
Abstract
Objective
The objective of this paper is to assess overactive bladder (OAB) symptom bother (SB) and health-related quality of life (HRQL) among patients with systemic lupus erythematosus (SLE) and primary Sjögren syndrome (pSS).
Methods
We recruited adult SLE and pSS patients and two groups of age- and sex-matched controls. We applied the OAB questionnaire-short form (OABq-SF) to all participants to assess SB and HRQL and collected clinical information relevant for OAB. We compared the OABq-SF scores for SB and HRQL between patients and controls using univariate and multivariate linear regression analysis.
Results
We recruited 95 rheumatic patients (68 SLE, 27 pSS) and 231 controls. Compared to controls SLE patients showed higher OABq-SF SB scores (22.6 ± 20.4 vs 14.7 ± 17.0, p = 0.004) and lower HRQL scores (89.8 ± 15.8 vs 93.8 ± 11.4, p = 0.044). On multivariate analysis SLE was significantly associated with a higher SB score (ß-coefficient 7.13, p = 0.008) and tended to be associated with worse HRQL values (ß-coefficient –3.53, p = 0.055). Patients with pSS had numerically higher mean SB scores (22.8 ± 22.5 vs 16.2 ± 18.0, respectively, p = 0.107) and lower HRQL scores (91.0 ± 10.7 vs 93.2 ± 11.6, respectively, p = 0.369), although these differences were not statistically significant. Diagnosis of pSS was not significantly associated with SB or HRQL scores on univariate or multivariate analysis.
Conclusions
Patients with SLE have significantly worse OAB-SB and poorer HRQL compared to controls. A similar trend was seen for pSS patients, especially for SB. These findings suggest that clinically subtle OAB symptoms may be present in rheumatic patients for whom, later on, bladder pain syndrome may occur.
Keywords
Introduction
The aetiology of bladder pain syndrome (BPS) remains uncertain, and this entity probably comprises a heterogeneous group of patients that should be managed differently according to individual profiles. The unknown mechanisms may account for at least part of the frequently observed treatment failures, most likely due to therapy off-targeting rather than to subtherapeutic effective treatments. 1 Further knowledge of clinically relevant associations should allow for future patient stratification along with the possible use of urine or serum biomarkers that represent an important research priority towards effective patient-tailored therapies.
Patient self-reported symptoms have shown significant overlap between BPS and overactive bladder (OAB), suggesting that these may both represent different conditions under the same spectrum of bladder hypersensitivity. 2 While the latter is considered a benign, treatable condition, although with significant impact on patients’ quality of life, the former represents a dysfunctional sensory process due to central sensitization and a systemic, self-perpetrated, painful condition. 3 Storage lower urinary tract symptoms (LUTS) assessment in patients suffering from possible associated diseases may help to identify individuals at risk for BPS and to treat them according to their initial noxious stimuli, thus preventing central sensitization from ensuing.
An association between immune-mediated rheumatic diseases and BPS has been suggested in the literature 4 but the small numbers and lack of validated scales have usually yielded low evidence levels. 5 Primary Sjögren syndrome (pSS) patients are likely to present both with OAB symptoms (frequency, nocturia, urgency) and urodynamic abnormalities (such as detrusor overactivity) although further studies are needed to confirm these findings. 6 Case reports on this subject often reveal severe cases of bladder involvement requiring aggressive immunosuppressive treatment strategies. 7 Lupus cystitis has been described as a possible manifestation of systemic lupus erythematosus (SLE), and in a recent large, retrospective study it was strongly associated with lupus mesenteric vasculitis and poorer disease outcomes. 8 There is, however, a lack of data concerning LUTS in these patients when compared to the general population and no firm conclusions can thus be drawn.
In accordance with the potential role of immune-mediated mechanisms in the pathogenesis of BPS, promising data have recently emerged suggesting the efficacy both of immunotherapy 9 and immunosuppressant 10 agents for the treatment of this condition.
Based on these premises, our main goal was to assess OAB symptom bother (SB) and health-related quality of life (HRQL) among patients with SLE and pSS in comparison with controls.
