
Abstract
Objective
To investigate the characteristics and associated factors of invasive fungal disease in patients with systemic lupus erythematosus from Southern China.
Methods
A retrospective study was performed. Demographic and clinical characteristics, laboratory data, and radiographic manifestations were recorded.
Results
A total of 45 lupus patients with invasive fungal disease (incidence 1.1%) were included. Twenty-three cases (51.1%) were infected with mold and 22 cases (48.9%) with yeast. Aspergillus spp. (44.4%) and Cryptococcus spp. (33.3%) were common. Aspergillosis mainly occurred in the lung. Cryptococcosis developed in the lung (40.0%), meninges (46.7%) and bloodstream (13.3%). Compared with yeast infection, mold infection tended to develop in patients with active lupus nephritis (65.2% vs. 31.8%, P = 0.03) and the mortality rate was higher (20.0% vs. 0%, P = 0.001). Co-infection with bacteria, virus or superficial fungi occurred in 12 patients (26.7%). Multivariate logistic regression analysis indicated that lymphopenia (odds ratio 2.65, 95% confidential interval 1.14–6.20, P = 0.02) and an accumulated dose of glucocorticoid (odds ratio 1.58, 95% confidence interval 1.10–2.25, P = 0.01) was associated with invasive fungal disease in lupus patients.
Conclusion
Mold infection tended to develop in patients with active lupus disease with high mortality. Co-infection is not rare. Lymphopenia and an accumulated dose of glucocorticoid are associated with invasive fungal disease in lupus patients.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease caused by immune system disorder. Infection remains one of the major threats to lupus patients despite great progress in management.1–23 Invasive fungal disease (IFD) is a long-lasting issue in immunocompromised hosts.4,5 In contrast to patients with HIV or organ transplantation, immune cell dysfunction plays an important role in the development of IFD in lupus patients. 6 In addition, the systemic manifestations of SLE mimic those of IFD, making differential diagnosis difficult. The mortality of IFD remains high.7,8 Some cases were even discovered postmortem because of insufficient vigilance and lack of experience. 8 Until recently, only a few numbers of researches have been published to investigate the situation of IFD in SLE.9–10,11 Studies exploring its clinical spectrum and associated factors are scarce in lupus patients in Southern China.
In this study, we performed a retrospective study in lupus patients with IFD, aiming to investigate the prevalence and characteristics of IFD as well as to identify the factors associated with IFD in patients with SLE from Southern China.
Methods
Study design and patients
We performed a retrospective study on the inpatients from the First Affiliated Hospital of Sun Yat-Sen University from 1 January 2007 to 31 December 2017. The International Classification of Diseases, version 10 (ICD-10) coding of discharged diagnoses was used to identify patients with SLE and IFD (see relevant ICD-10 coding in Supplementary Appendix 1). A total of 4196 inpatients with SLE were selected, among which 60 patients were infected with invasive fungi. The records of the 60 patients were then re-evaluated by a rheumatologist (Minxi Lao) and a respirologist (Haihong Chen). SLE was diagnosed according to the 1997 American College of Rheumatology classification criteria. 12 IFD was determined using the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Group (EORTC/MSG) 2008 guidelines. 13 Eight patients were excluded for misdiagnosis of IFD and seven patients were excluded for incompleteness of data. Finally, 45 patients were included in our research. The ethics committee of the First Affiliated Hospital of Sun Yat-sen University approved the research. This work was conducted according to the provisions of the Declaration of Helsinki.
Definition of cases
IFD was classified into three categories, namely proved, probable, or possible according to the EORTC/MSG 2008 guidelines.
13
A diagnosis of proved IFD required culture or microscopic evidence of the fungi from a normally sterile site. A probable case required the presence of a host factor, mycological evidence (identification of fungal species in respiratory samples (positive twice in microscopic examination and culture of sputum; or positive once in bronchoalveolar lavage fluid); or in a gastrointestinal brushing sample obtained from endoscopy; or identification of fungal antigen in blood (twice elevated serum 1,3-β-
Demographic, clinical, laboratory, radiographic data and therapeutic variables
Demographic and clinical data were collected from medical records. Clinical characteristics of IFD included symptoms and signs, sites of involvement and medication history. Laboratory data included routine blood tests, antinuclear antibodies (ANA), anti-dsDNA antibodies, ESR and serum CRP. ESR, CRP, G-test, galactomannan test and CrAg detection were performed according to the manufacturers' instructions. The systemic lupus erythematosus disease activity index (SLEDAI) was used to evaluate SLE activity. Scores greater than 4 were considered as active SLE. 15 Specimen culture and biopsy findings were recorded if available. Medication history included the daily dose of glucocorticoid and the use of immunosuppressive agents during the three months prior to IFD onset. The dose of glucocorticoid was converted using the following equation: 1 mg of prednisone = 0.8 mg of methylprednisolone = 0.15 mg of dexamethasone.
