
Abstract
‘Refractory lupus nephritis’ is a frequently used term but poorly defined. We conducted a survey among nephrologists and rheumatologists to spot the diversity of perceptions of this term and to better understand the clinical practice related to ‘refractory lupus nephritis’. A total of 145 questionnaires completed by lupus nephritis experts were available for analysis, of which 52% were nephrologists, 34% rheumatologists, and 13% internists. Response to induction treatment was mostly assessed after six months (58%), but assessment at three months was more common with the use of the EURO lupus protocol than with other treatment protocols. Rheumatologists used urinary sediment to assess response more frequently than nephrologists (66 vs. 48%, p < 0.05, Chi2), while nephrologists conversely relied significantly more on clinical symptoms (61 vs. 31%, p < 0.0001, Chi2). Non-nephrologists quantified proteinuria preferentially by 24 h urine sampling, while the majority of nephrologists relied on the urinary protein/creatinine ratio (UPCR) or the albumin/creatinine ratio of spot urine samples (59 vs. 38%, p < 0.05, Chi2). A total of 91% were concerned about persistent immunological systemic lupus erythematosus activity. There was less concern about drug adherence, renal scarring, genetic factors or other kidney diseases. Less than 20% check for drug adherence by regularly monitoring drug plasma levels. Nephrologists considered a re-biopsy more often than rheumatologists (58 vs. 38%, p < 0.05, Chi2). Together, among lupus nephritis experts there is considerable diversity in the perception of what the term ‘refractory lupus nephritis’ describes and how it is defined. A consensus definition of ‘refractory lupus nephritis’ is needed.
Introduction
Lupus nephritis (LN) is the most frequent organ manifestation of systemic lupus erythematosus (SLE). The diagnosis of LN may be suspected from the combination of hematuria and proteinuria but only a kidney biopsy can identify those patients with proliferative immune complex glomerulonephritis that are at risk for nephron loss and chronic kidney disease (CKD) progressing to end stage renal disease (ESRD). Intense immunosuppression is the treatment of choice to control systemic autoimmunity and intrarenal inflammation, as the major strategy to halt autoimmune injury of the kidney and to improve long term outcomes of disease. In fact, failing to respond to induction therapy with immunosuppressive drugs is associated with an unfortunate long term kidney prognosis and lower overall survival. 1 Current treatment guidelines suggest evaluating the response to immunosuppressive drugs with biomarkers of renal excretory function (serum creatinine level) and renal filtration barrier function (hematuria, proteinuria), but the time point of assessment is not clearly defined.2–4
The term ‘refractory LN’ (RLN) is frequently used in the medical literature in the context of patients with LN not adequately responding to immunosuppressive drugs. The use and understanding of this term varies and currently there is no consensus on its definition. However, defining RLN is clinically important to trigger a diagnostic workup for persistent LN disease activity versus non-adherence, genetic co-factors, e.g. APOL1 risk variants, promoting CKD progression independent of autoimmune disease activity, pharmacogenetics resistance to certain immunosuppressive drugs or concomitant other kidney diseases or renal drug toxicities. 5
The Lupus Nephritis Trials Network (LNTN) is a global network of LN specialists that seeks to develop a consensus definition for RLN to be implemented in future revisions of the current LN guidelines (http://lupusnephritis.org/). As a first step we performed a survey among the LNTN members and other decision takers in patients with LN to determine professional trends in defining and managing RLN in clinical practice.
Methods
Questionnaire and study population
The study was designed according to the international recommendations in the conduct and reporting of survey research. 6 The questionnaire consisted of 13 multiple choice questions in English or German language, structured into four different sections: (A) demographic information, (B) clinical practice in LN, (C) definition of RLN, and (D) clinical practice in the treatment of LN. The original survey is accessible as a supplementary document.
The online questionnaire was realized using LimeSurvey (version 2.06+), which was pre-installed on the server of the University Hospital at Ludwig-Maximilians Universität. The WAD-Support (Stabstelle Webanforderungen und - dienste) provided access to the core survey formula. The WAD-Support enabled the inquiry after meeting the criteria for data security according to the Bavarian law data protection act (Art. 26 BayDSG). LimeSurvey allowed creation of print versions of the survey by exporting queXML files, which were converted into a PDF file. We used open source software queXF, installed on a local host.
A total of 407 physicians were asked to participate in the survey. The 186 members of the LNTN received the link to the online survey twice. In addition, the attendees of the International Society of Nephrology Nexus meeting ‘Translational immunology of kidney disease’, Berlin, 14–16 April 2016 and the participants of the Rheumatology CME course at the ERA-EDTA congress 2016 in Vienna were asked to complete a print version of the same questionnaire. Data collection was open for a four-month period, 23 March–11 July, 2016.
After acquisition, data were transferred from LimeSurvey to Excel to perform a statistical analysis with Excel, Prism and R Studio. Printed questionnaires were scanned and added manually to the LimeSurvey form to provide consistent data quality.
Statistical analysis
Categorical variables were compared using Chi2 tests for the total sample or large subsamples of participants (n > 20) or Fisher's exact tests for smaller subsamples. The Cochran -Armitage test for trend was used to assess associations between a variable with two categories and an ordinal variable with several categories. p values less than 0.05 were considered statistically significant.
Results
The questionnaire was sent to the 186 members of the LNTN and presented to 221 attendees of two international nephrology/rheumatology meetings. Altogether, 171 questionnaires were available for analysis (total return rate 42% [171/407]) with 145 data sets containing answers to all 13 questions (85% of all received questionnaires). The question specific return rates and drop outs for incomplete questionnaires are depicted in Figure 1(a).