Materials and methods
In a cross-sectional study, we recruited SLE and pSS patients aged 18 or older and able to provide informed consent, who were followed in two different hospital outpatient clinics and who fulfilled the 1997 American College of Rheumatology (ACR) revised criteria for SLE 11 or the American-European Consensus Group criteria for pSS, 12 respectively. We recruited age- and sex-matched controls for each of the disease groups from a population of individuals attending a primary health care centre for routine consultations, who did not have any inflammatory or immune-mediated disease. Pregnant women and individuals with a history of urologic instrumentation (e.g. cystoscopy, prostate biopsy) in the previous three months were excluded.
We applied the overactive bladder questionnaire-short form (OABq-SF) to all study participants. The OABq is a grade A recommendation questionnaire for assessing OAB SB and urinary incontinence-related quality of life both in men and women and it has been validated for the Portuguese language. 13 The OABq-SF is composed of two scales (Supporting Information 1): a six-item symptom bother (SB Likert scale) assessing six items between 1 (not at all) and 6 (a very great deal; range 6–36) and a 13-item HRQL Likert scale with 13 items evaluated with the same six possible degrees (from 1, none of the time, to 6, all of the time; range 13–78). Both scores were then transformed into a scale of 0–100, where higher scores represent greater symptom severity and better HRQL. The OABq-SF has recently been demonstrated to have excellent reliability, validity and responsiveness, all similar to the full 33-item original questionnaire, while being less time consuming. 14
We further collected data on relevant medical history, including previous genital or urologic tumours and urinary tract infection (UTI) in the prior three months, and use of drugs potentially associated with LUTS, namely diuretics, oral or inhalable anticholinergics, antidepressants and corticosteroids. All patients were included between January and September 2013 after providing written informed consent. The study was conducted according to the Declaration of Helsinki, as revised in Fortaleza, Brazil, in 2013, and was approved by the Centro Hospitalar Lisboa Norte Ethics Committee.
We compared SB and HRQL scores between patients and controls using the Student T test. To study the association of SLE/pSS and OAB-SB and HRQL scores accounting for potential confounders, we conducted univariate and multivariate linear regression analyses for both of these outcomes. Explanatory variables to be included in the multivariate models included diagnosis and those with a p value less than 0.1 on univariate analysis. Significance level was 0.05. All statistical analysis were conducted using Stata version 12.1 (StataCorp, College Station, TX, USA) and GraphPad Prism® version 5.0a for Mac OS X (GraphPad Software, San Diego, CA, USA).
Results
Baseline characteristics of patients and healthy controls
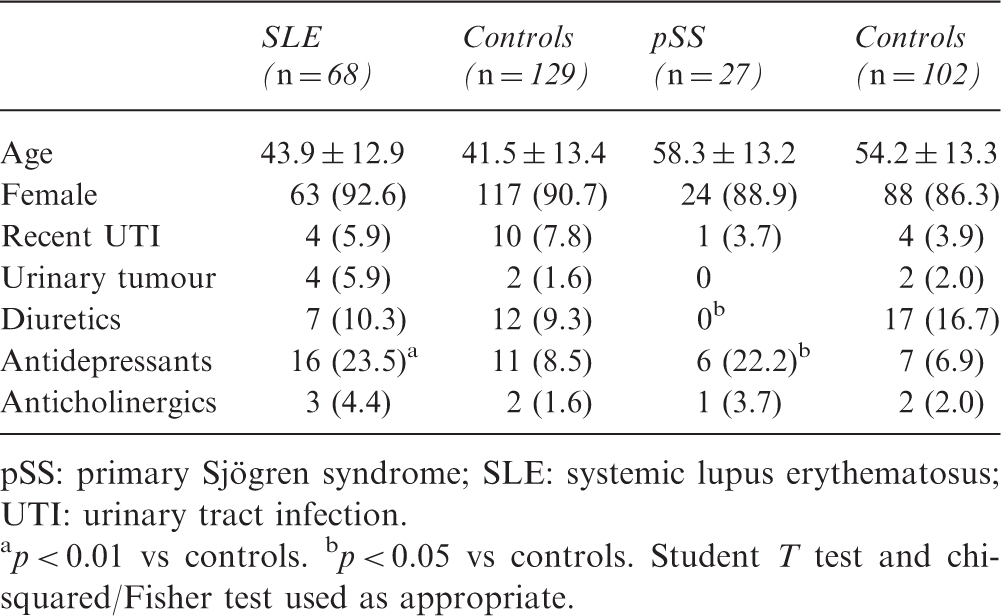
pSS: primary Sjögren syndrome; SLE: systemic lupus erythematosus; UTI: urinary tract infection.
p < 0.01 vs controls. bp < 0.05 vs controls. Student T test and chi-squared/Fisher test used as appropriate.