Statistical analysis
Statistical analysis was performed using SPSS 19.0 (SPSS Inc., Chicago, IL, USA). Continuous data were presented as mean±SD or median (interquartile range; IQR), respectively. Categorical variables were presented as frequency and percentage. Between-group comparison was evaluated with the chi-square test or Fisher's exact test for categorical variables and Student's t-test for continuous variables with normal distribution. Between-group comparison was evaluated using the Mann–Whitney U test for continuous variables with non-normal distribution. Odds ratios (ORs) and corresponding 95% confidence intervals (CIs) of clinically significant variables with a P < 0.1 in between-group comparison were adjusted by multivariate logistic regression analyses to identify the factors associated with IFD. A P value less than 0.05 was considered statistically significant.
Results
Demographic data
IFD was diagnosed in 45 patients (35 women, 10 men) with an incidence of 1.1% (45/4196). All patients were of Chinese Han ethnicity. Of the 45 patients enrolled, the mean age at IFD diagnosis was 37.2 ± 14.3 years (range 14–74 years). The hospital stay from IFD diagnosis to discharge was 24.9 ± 17.0 days. The average SLEDAI score was 5.4 ± 4.3. During the 3 months prior to IFD onset, 35 (77.8%) patients received glucocorticoid treatment. The median (IQR) accumulated dose of glucocorticoid was 1250 mg (490, 2700). Hydroxychloroquine was given to 17 patients. Cyclophosphamide, mycophenolate mofetil (MMF), methotrexate and cyclosporine A (CsA) were prescribed to 13, eight, seven and six patients, respectively. To be specific, cyclophosphamide was administered intravenously (0.5–1.0 g/m 2 monthly). MMF was given to the patients 0.5 g twice a day. Methotrexate was injected 15 mg once a week subcutaneously. The usage of CsA was 3–5 mg/kg/day. Immunosuppressants were discontinued once IFD was diagnosed and glucocorticoid was tapered to the lowest dose that was effective and safe.
Characteristics of mold infection in patients with SLE
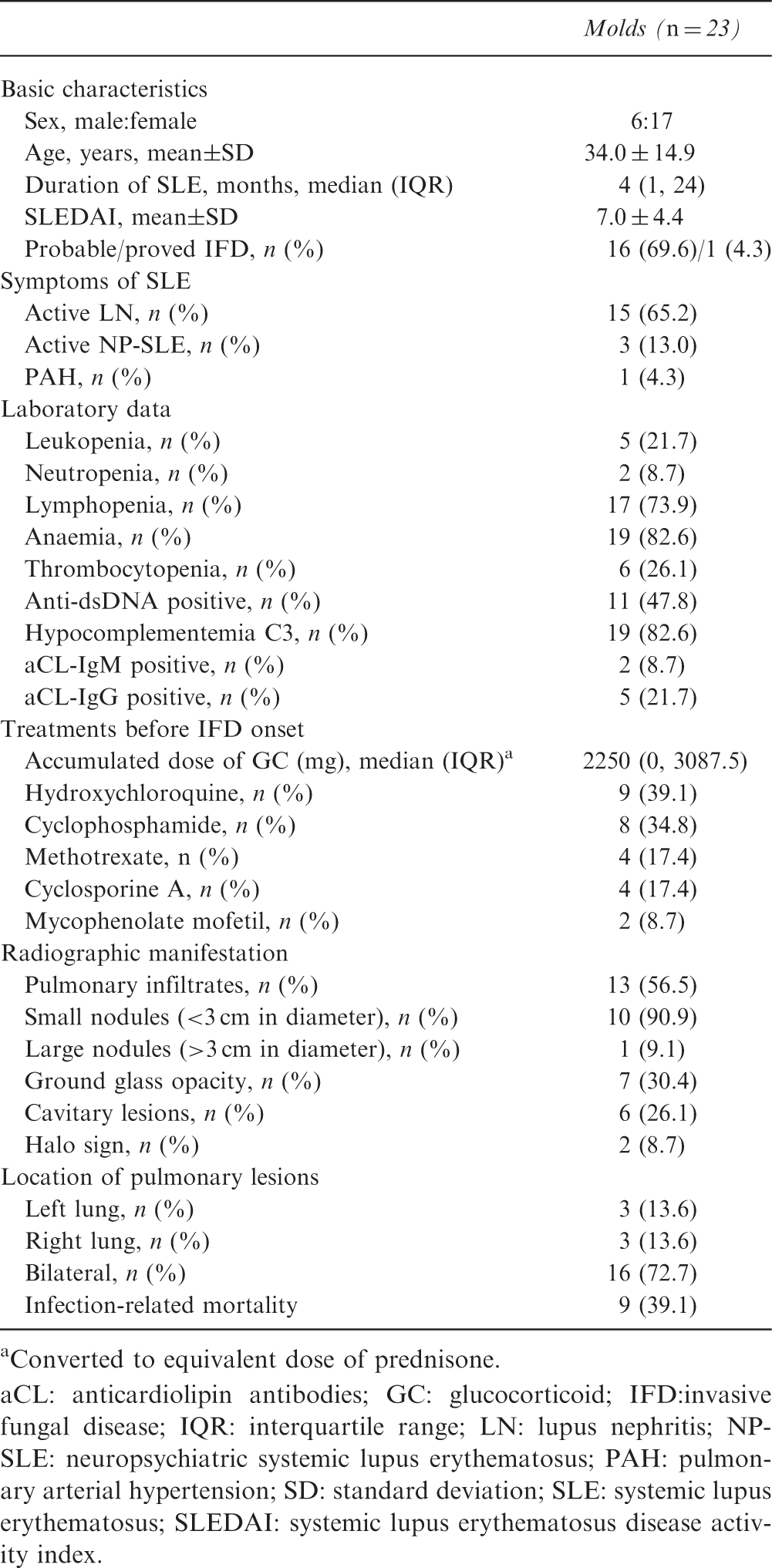