Return rates and basic characteristics of participants. (a) Flow chart depicting available answers per question. Final questions on lupus nephritis treatment stratified for ethnicity and line of therapy caused a drop-out of 15%. (b)–(f) Pie charts depicting basic characteristics of study participants, i.e. age of participant, years of clinical experience, number of lupus nephritis patients, country of practice as well as subspecialty training.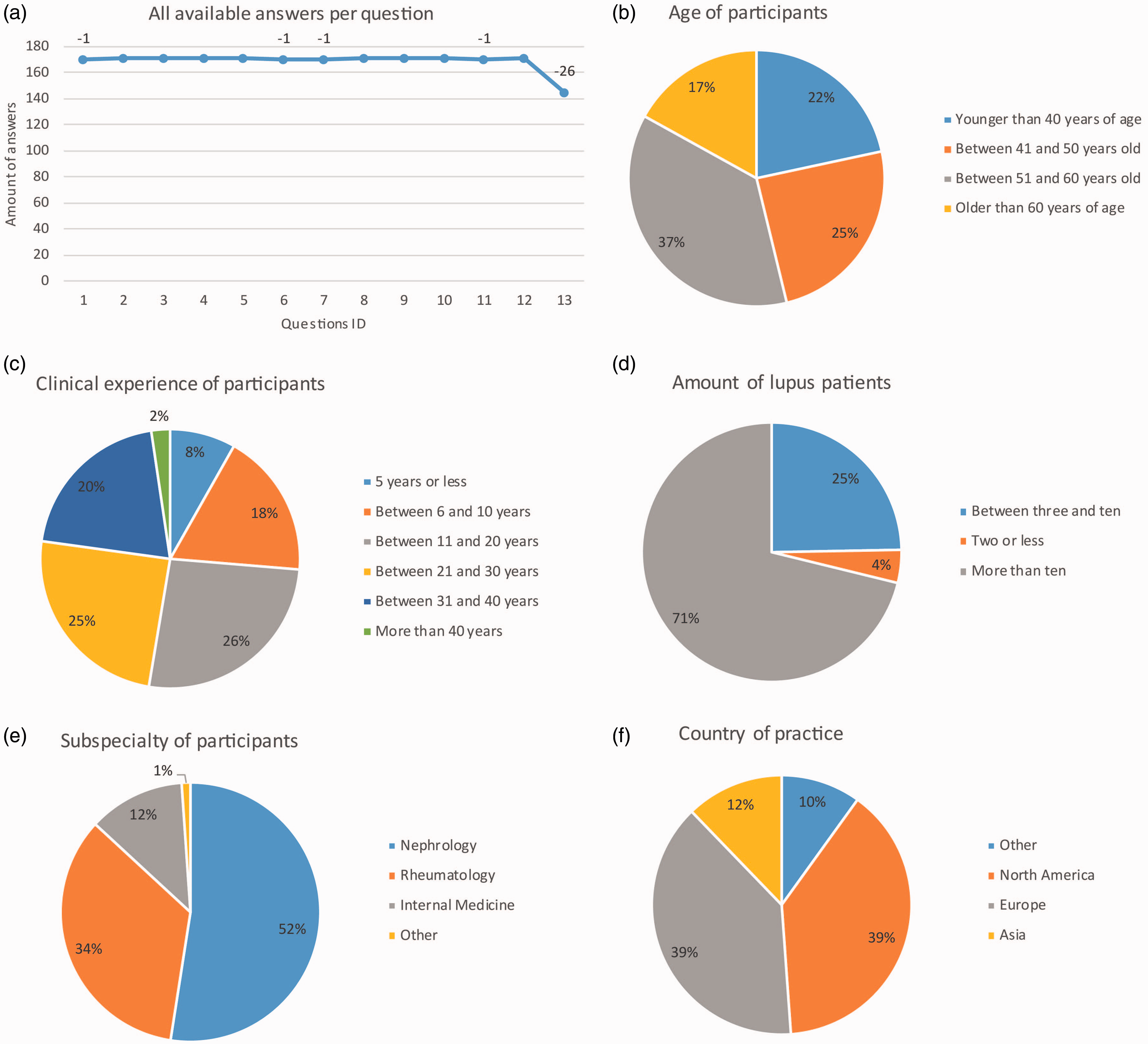
Demographic data on survey participants
Age distribution and years of clinical experience of participants are shown in Figure 1(b) and (c), respectively. A total of 74% of participants reported more than 10 years of clinical experience (Figure 1(c)) and most participants (71%) reported treating more than 10 patients with lupus nephritis (‘LN specialists’) (Figure 1(d)). A total of 52% of participants were nephrologists, 34% were rheumatologists, and the remainder (13%) mostly reported general internal medicine as their specialization (Figure 1(e)). A total of 39, 39, and 12% of participants reported Europe, North America, and Asia as their country of clinical practice, respectively (Figure 1(f)). When participants who only completed questions on clinical practice (n = 171) were compared with participants who completed the full questionnaire (including questions on sequential LN treatment) (n = 145), these distributions showed no significant differences (see Supplemental Figure 1).