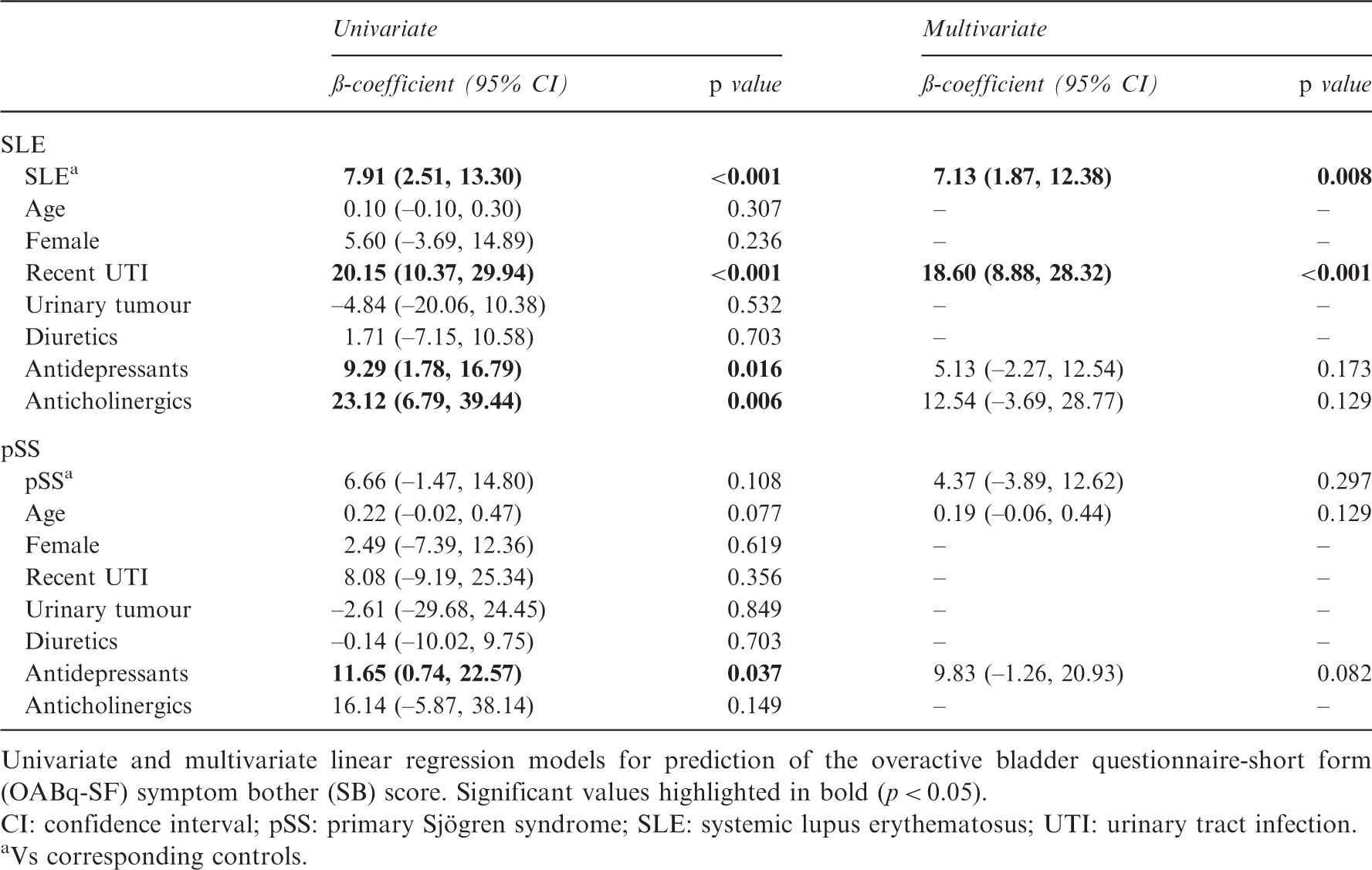
Mean OABq-SF SB scores were significantly higher in the SLE group compared to controls (22.6 ± 20.4 vs 14.7 ± 17.0, respectively, p = 0.004; Figure 1). Patients with pSS had numerically higher mean SB scores, although the difference against controls did not reach statistical significance (22.8 ± 22.5 vs 16.2 ± 18.0, respectively, p = 0.107; Figure 1). For SLE patients, variables associated with OABq-SF SB score on univariate linear regression analysis included a diagnosis of SLE (ß-coefficient 7.91, p < 0.001), recent UTI (ß-coefficient 20.15, p < 0.001) and use of antidepressants (ß-coefficient 9.29, p = 0.016) or anticholinergics (ß-coefficient 23.12, p = 0.006; Table 2). On multivariate analysis, only SLE (ß-coefficient 7.13, p = 0.008) diagnosis and recent UTI (ß-coefficient 18.6, p < 0.001) were independently associated with higher SB score. As for the pSS population, a diagnosis of pSS tended to be associated with SB scores, but did not reach statistical significance on univariate (ß-coefficient 6.66, p = 0.108) or multivariate analysis (ß-coefficient 4.37, p = 0.297). Antidepressants were significantly associated with higher SB score on univariate (ß-coefficient 11.65, p = 0.037) but not on multivariate models (ß-coefficient 9.83, p = 0.082; Table 2).