A total of 23 patients were infected by mold. Proved IFD accounted for 4.3% (1/23) of the cases, probable IFD for 69.6% (16/23) and possible IFD for 26.1% (6/23). Molds were identified from sputum culture (n = 15) and bronchoscopic biopsy (n = 1). Causative pathogens included Aspergillus fumigates (n = 7), Aspergillus flavus (n = 1), Aspergillus niger (n = 1), and Penicillium marneffei (n = 2). Co-infection with two kinds of fungi was found in four patients. The median (IQR) duration of SLE at IFD onset was 4 months (1, 24). The average SLEDAI score was 7.0 ± 4.4. Lupus symptoms included active lupus nephritis (LN) (65.2%), haematological disorders (39.1%), neuropsychiatric lupus (NP-SLE) (13%), and pulmonary arterial hypertension (PAH) (4.3%). Clinical symptoms of mold infection included fever (78.3%), cough (69.6%), sputum (60.9%), dyspnoea (30.4%) and haemoptysis (8.7%). The characteristics are shown in Table 1. All the infections occurred in the lungs. Pulmonary lesions mainly presented as infiltrations (56.5%), nodules (47.8%), ground glass opacity (30.4%) and cavitary lesions (26.1%) (Figure 1(a and b)). The halo sign was shown in three cases (8.7%). Most of the nodules (10/11, 90.9%) were small nodules with a diameter less than 3 cm. Nodules with a blurred edge were common (7/11, 63.6%). All the cavitary lesions were eccentric. Bilateral lung involvement was displayed in 16 patients (72.7%). Bronchoscopic biopsy was performed in one patient. Representative images of Aspergillus spp. found in lung tissue are shown in Figure 1(d–f). The serum G-test was performed in 16 patients and was positive in eight (50.0%). The serum galactomannan test was performed in 18 patients and was positive in six (33.3%). Galactomannan was also positive in bronchoalveolar lavage fluid in two patients. Intravenous voriconazole (11/23, 47.8%) was the first-line therapy for mold infection. Other patients were treated with caspofungin (3/23, 13.0%), micafungin (3/23, 13.0%) or itraconazole (3/23, 13.0%). Clinical and radiographic improvement was observed in 14 patients before discharge. Nine patients died of severe mold infection, and the mortality rate was 39.1%. Among the nine non-survivors, LN and NP-SLE occurred in five (66.7%) and two (22.2%) patients, respectively. Aetiological agents included A. fumigates (n = 4), P. marneffei (n = 2) and mixed infection with A. fumigates and Aspergillus nidulans (n = 1). All the patients had lymphopenia. The median dose of accumulated glucocorticoid was 3000 mg (IQR 1500, 3700).