Clinical practice in lupus nephritis
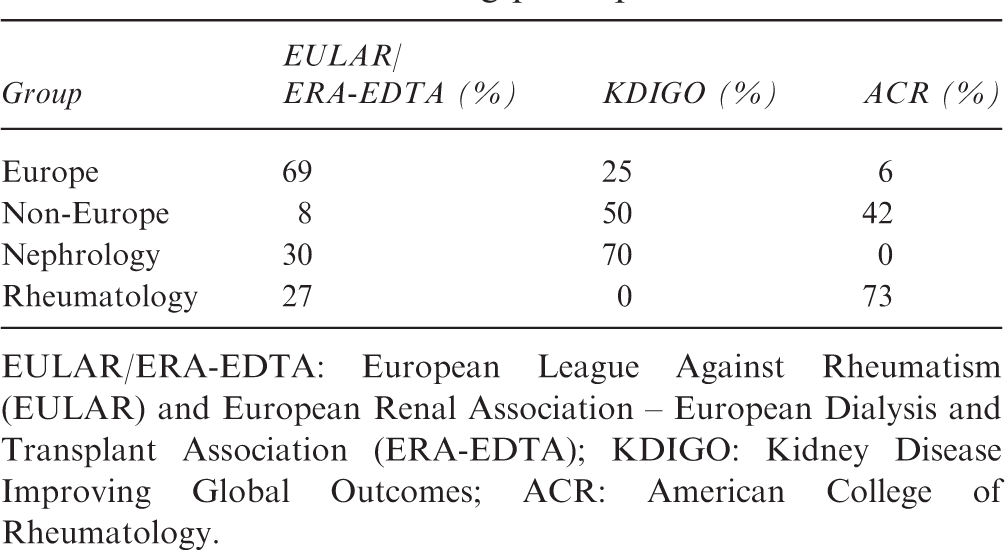
Use of guidelines. The main part of the questionnaire focused on patterns of clinical practice in LN. To this end, first awareness and usage of published guidelines were asked (Table 1). Nearly half of all participants (48%) reported adherence to recommendations from all three guidelines in their clinical practice (Figure 2). One quarter of participants reported single guideline use, which was somewhat balanced between KDIGO (Kidney Disease Improving Global Outcomes) (37% of single guideline users) and EULAR/ERA-EDTA (European League Against Rheumatism (EULAR) and European Renal Association – European Dialysis and Transplant Association (ERA-EDTA)) (30% of single guideline user) and, a little less frequently, ACR (American College of Rheumatology) (26% of single guideline users). As the respective guideline usage might be specifically affected by the country of clinical practice, we compared the prevalence of single guideline use between participants in Europe and North America (Table 1). Indeed, while single-guideline users from North America preferred ACR guidelines (60%), single guideline users from Europe preferred ERA-EDTA (73%) and KDIGO (20%) (p < 0.001, Chi2 test for ACR vs. non-ACR guideline use in participants from North America and Europe). Interestingly, in addition to differences in local prevalence of guideline use, specialty-dependent differences also exist, as all KDIGO single guideline users (n = 16) were nephrologists.
Guideline use among participants. (a) Pie chart depicting distributions of guideline use of overall participants. (b) Bar graphs showing proportions of individual guidelines used by participants who reported single guideline use. Guideline use among participants EULAR/ERA-EDTA: European League Against Rheumatism (EULAR) and European Renal Association – European Dialysis and Transplant Association (ERA-EDTA); KDIGO: Kidney Disease Improving Global Outcomes; ACR: American College of Rheumatology.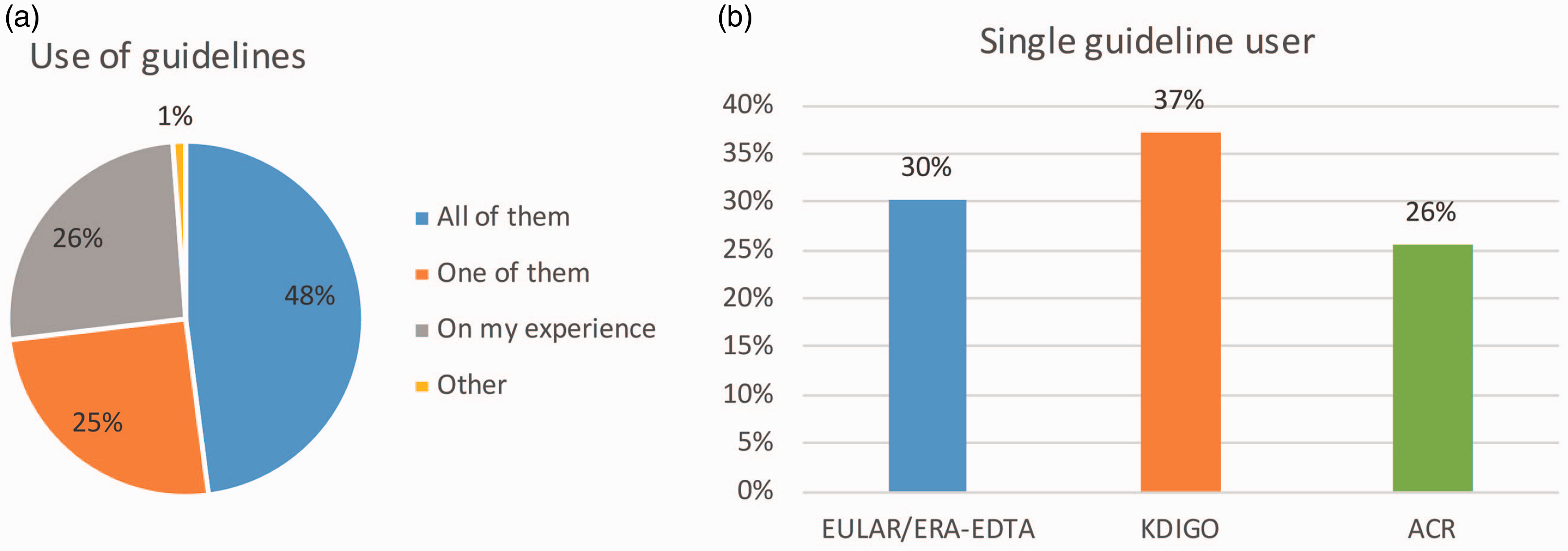
Time point of reassessment. Next, we were interested in the time point and way of reassessment of LN activity to identify refractory cases. Specific time points of reassessment, stratified for different agents are shown in Figure 3. Most participants (58%) reassess LN activity after six months, irrespective of treatment, albeit with statistically earlier assessment after cyclophosphamide (CYC) induction (EURO lupus protocol) and later reassessment with the use of rituximab (RTX) (p < 0.00001, Chi2 test, respectively). While no differences in the timing of reassessment were found between different specialties or according to years of clinical experience, participants that treated less than 10 patients reassessed patients significantly more often after three months compared to LN specialists, who reassessed later (p < 0.05, Chi2 test).
