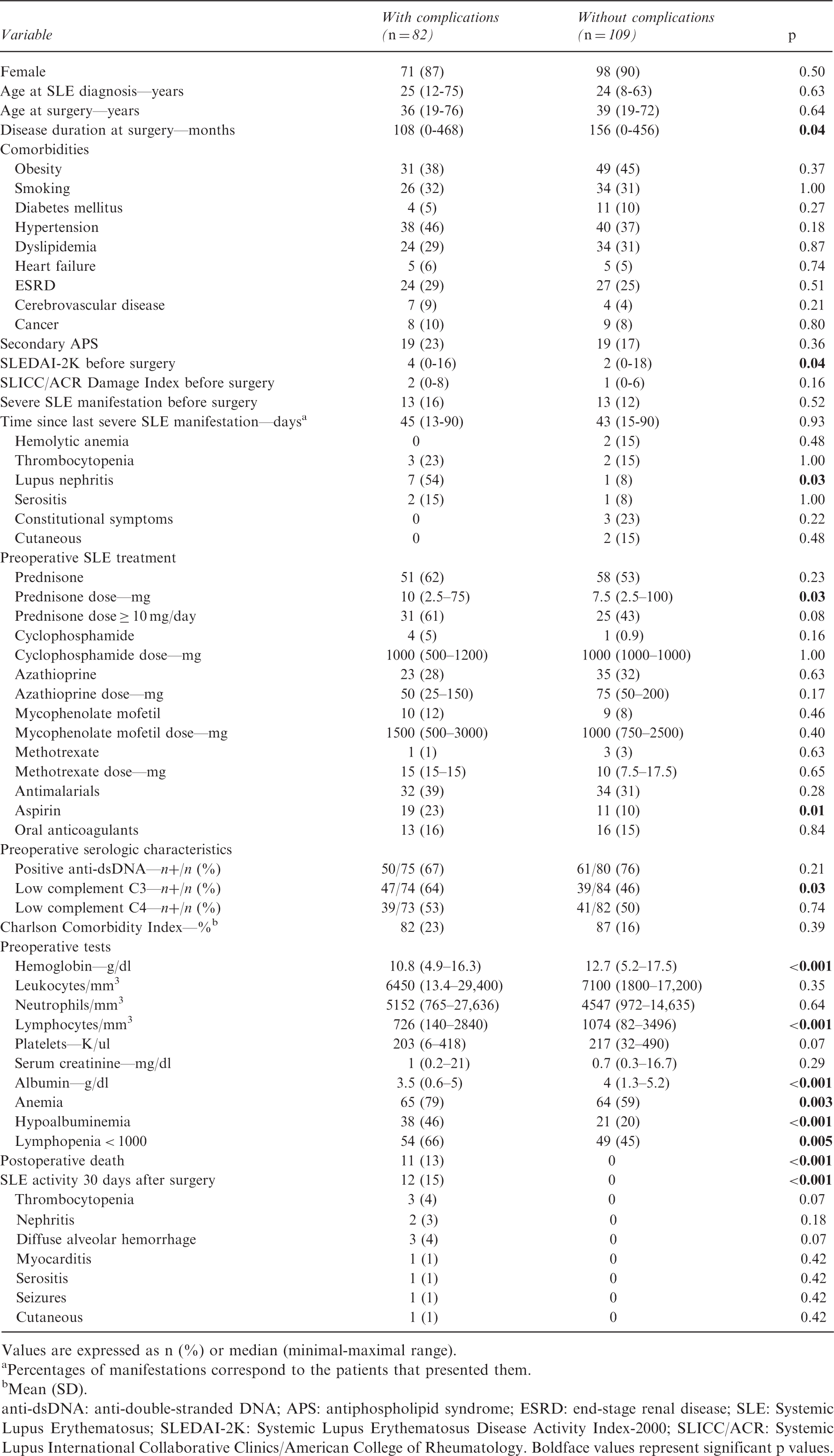
Values are expressed as n (%) or median (minimal-maximal range).
Percentages of manifestations correspond to the patients that presented them.
Mean (SD).
anti-dsDNA: anti-double-stranded DNA; APS: antiphospholipid syndrome; ESRD: end-stage renal disease; SLE: Systemic Lupus Erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index-2000; SLICC/ACR: Systemic Lupus International Collaborative Clinics/American College of Rheumatology. Boldface values represent significant p values.