Radiographic manifestation of pulmonary invasive fungal disease (IFD) in patients with systemic lupus erythematosus (SLE). (a) Pulmonary computed tomography (CT) scan showed an intracavitary nodule in the left lung. (b) Bilateral diffused small nodules and patchy infiltrations were shown in the pulmonary CT scan. (c) Pulmonary CT scan showed a consolidation with a cavitation in the left lung. (d) Branched, septate hyphae of Aspergillus spp. were found in lung tissue obtained from bronchoscopic biopsy (red arrow) (haematoxylin and eosin (HE) staining, 200×). (e) Periodic acid–Schiff stain revealed fungal hyphae (red arrows) in the lung tissue (200×). (f) Septate fungal hyphae were stained brown (red arrows) by periodic acid-silver metheramine (PASM) (200×). (g) Histopathological examination of pleura biopsied specimen showed yeast-form fungi (red arrow) (HE staining, 200×). (h) Cryptococci were dyed blue by Alcian blue staining (red arrows) (200×). (i) Cryptococci (red arrows) were seen on PASM staining (red arrows) (200×). Characteristics of mold infection in patients with SLE Converted to equivalent dose of prednisone. aCL: anticardiolipin antibodies; GC: glucocorticoid; IFD:invasive fungal disease; IQR: interquartile range; LN: lupus nephritis; NP-SLE: neuropsychiatric systemic lupus erythematosus; PAH: pulmonary arterial hypertension; SD: standard deviation; SLE: systemic lupus erythematosus; SLEDAI: systemic lupus erythematosus disease activity index.