Time point of treatment response. Bar graphs showing time points of re-evaluation of disease activity after induction therapy, stratified for individual drugs as well as country of practice of participants.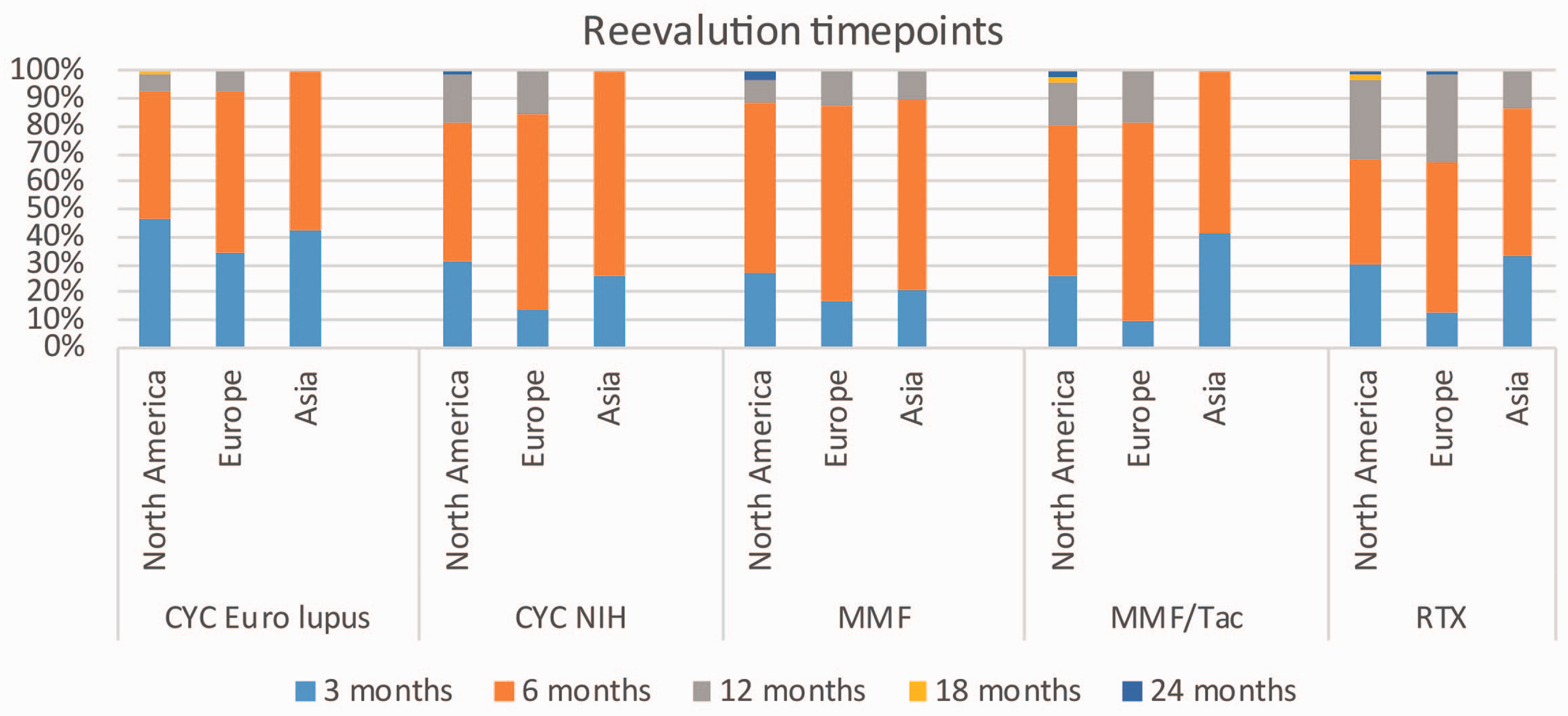
With respect to the markers used for reassessment, the majority of participants reported on standard evaluation of proteinuria (92%), serum creatinine (67%) or the eGFR (54%) and the urinary sediment (58%) (see Figure 4(a)). Interestingly, 58% of clinicians also reported to base their reassessments on the results of a re-biopsy, while less than 37% of participants reported the use of an autoantibody titer such as ds-DNA antibodies. When respective marker usage was compared between subgroups, LN specialists relied less on clinical symptoms, but more on findings in the urinary sediment and on performing a re-biopsy when compared to participants treating less than 10 patients (p < 0.05 in Chi2 tests, respectively). Also, when we compared testing regimens between nephrologists and rheumatologists, we found rheumatologists statistically more likely to perform urinary sediment analysis (66 vs. 48%, p < 0.05, Chi2), while nephrologists conversely relied significantly more on clinical symptoms (61 vs. 31%, p < 0.0001, Chi2) but this term was not further specified. One quarter of participants reported to guide their practice mostly on personal experience despite being aware of guidelines. Therefore, we compared patterns of clinical practice of these participants (non-guideline users) with those of participants reported to use one or all guidelines for their practice (guideline users). The non-guideline users, who were more frequently practicing in North America (Chi2 p < 0.05), overall reported the same patterns of clinical practice regarding both time point and markers of reassessment as guideline users, using serum autoantibodies more frequently, but this trend did not reach statistical significance. Also, when participants who did not complete the optional parts on sequential LN treatment (see below) were compared with all participants, no significant differences were found.