Univariate regression analysis of patients with SLE and any complication showed an association with preoperative SLEDAI-2K (OR 1.1, 95% CI 1.01–1.20, p = 0.02), lupus nephritis in the previous 90 days (OR 10.08, 95% CI 1.21–83.63, p = 0.03), aspirin use (OR 2.68, 95% CI 1.19–6.02, p = 0.01), preoperative low C3 (OR 2.00, 95% CI 1.06–3.80, p = 0.03), anemia (OR 2.68, 95% CI 1.39–5.18, p = 0.003), hypoalbuminemia (OR 3.49, 95% CI 1.83–6.66, p < 0.001) and lymphopenia (OR 2.36, 95% CI 1.30–4.26, p = 0.004). Multivariate analysis only retained aspirin use as an independent variable (OR 4.35, 95% CI 1.32–14.30, p = 0.01).
Comparative analysis of SLE patients undergoing elective and nonelective procedures
Characteristics of SLE patients with elective and nonelective surgeries
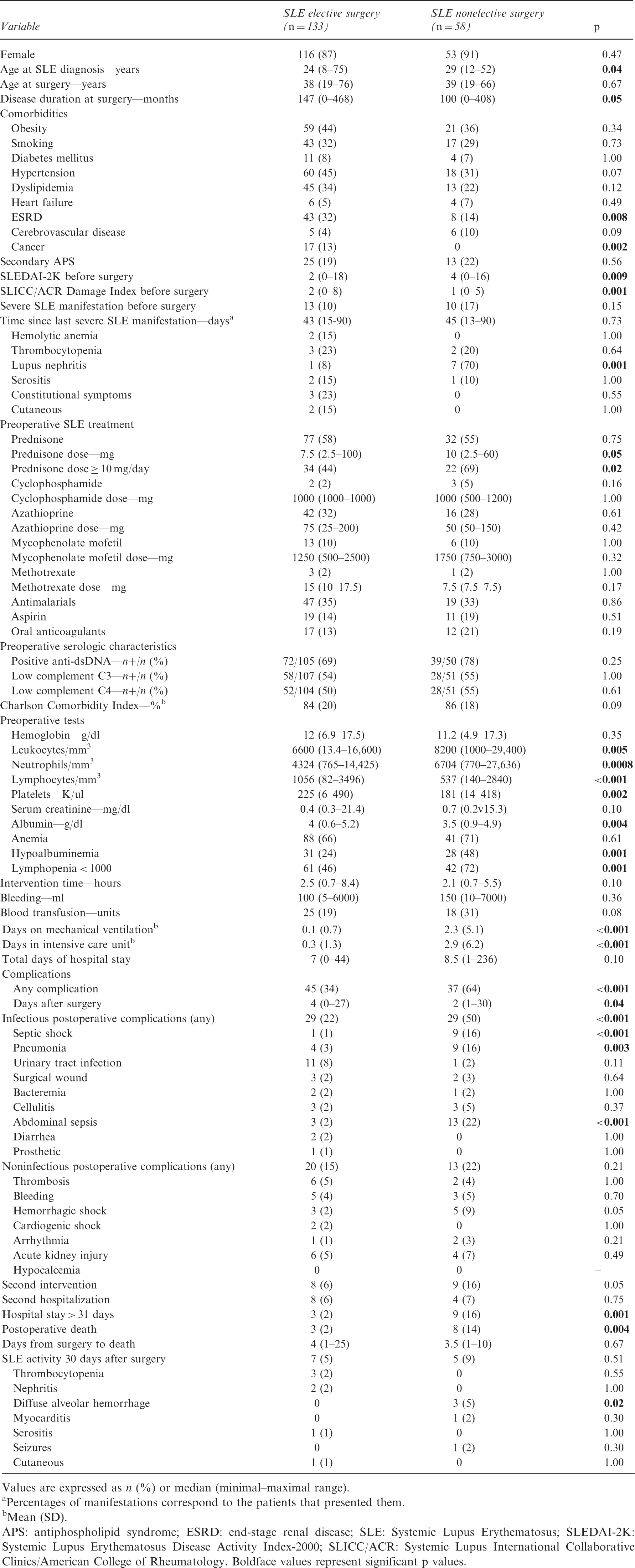
Values are expressed as n (%) or median (minimal–maximal range).