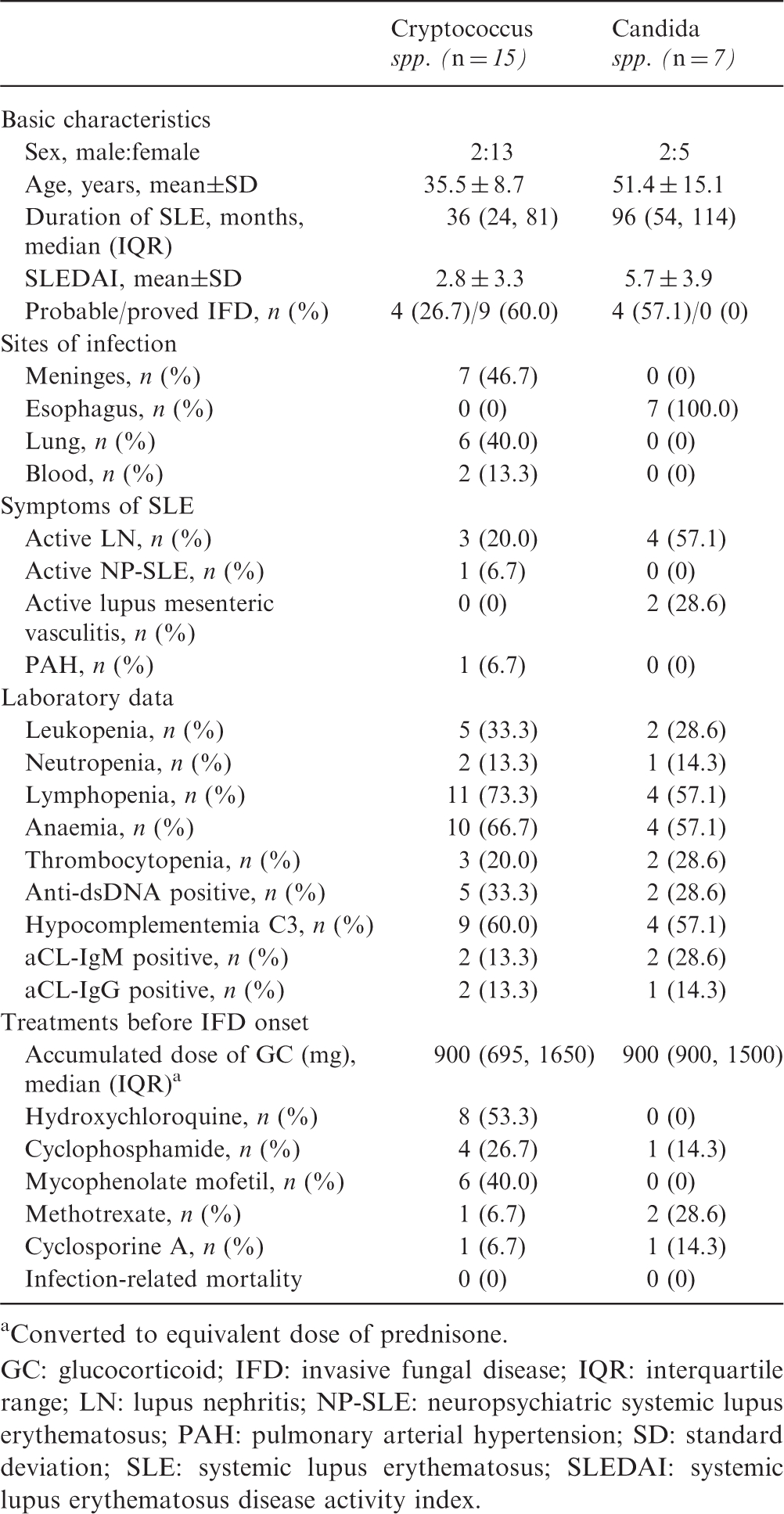
Characteristics of yeast infection in patients with SLE
Characteristics of yeast infection in patients with SLE
Converted to equivalent dose of prednisone.
GC: glucocorticoid; IFD: invasive fungal disease; IQR: interquartile range; LN: lupus nephritis; NP-SLE: neuropsychiatric systemic lupus erythematosus; PAH: pulmonary arterial hypertension; SD: standard deviation; SLE: systemic lupus erythematosus; SLEDAI: systemic lupus erythematosus disease activity index.
Comparison between IFD caused by mold or yeast
A comparison between mold-associated IFD and yeast-associated IFD was performed. The duration of SLE was significantly shorter in patients with mold infection than those with yeast infection (4 months vs. 48 months, P = 0.001). The SLEDAI score was higher in patients infected by mold than those infected by yeast (7.0 vs. 3.7, P = 0.01). Active LN was more frequent in patients with mold infection than those with yeast infection (65.2% vs. 31.8%, P = 0.03). Nine patients (39.1%) died of mold infection while yeast-associated mortality was zero (P = 0.001). The incidence of NP-SLE, PAH, haematological disorders, anti-dsDNA positivity and hypocomplementemia C3 did not differ between the groups.
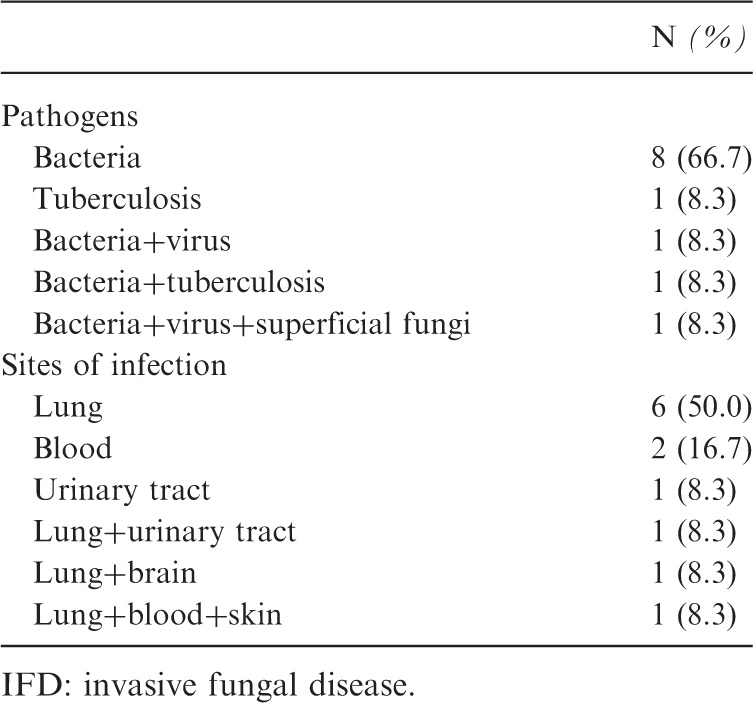
Co-infection with other pathogens in lupus patients with IFD
Co-infection with other pathogens in lupus patients with IFD
IFD: invasive fungal disease.