Boxplot representation of overactive bladder questionnaire-short form scores of symptom bother (a) and health-related quality of life (b). Compared to controls, systemic lupus erythematosus (SLE) and primary Sjögren syndrome (pSS) patients had significantly higher symptom bother scores and worse health-related quality of life. *p < 0.05; **p < 0.01. Linear regression for OABq-SF symptom bother score of SLE and pSS patients Univariate and multivariate linear regression models for prediction of the overactive bladder questionnaire-short form (OABq-SF) symptom bother (SB) score. Significant values highlighted in bold (p < 0.05). CI: confidence interval; pSS: primary Sjögren syndrome; SLE: systemic lupus erythematosus; UTI: urinary tract infection. Vs corresponding controls.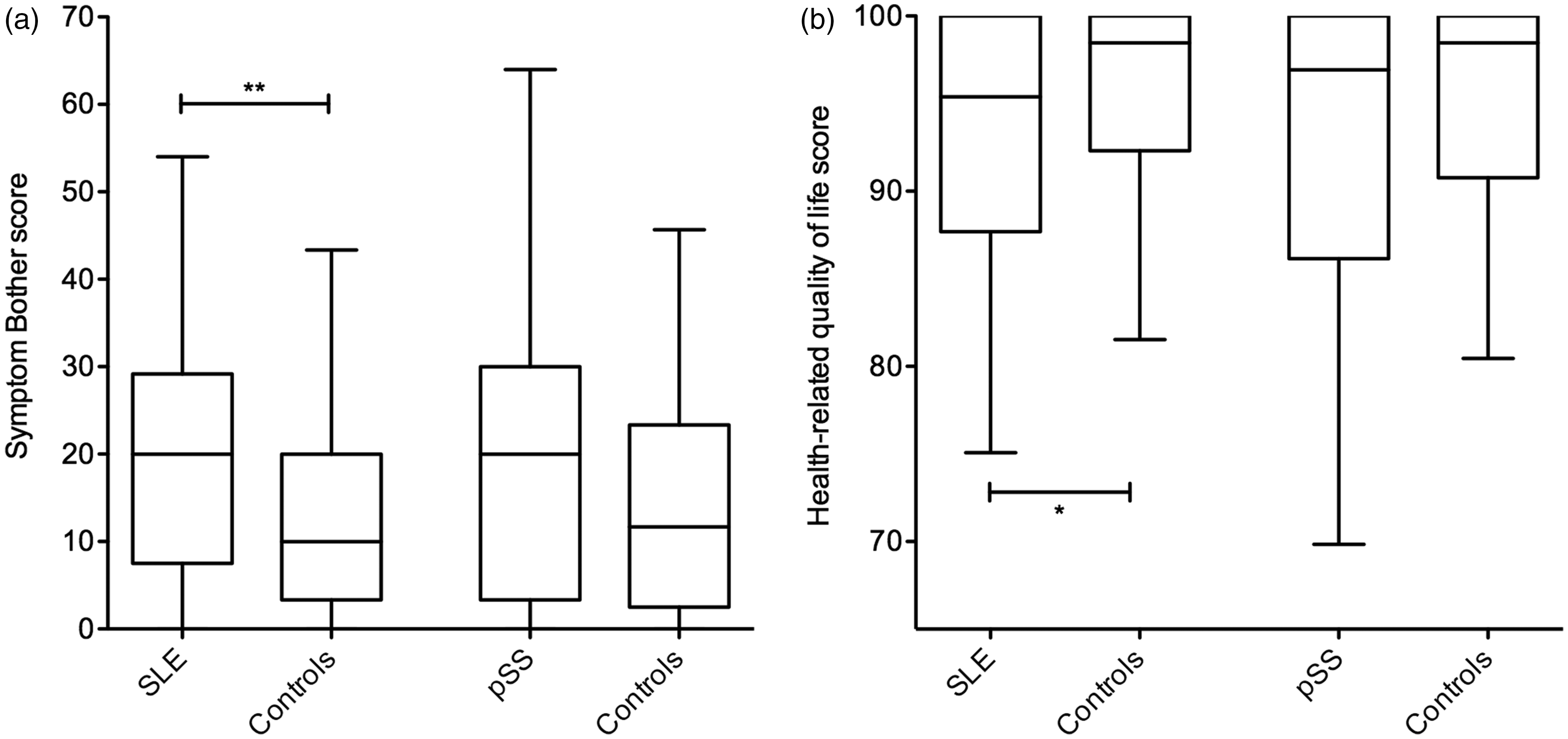
Linear regression for OABq-SF health-related quality of life of SLE and pSS patients
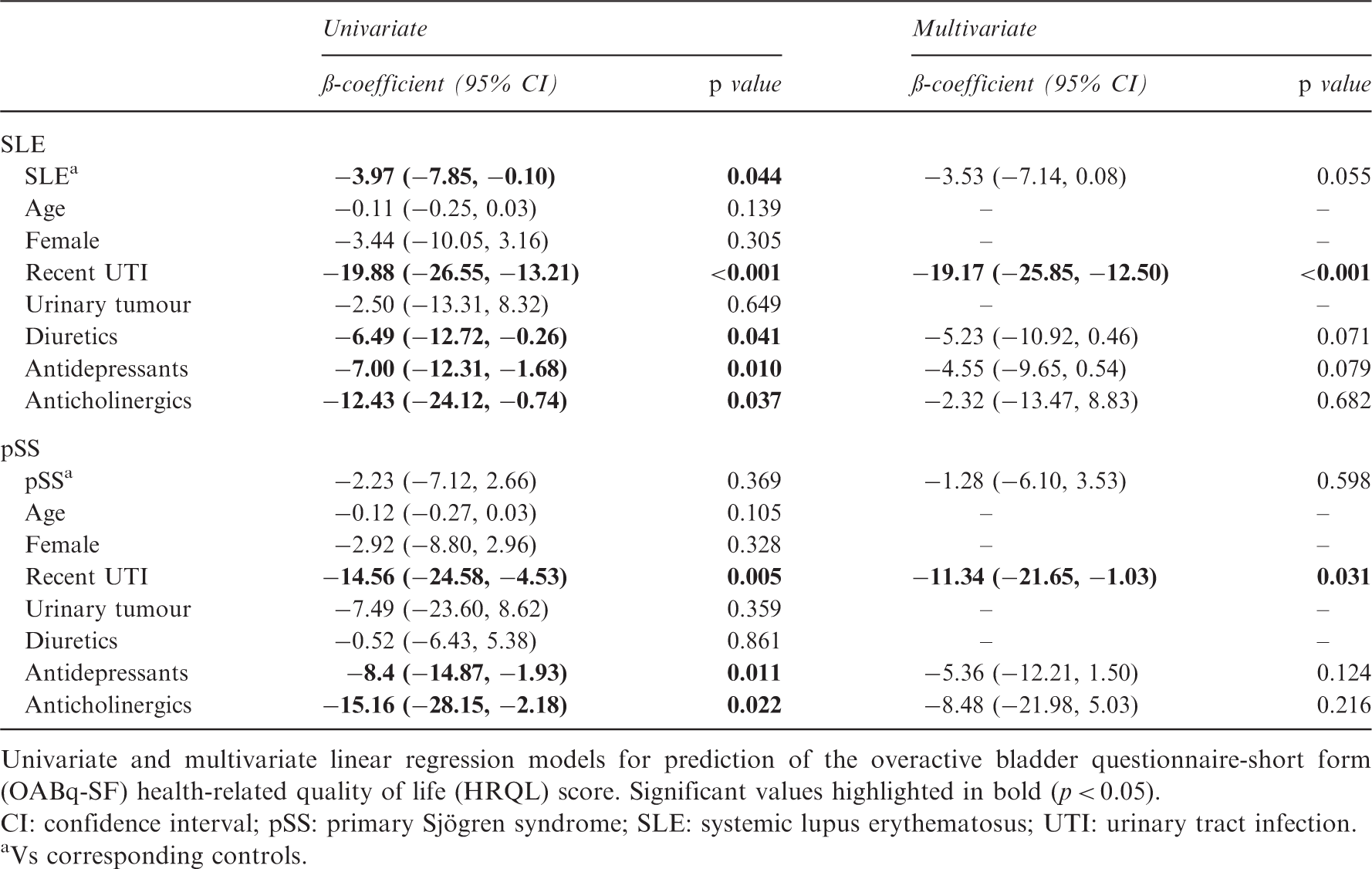
Univariate and multivariate linear regression models for prediction of the overactive bladder questionnaire-short form (OABq-SF) health-related quality of life (HRQL) score. Significant values highlighted in bold (p < 0.05).
CI: confidence interval; pSS: primary Sjögren syndrome; SLE: systemic lupus erythematosus; UTI: urinary tract infection.
Vs corresponding controls.
Discussion