Percentages of manifestations correspond to the patients that presented them.
Mean (SD).
APS: antiphospholipid syndrome; ESRD: end-stage renal disease; SLE: Systemic Lupus Erythematosus; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index-2000; SLICC/ACR: Systemic Lupus International Collaborative Clinics/American College of Rheumatology. Boldface values represent significant p values.
In multivariate analysis, SLEDAI-2K (OR 1.18, 95% CI 1.02–1.36, p = 0.02); SLICC/ACR DI (OR 0.54, 95% CI 0.33–0.90, p = 0.01); pneumonia (OR 11.71, 95% CI 1.75–78.39, p = 0.01); death (OR 14.73, 95% CI 1.19–182.49, p = 0.03); abdominal sepsis (OR 1.38, 95% CI 1.05–1.81, p = 0.01), and days on mechanical ventilation (OR 10.70, 95% CI 1.49–76.83, p = 0.01) were variables independently associated with nonelective procedures in SLE patients.
Discussion
In this study, we analyzed the frequency of early postoperative infectious and noninfectious complications in SLE patients who underwent major noncardiac surgery, and compared them with patients without connective tissue disorders. SLE patients exhibited greater morbimortality, mainly in nonelective procedures, in association with variables related to the disease (activity, measured by SLEDAI-2K), treatment (use of aspirin) and laboratory parameters (hypoalbuminemia, lymphopenia and anemia).
The frequency of any postoperative complication in SLE and non-SLE patients was 43% and 30% respectively in our study, as opposed to 8.9% and 6.6% previously reported in a Taiwanese study. 1 In this latter study, SLE patients showed more comorbidities and higher risk of pneumonia and bacteremia than controls, but lower mortality (0.8%) compared to the one we reported (6%). One possible explanation for these results could be that our cohort had a higher prevalence of hypertension (41% vs 19.6%), dyslipidemia (30% vs 6%), end-stage renal disease (27% vs 5.9%) and cerebrovascular disease 6% vs 2.3%) compared with the Taiwanese cohort, variables that could have accounted for a higher frequency of postoperative complications in our patients. Although in our cohort the SLEDAI-2K was low (median of two points) and only 12% of the SLE patients had a severe clinical manifestation in the 90 days before surgery, these variables could have affected as well more postoperative complications. Another reason for more complications in our cohort compared to the Taiwanese cohort is that we included urgent and emergent major surgeries.
Michaud et al. 15 described early complications (30-day postoperative) in a cohort with osteoarthritis (OA) and rheumatoid arthritis (RA) patients who underwent elective total joint replacement. They reported that 6.6% of RA patients experienced any complication, compared to 34% of our patients who underwent elective surgery. Moreover, 4.5% of the RA patients returned to the operating room, meanwhile 6% of our SLE patients had a second intervention. On the other hand, Yong et al. 16 compared diabetic and nondiabetic patients who underwent major surgery. At six months' follow-up, diabetic patients experienced 9% mortality and 16% readmission. These results contrast with the 6% of mortality and readmission in our cohort at 30 days, showing the impact of SLE on postoperative outcomes compared to other chronic diseases.