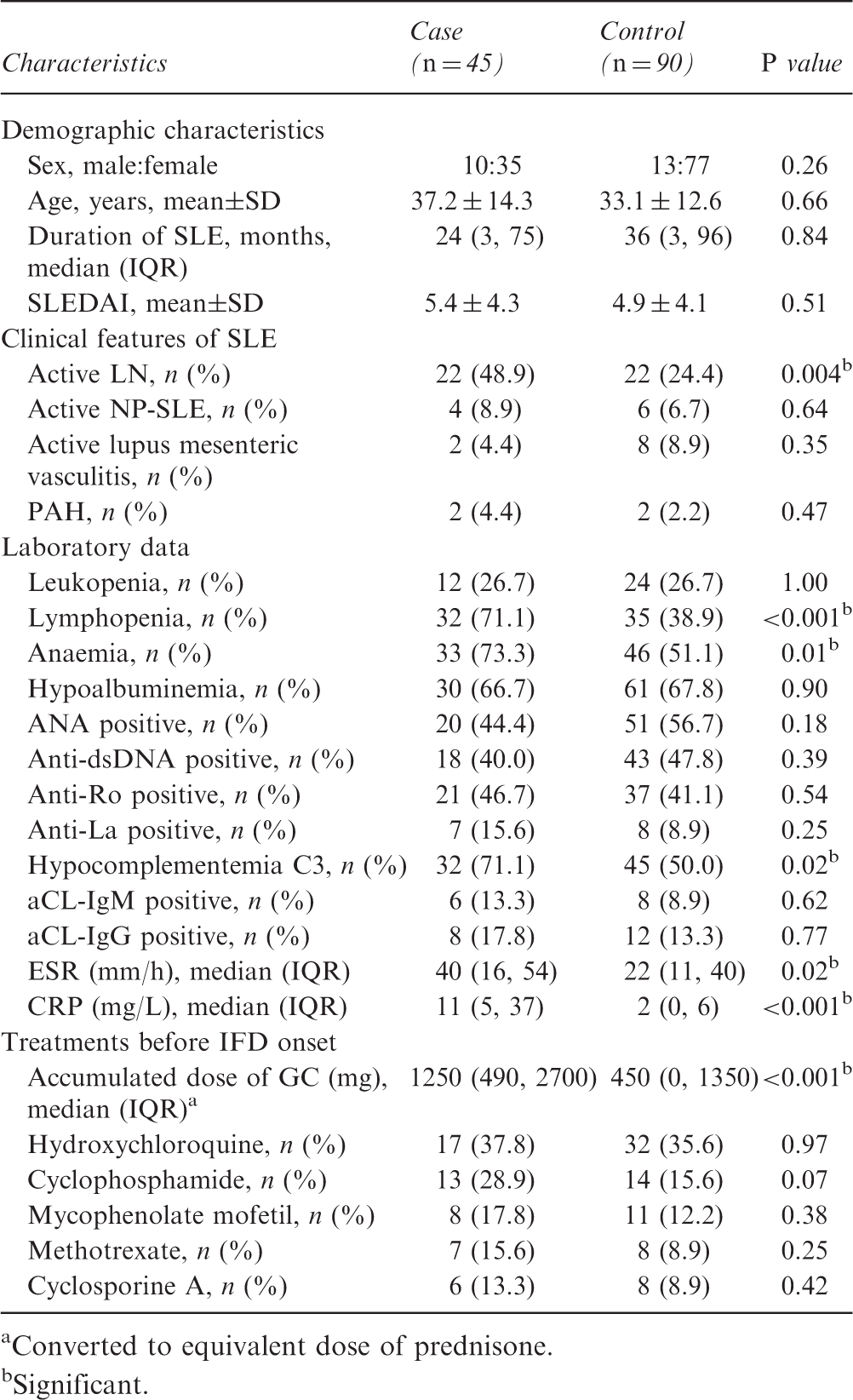
Comparison between IFD and non-IFD in patients with SLE
Comparison between lupus patients with or without IFD
Converted to equivalent dose of prednisone.
Significant.
ANA: anti-nuclear antibodies; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; GC: glucocorticoid; IFD: invasive fungal disease; IQR: interquartile range; LN: lupus nephritis; SD: standard deviation; SLE: systemic lupus erythematosus; SLEDAI: systemic lupus erythematosus disease activity index.