Inflammatory rheumatic diseases have been associated with an increased incidence of BPS. 4 It is likely that OAB symptoms may present earlier in disease course but are eventually overlooked in the setting of clearer rheumatological manifestations until pelvic pain symptoms develop. Thus, OAB complaints will further negatively affect the already poor quality of life of such patients and should, therefore, be addressed at its onset. In our study, the main finding was that SLE patients had worse symptom severity when compared to controls, even when adjusting for other relevant variables. Quality of life was also poorer in SLE patients, although statistical significance was marginally lost in multivariate analysis. On the contrary, we were unable to identify a significant difference in SB and HRQL scores in pSS patients, compared to controls. Importantly, history of recent UTI was strongly associated with worsening of OAB SB and HRQL.
Since our intention was to screen rheumatic patients and healthy controls, no urodynamic assessment was possible to obtain from these patients and so a validated questionnaire was used to measure both SB and HRQL. We chose the OABq-SF mainly for its accuracy in measuring the most important storage LUTS. Furthermore, it had been previously validated for the Portuguese language, which was not the case for other recent questionnaires (e.g. the International Consultation on Incontinence Questionnaire-Female Lower Urinary Tract Symptoms, derived from the Bristol Female Lower Urinary Tract Symptoms-Short Form), demonstrating the importance of questionnaire validation for standardization and comparison of studies.
Other recently published key studies in this field have used nonstandardized questionnaires with a qualitative severity scale, but not addressing storage LUTS, 5 which, in our opinion, should be the main focus in these patients. Quality of life was also not assessed in studies available to date, and the HRQL subscore we applied also helped to shed some light on investigating whether LUTS, when present, do significantly affect quality of life.
Our results confirmed that, indeed, SLE patients have significantly increased OAB SB, as reported by Haarala et al., 5 and that SLE diagnosis is an independent predictor of higher OABq-SF SB scores. Although not statistically significant, a numerical difference was also seen in the degree of SB in pSS patients compared to age- and sex-matched controls. Of note, the mean (22.8/22.6), median (20/20) and distribution of SB scores were very similar in the pSS and SLE populations (Figure 1), suggesting that in these two conditions the impact of OAB SB can be similar. A lower sample size in the pSS population may help to explain the lack of statistical significance observed.