The frequency of specific infectious and noninfectious complications was not different among patients with and without SLE despite the differences in the preoperative treatment among groups (use of corticosteroids and immunosuppressants in SLE patients). Previous studies have identified the use of corticosteroids in SLE patients as a risk factor for postoperative complications, 1 a finding that in our study was significant only in the univariate regression analysis of infectious complications. In a previous study of SLE patients who underwent cardiac surgery at our center, the use of corticosteroids was not associated with postoperative complications either. 17
There was a higher frequency of preoperative use of aspirin and oral anticoagulants in SLE patients, without impact on the amount of bleeding or blood transfusion requirements, similar to previous findings in non-SLE patients undergoing surgery. 18 However, aspirin use was independently associated with the presence of any postoperative complication in our SLE patients. Other studies have shown greater risk of bleeding and renal failure, with no differences in cardiovascular events in patients receiving preoperative low-dose aspirin compared to placebo in noncardiac surgery. 19
Differences in the Charlson Comorbidity Index may be explained by the fact that it considers the presence of connective tissue disease and because of a higher frequency of comorbidities in SLE patients (hypertension, dyslipidemia and cerebrovascular disease), which possibly accounted for a higher early postoperative mortality. Previous studies have described the correlation between this index and complications such as blood transfusion requirements, hospital stay and mortality in patients undergoing orthopedic procedures and other major surgeries.20,21
Studies that analyzed postoperative outcomes in SLE patients undergoing orthopedic surgery (hip joint replacement), compared to patients with OA, described higher use of corticosteroids and Charlson Comorbidity Index, higher rate of major and minor adverse events, and longer hospital stay in SLE patients, SLE being an independent risk factor for development of any complication. 22 Furthermore, a recent retrospective study comparing SLE patients to patients with OA and RA undergoing hip joint replacement found a significantly higher rate of postoperative complications (especially early complications) in SLE (36.2%), compared to OA (5.1%) and RA (15.5%) patients. Having SLE and a decrease in postoperative hemoglobin were variables independently associated with complications. 23
Hypoalbuminemia was identified as a risk factor associated with early complications (infectious and noninfectious) in SLE patients, as opposed to previous studies including SLE patients that have not described this finding.1,7,17 In studies evaluating patients without connective tissue disease undergoing major surgery, however, hypoalbuminemia has been identified as a risk factor for infectious postoperative complications, longer hospital stay, higher blood transfusion requirements, rehospitalization, second intervention, and mortality.23–27 Moreover, hypoalbuminemia has been used as a serum marker of malnutrition, and the latter has been related to worse general condition including more comorbidities, older age, lower immune response, muscle wasting, poor cardiac function, low weight and sepsis.25,26 Some of these factors could have accounted for the adverse postoperative outcomes in our patients.
Lymphopenia in SLE is associated with disease activity and is mediated via several mechanisms such as antilymphocyte antibodies, increased complement expression and apoptosis.28,29 In this study, lymphopenia was associated with development of any postoperative complication and with infectious complications. However, this does not seem to be exclusive to SLE, since previous studies in patients without SLE undergoing cardiac surgery identified preoperative lymphopenia as a prognostic factor for postoperative morbimortality. 30 It is suspected that as in human immunodeficiency virus patients, lymphopenia mediated by the aforementioned mechanisms predisposes SLE patients to infections, as was described in an early SLE cohort by Ng et al. 31 Furthermore, corticosteroids inhibit migration and accumulation of leukocytes, bactericidal activity, Fc receptor binding, and redistribution of lymphocytes to various tissue compartments. In the Ng et al. cohort, however, immunosuppressive therapies and corticosteroids did not appear to confer excessive infective risk and did not make a difference in lymphocyte count. 31
Preoperative risk assessment according to type of procedure (low, intermediate or high-risk) did not affect the postoperative outcome. Elective vs nonelective procedures, however, marked several differences in patients with SLE. Patients who underwent nonelective procedures (mainly small intestine surgeries), showed higher disease activity but lower damage accrued, compared to patients who underwent elective procedures (mainly kidney transplant, hystero-oophorectomy, and joint replacement), a finding that reflects the effect of disease duration and treatment on the type of procedures.
Our study has certain limitations. First are its retrospective design and the inclusion of patients who belong to a tertiary care center, with a more severe spectrum of disease. Second, not all patients with SLE who underwent surgery during that period of time were included because of the lack of proper controls for specific procedures such as joint replacements. Third is the consideration that our center is a teaching hospital and sufficient information regarding who performed the surgery was not available. The strengths of our study include the large number of SLE patients; the analysis of variables related to SLE (clinical and serologic characteristics, treatment, activity and damage); a comprehensive preoperative risk assessment; evaluation of postoperative complications, and the inclusion of a control group without connective tissue disease.
Conclusions
Patients with SLE have more frequency of early postoperative complications and mortality compared to patients without SLE undergoing the same type of surgery. The effect of aspirin use, preoperative hypoalbuminemia, anemia and lymphopenia as risk factors for early complications, as well as the prognostic value of the Charlson Comorbidity Index in SLE patients deserve to be analyzed in prospective studies to design a preoperative risk-assessment scale specific for patients with systemic autoimmune diseases undergoing major surgery.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.