Factors associated with IFD in patients with SLE
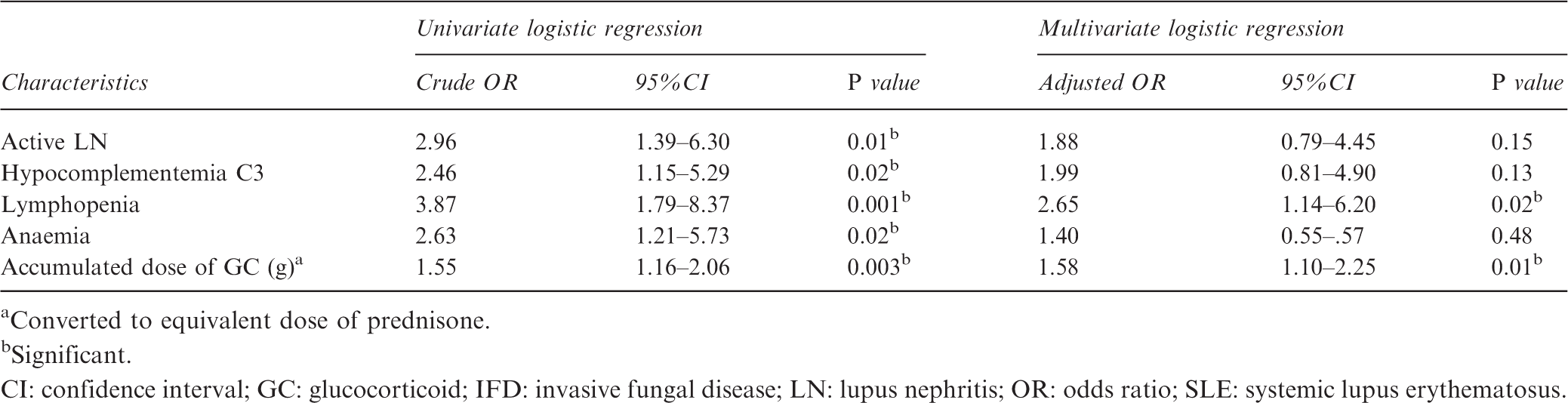
Converted to equivalent dose of prednisone.
Significant.
CI: confidence interval; GC: glucocorticoid; IFD: invasive fungal disease; LN: lupus nephritis; OR: odds ratio; SLE: systemic lupus erythematosus.
Discussion
In this study, we explored the clinical characteristics of IFD in patients with SLE. Our results suggested that Aspergillus spp. and Cryptococcus spp. were the common strains that caused IFD. The mortality of IFD in lupus patients was high. Concomitant infection with bacteria, virus or superficial fungi was not rare. Lymphopenia and an accumulated dose of glucocorticoid were associated with IFD in lupus patients.
In our study, about 1.1% (45/4196) of the lupus patients developed IFD. The incidence was comparable to the current situation in other countries (0.6–3.2%). 16 SLE per se entailing cell-mediated immune disorder was vulnerable to invasive fungal infection. Our results indicated that IFD is a common complication in patients with SLE and could be life threatening. Physicians should be vigilant against IFD, especially aspergillosis and cryptococcosis.
Pneumonia caused by mold accounted for half of the infection in our research (51.1%). Aspergillus spp. was the main agent. All of the mold infection occurred in the lung. Nodules and cavitary lesions were relatively common in radiographic imaging. Although the halo sign and the crescent sign were specific for mold-associated pneumonia, they were seldom found in lupus patients. Our results suggested that the radiographic manifestation of mold infection could be atypical in lupus patients. The mortality (39.1%) in the mold-infected group was high. Nine patients died even though aggressive anti-fungal therapy was applied. Therefore, laboratory tests should be performed as soon as possible for those in whom response to conventional antibiotics was poor. Considering the high mortality rate of mold infection, anti-fungal therapy should be initiated in lupus patients diagnosed with possible IFD if multiple risk factors are found.
Yeast infection could develop in the lung, meninges and digestive tract. In particular, infection by Cryptococcus spp. was common. In our research, cryptococcosis accounted for 33.3% of the IFD. A systemic review of 393 cases from 182 studies identified that 35.4% of the fungal infection was caused by Cryptococcus neoformans in lupus patients. 16 Cryptococcal meningitis was prevalent in lupus patients from Asia. 17 In our research, cryptococcal pneumonia was not rare (6/22, 27.3%). C. neoformans was also detected in the bloodstream in two cases (2/22, 9.1%), leading to disseminated fungal infection. In contrast to mold infection, the prognosis of yeast infection was relatively favourable.