We have also found that OAB-associated HRQL was significantly decreased in SLE patients through application of patient self-reporting tools. When adjusting for other relevant variables, SLE diagnosis tended to be associated with lower HRQL scores, although this was not statistically significant. On the other hand, a smaller, nonsignificant decrease in this outcome was seen in pSS patients, compared to the corresponding control population.
Overall, these findings support the hypothesis that rheumatic patients, especially those with SLE, while being significantly more affected by symptoms, will tend to report them at a later stage, eventually presenting by then with OAB symptoms accompanied by bladder pain and thus being categorized as BPS.
Storage LUTS with varying severity are a common complaint among men and women and sometimes are interpreted as a normal ageing phenomenon. Both in pre- and postmenopausal women, increasing age has been suggested to be associated with more OAB symptoms, 15 a finding, however, that we have failed to confirm. Even though it was not the main focus of our study, this is in accordance with findings from large cohort studies of urodynamics, which have shown that impaired detrusor contractility in women is also more likely to occur at older ages. 16
The main goal of studying LUTS in patients with immune-mediated rheumatic diseases such as SLE does not rely solely on preventing target-organ lesions and the severe consequences for the bladder that lupus cystitis may provoke 17 but it can give us a better understanding of the noxious stimulus that leads to BPS in a subgroup of patients for whom bladder complaints have a large impact on general health. BPS is frequently associated with other medical conditions, many of which may account for chronic inflammation and/or ischaemia (such as hypertension, congestive heart failure, stroke or ischaemic heart disease). 18 Both pSS and SLE may have a role in the establishment of BPS through immune-complex mediated vasculitis as suggested by pathology studies showing granular deposits of immunoglobulin (Ig)G, IgA, IgM, C3 and C1q as well as mononuclear and polymorphonuclear infiltration of blood vessel walls. 19 Serologic abnormalities such as a high rate of positive anti-SSA were described in a series of patients with severe lupus cystitis, 20 also suggesting a possible aetiological link among SLE, pSS and bladder lesions. Even so, the role of anti-SSA on detrusor overactivity is still uncertain. In vivo animal studies based on Ro peptide immunization 21 failed to prove direct anti-SSA muscarinic acetylcholine M3 receptor inhibitory activity as the main mechanism for OAB symptoms in pSS patients, as previously suggested by the induction of OAB features in an animal model through passive transfer of pSS patients’ IgG. 22
It should be highlighted that early screening of SLE and pSS patients for unnoticed or overlooked OAB symptoms may help to identify individuals at risk for the development of BPS before the establishment of a self-perpetrated painful condition, thus preventing severe HRQL impact and further complications in the upper urinary tract. Investigating the aetiological links between these diseases and BPS may also help us to better understand the latter and design more effective treatments that can act at an earlier stage, rather than treating symptomatically a painful end-stage condition for which treatment options are limited.
This study has some important limitations, including its cross-sectional design, which makes it prone to bias as a single assessment was made with no evaluation of progression over time. We have also included a small number of pSS patients, especially compared with the SLE population. We tried to overcome this by including a larger number of controls, but we acknowledge that it may hamper the results obtained and the conclusions to be withdrawn for this condition. Finally, a number of important confounders could have influenced OAB-associated SB and HRQL. We have tried to account for the most important ones by performing multivariate analysis but we are aware that other measurable and unmeasurable variables exist and may influence the associations observed.
Conclusions
This cross-sectional observational study shows that SLE patients report significantly higher OAB SB scores and worse HRQL compared with controls. A similar trend was seen for pSS patients, especially for SB. These findings suggest that clinically subtle OAB symptoms may be present early in the life of rheumatic patients for whom, later on, BPS may occur.
Footnotes
Acknowledgements
The authors would like to thank Carla Macieira, MD, Joaquim Polido-Pereira, MD, Susana Capela, MD, Maria João Saavedra, MD, Rita Barros, MD, and Maria João Gonçalves, MD, for their support in recruiting SLE and pSS patients for this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.