Parameters used for re-evaluation of LN activity. (a) Bar graphs indicating parameters used by nephrologists (blue) and rheumatologists (orange). (b) Pie chart depicting the distribution of participant's definitions of proteinuria cut-offs for diagnosing refractory lupus nephritis.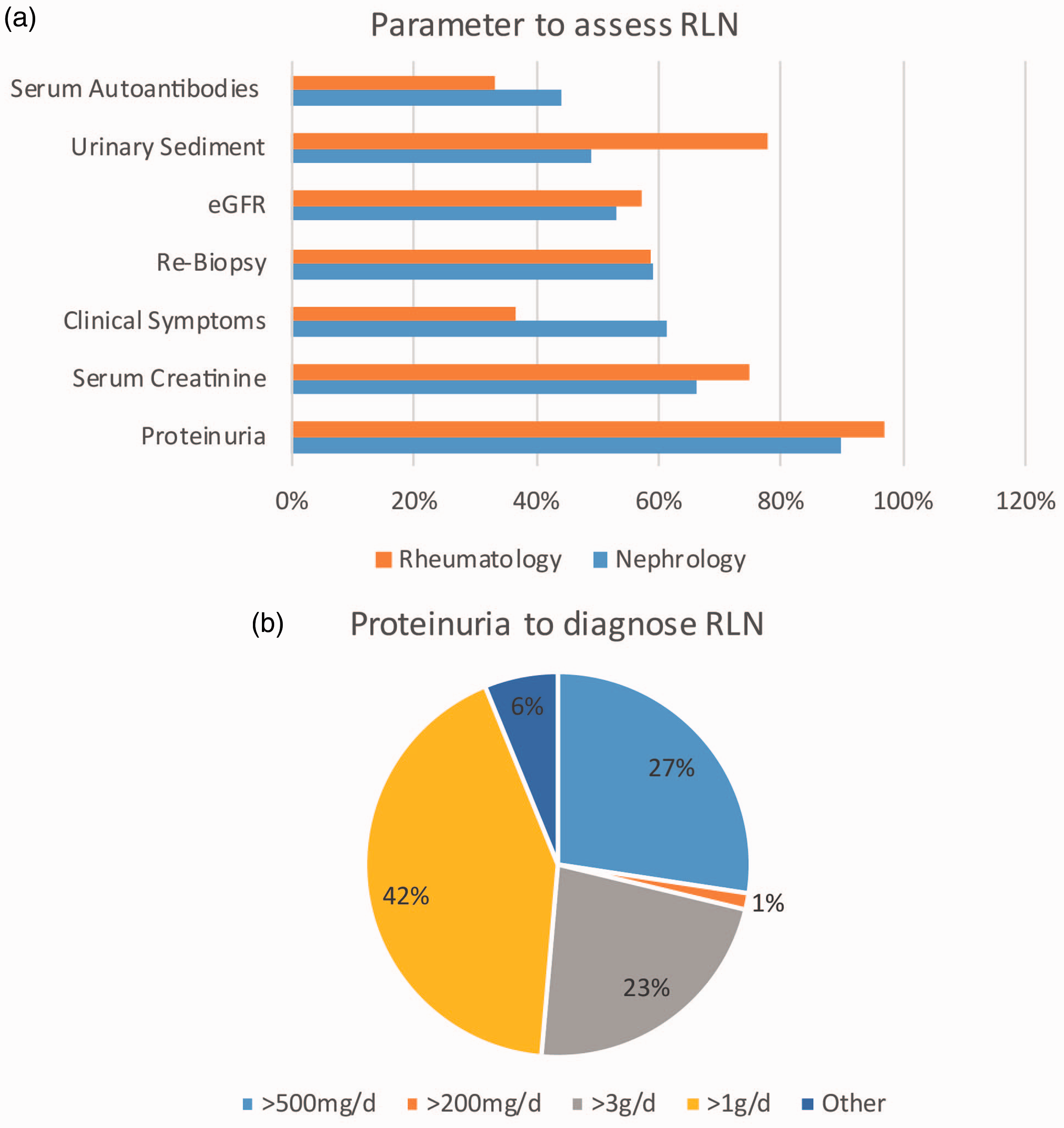
Taken together, these results indicate that, in a representative cohort of LN specialists from Europe, the United States, as well as Asia, (i) most clinicians adhere to one or more LN guidelines, (ii) reassessment of LN activity after induction therapy is typically performed after six months of therapy, and (iii) reassessment tests show considerable variation among participants.