A systemic review showed that approximately 86% of the lupus patients developed IFD during the active disease stage. 16 In recent research, the SLEDAI score was significantly higher in patients with mold infection than those with yeast infection. Active LN, in particular, was prevalent in patients infected by mold. Mortality in the mold-infected group was 39.1% (9/23), significantly higher than that in the yeast-infected group. Our results were inconsistent with a prospective study of 1208 IFD patients from 1063 organ transplant recipients, which found that Aspergillus spp. was more fatal than Candida spp. in immunocompromised hosts. 18 By comparing the basic characteristics, we found that mold infection was more likely to develop during the active disease stage with a poorer prognosis.
Although it is widely recognized that patients receiving broad-spectrum antibiotics are prone to develop IFD, co-infection with other organisms has been poorly studied in lupus patients with IFD. Our research showed that co-infection occurred in 26.7% of the patients. The lung was the most frequently affected organ. About two thirds of the infected cases (66.7%) were bacteria associated. Our results indicated that lupus patients with immune impairment were inclined to develop co-infection with various agents. Physicians should be vigilant against co-infection even though IFD was confirmed.
Many factors were associated with IFD. The toxicity of glucocorticoid is well recognized in SLE. A high dose of glucocorticoid was reported to be associated with the highest crude rate of serious infection in patients with LN. 19 A retrospective study showed that current users of glucocorticoid had a higher risk of developing all types of infection than the non-users. 20 Inconsistently, the accumulated dose of glucocorticoid was remarkably higher in the IFD group than that in the control group in our study. The accumulated glucocorticoid dose was associated with IFD and increased the risk 1.58-fold. Lymphopenia was more predominant in patients with IFD than those in the control group. It increased the development of IFD 2.65-fold. SLE, per se, exerts an inhibitory effect on the generation and function of the lymphocytes. The incidence of lymphopenia, as a pattern of haematological abnormality secondary to SLE, was reported to be 56.4%. 21 Besides, CD4+T cells isolated from lupus-prone mice displayed immune disability against intracellular infection. 22 Both T cells and B cells play critical roles in fungal defence. In particular, T-helper type 1 (Th1) cells by secreting interferon (IFN)-γ and TNF-α activate the innate immune system as well as stimulating B cells to produce fungi-specific antibodies.23,24 The adoptive transfer of CD4+Th1 cells was able to protect haematopoietic stem-cell transplantation patients against aspergillosis. 25 Our results suggested that the lymphocyte count was associated with IFD.
Recently, the protective roles of hydroxychloroquine and antiphospholipid (aPL) antibodies against infection were suggested in lupus patients.26–28 However, our study did not reproduce this trend. In previous research, Asians accounted for only a small proportion of the research subjects. Subgroup analysis revealed that antimalarial users experienced viral infection less frequently than non-users. 20 The beneficial effect of hydroxychloroquine on IFD in lupus patients from China needs further exploration. The positivity of anticardiolipin antibodies (aCL) was slightly higher in patients with IFD than those without in our research, but it was not statistically significant. The mechanism of aPL against infection was not clarified. Further research is needed to verify the possible relation between aPL and IFD.
In this study, we analyzed the situation of IFD in lupus patients from the past 10 years systemically. It could be the study enrolling the largest number of lupus patients with IFD among Chinese research. To the best of our knowledge, this study is the first to compare the characteristics between mold and yeast infection in SLE. However, there are also some drawbacks. As only data from the inpatients were collected, we were not able to provide information regarding the course of antifungal treatment and long-term prognosis.
In conclusion, patients with SLE are at high risk of IFD. Aspergillus spp. and Cryptococcus spp. are the common strains. Mold infection is likely to develop during active disease. Co-infection with other pathogens is not rare. Lymphopenia and accumulated glucocorticoid use are associated with IFD in lupus patients. Screening for IFD and prompt treatment in selective patients is needed.
Supplemental Material
Supplemental material for Invasive fungal disease in patients with systemic lupus erythematosus from Southern China: a retrospective study
Supplemental Material for Invasive fungal disease in patients with systemic lupus erythematosus from Southern China: a retrospective study by M. Lao, X. Wang, M. Ding, Z. Yang, H. Chen, L. Liang, Z. Zhan and D. Chen in Lupus
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this project was supported by grants from the Guangdong Technology Project (2016A020215043) and grants from the National Natural Science Foundation of China (81603435, 81601403).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.