Definition of refractory lupus nephritis
Marker dynamics. While reassessment of disease activity and respective parameters used for assessment varied, we next asked participants for criteria they apply in order to classify lupus nephritis as ‘refractory’. To this end, participants were asked to specify relative changes of the markers they use for LN reassessment (‘increasingly abnormal’, ‘unchanged’, ‘improved, but not normal’). In general, the majority of participants considered clinical symptoms (85%), serum creatinine/eGFR (90/92%), autoantibodies (73%), urinary sediment (76%), and lesions on renal re-biopsies (88% for light microscopy, 83% for IHC/EM) as markers of refractory disease only when unchanged or increasingly abnormal, while an improved, but less than halved, proteinuria was already considered indicative of RLN for most participants (80%). Interestingly, non-nephrologists mostly assessed proteinuria by means of 24 h urine sampling, while the majority of nephrologists relied on the urinary protein/creatinine ratio (UPCR) or the albumin/creatinine ratio of a spot urine sample (59 vs. 38%, p < 0.05 Chi2). Absolute levels of proteinuria to trigger diagnosis for RLN are shown in Figure 4(b). Apart from proteinuria assessment, the patterns of response criteria were generally consistent between nephrologists and non-nephrologists, as well as between LN specialists and non-LN specialists.
Concerns in RLN. We then asked participants to specify their concerns in patients with RLN. The majority of participants listed CKD (69%) and even ESRD (67%) as a concern in patients with RLN. While 56% of participants were also concerned about excess mortality and 50% about cumulative drug toxicity, only 44% of participants listed impaired patient's quality of life as a concern. While Europeans were less concerned about mortality compared to non-Europeans (35 vs. 61%, Chi2, p < 0.05), Asians were especially concerned about cumulative drug toxicities (80 vs. 51%, p < 0.05, Chi2). Interestingly, rheumatologists were significantly more concerned than nephrologists about mortality (80 vs. 57%, p < 0.01, Chi2) and ESRD (92 vs. 65%, p < 0.01, Chi2), while additionally there was an obvious trend for more concerns overall (on average + 15%) in non-LN specialists compared to LN specialists, regardless of the specialty (p < 0.0001, Cochran–Armitage test).
Potential causes of RLN. When asked for potential causes of RLN, more than 91% of participants listed the persistent immunological SLE activity as a priority differential diagnosis (Figure 5). Interestingly, the second most frequent differential diagnosis of RLN, listed by 71% of participants was insufficient drug adherence, followed by renal scarring/Class VI LN (56%), and genetic factors in both pharmacogenetics (45%) and LN pathogenesis (43%). Of note, less than 32% of all participants considered an underlying kidney disease other than LN a reason for RLN in SLE patients, with nephrologists considering a coexisting second renal pathology significantly more often than rheumatologists (58 vs. 38%, p < 0.05, Chi2). When those participants who reported considering other renal diseases than LN as a RLN cause were asked for specific concurrent pathologies, TMA/APS was by far the most prevalent answer, while conversely participants who listed genetic factors for a refractory course of LN mostly listed podocyte genes and APOL1. Taken together, there was consensus among a majority of participants on markers for RLN (symptoms, serum creatinine/eGFR, and proteinuria) as well as on concerns in RLN patients (mainly excess mortality), while there was neither consensus on a proteinuria cut-off for RLN nor on causes of RLN other than persisting SLE activity (e.g. other kidney diseases or non-adherence to therapy).
Underlying causes of refractory lupus nephritis. Bar graphs indicating participants' agreement rates to different possible etiologies of refractory lupus nephritis, stratified for country of practice.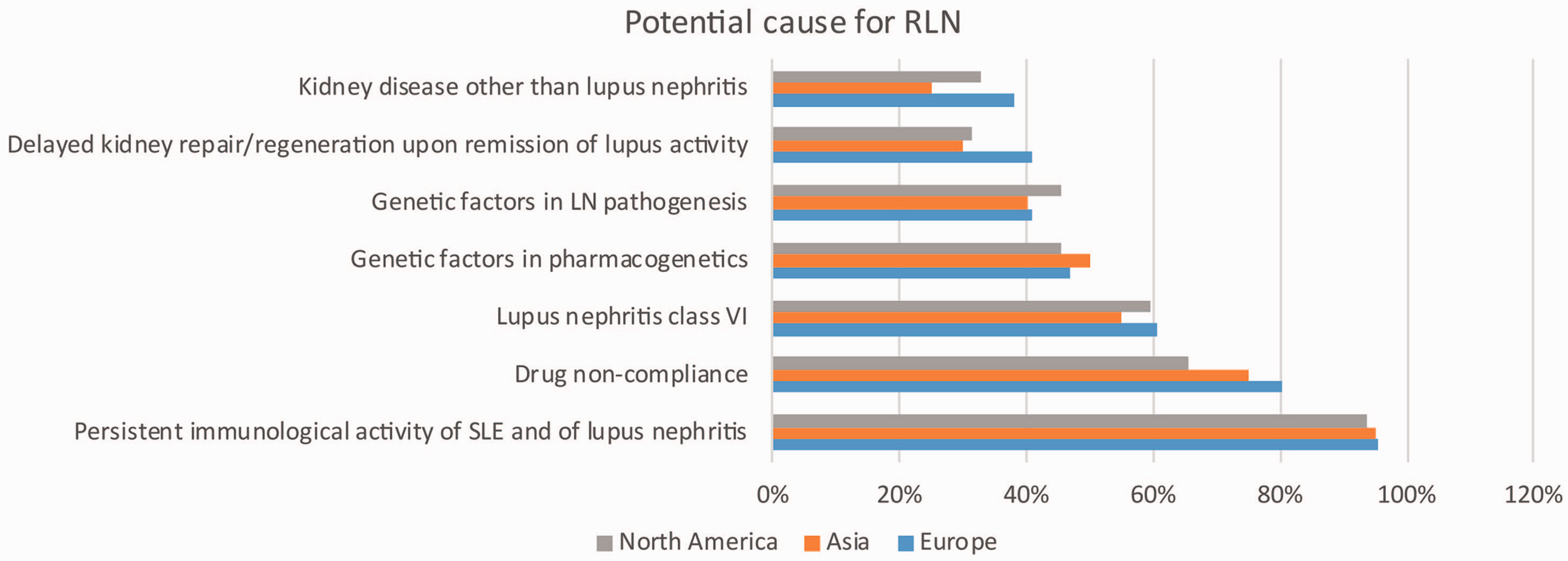
Clinical practice in the treatment of lupus nephritis
Targeting insufficient drug adherence. With regard to drug adherence, more than 69% of participants from Europe and North America reported the preferential use of IV drugs, while participants from Asia reported such practice only in 38% of cases (p < 0.01, Chi2) (Figure 6). Conversely, pill counting was reported by 29% of participants from Asia, but less than 13% of participants from Europe and North America reported this strategy to ensure adherence (non-significant at p = 0.05, Chi2). Interestingly, regular drug plasma level monitoring was reported by less than 20% of participants irrespective of country of practice. We did not observe significant specialty-dependent differences regarding drug adherence control, albeit a numerically bigger fraction of nephrologists report use of regular drug plasma monitoring compared to non-nephrologists (15 vs. 8%, n.s., Chi2). No significant differences were found though between LN specialists and non-LN specialists.
Measures to secure treatment adherence. Bar graphs depicting several strategies used by participants in clinical practice to ensure sufficient drug adherence by patients. Responses are stratified for country of practice.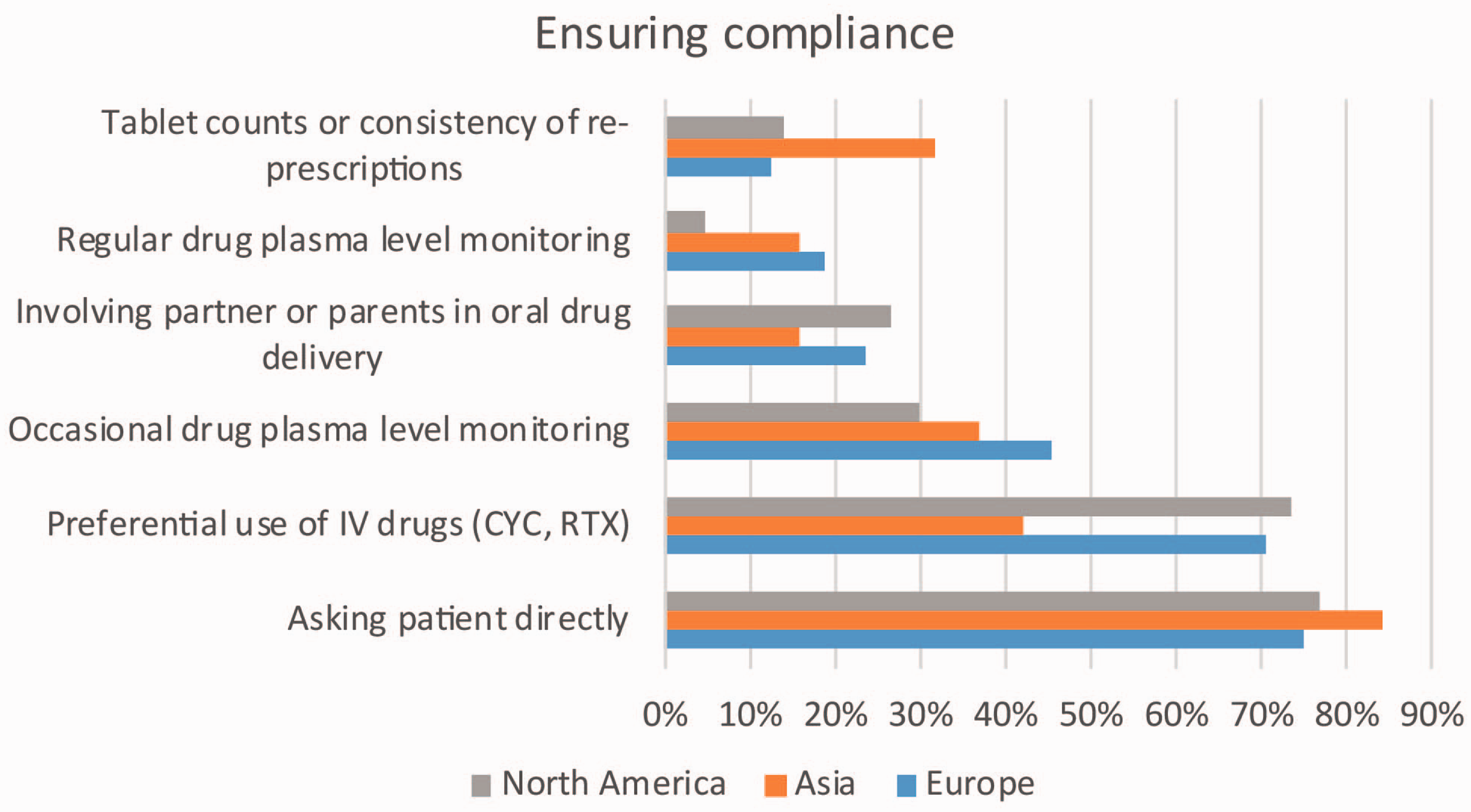
Lupus nephritis therapy according to treatment line
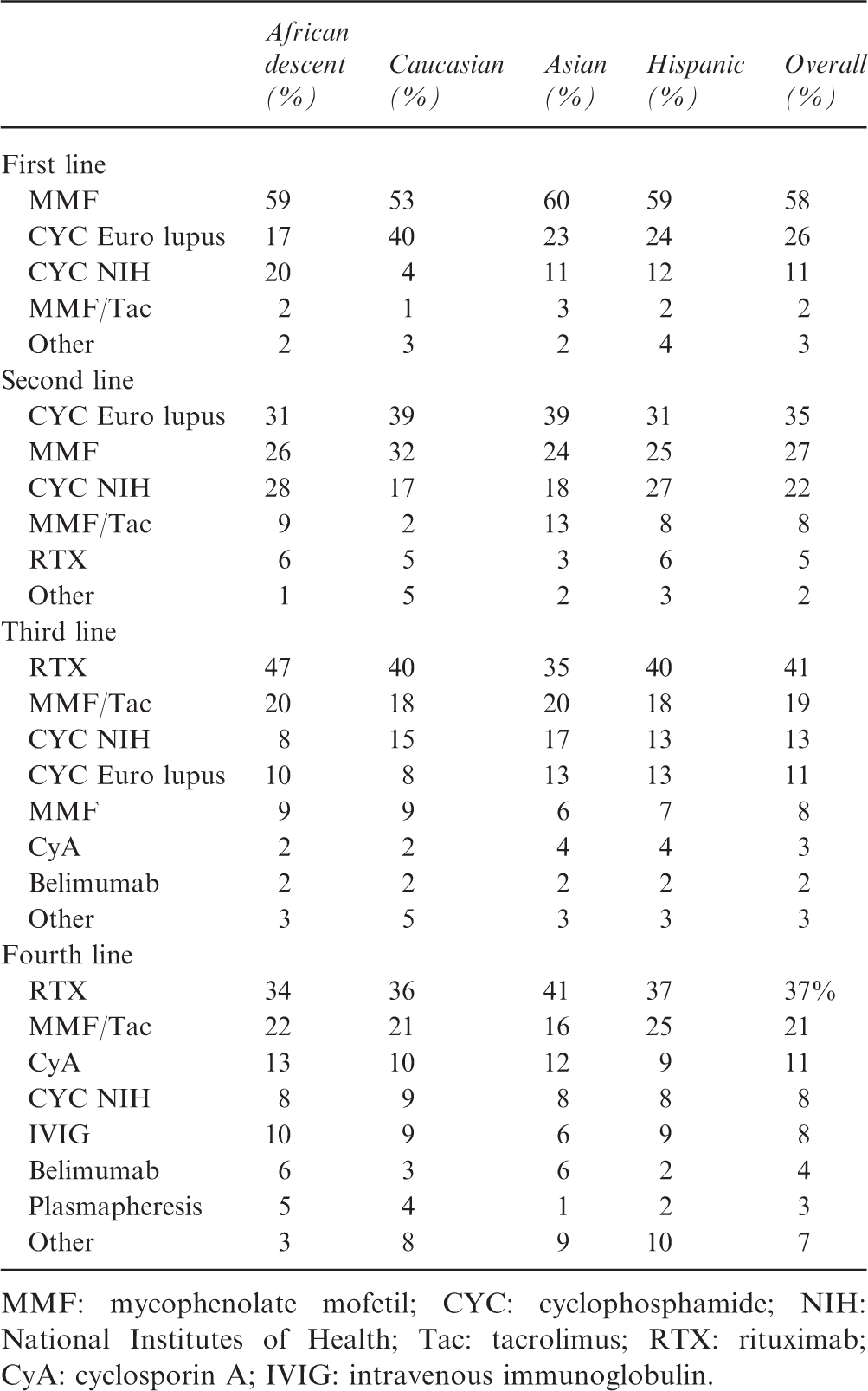
MMF: mycophenolate mofetil; CYC: cyclophosphamide; NIH: National Institutes of Health; Tac: tacrolimus; RTX: rituximab; CyA: cyclosporin A; IVIG: intravenous immunoglobulin.
Discussion
Given the lack of a consensus on definition and management of RLN, we had speculated on a considerable variability of views on this topic and differences related to world region or type of clinical specialization. With approximately 75% of participating physicians caring for more than 10 LN patients, our cohort represents nephrologists and rheumatologists familiar with the topic ‘lupus nephritis’. Of note, most participants of the survey had considerable clinical experience. Interestingly, we did not observe any differences in management of RLN between more and less seasoned clinicians, while such differences were present between participants who manage more and less than 10 RLN patients, respectively (e.g. timing of reassessment). This is in line with the common finding in medicine that patient volume, rather than mere clinical experience independent of the topic, determines quality of care.7–9
As expected, we identified significant differences regarding both the definition as well as the management of RLN, e.g. between Europe and Northern America. This can be only partially explained by divergent guidelines,2–4 as the differences remained significant also when only answers were compared that came from participants who stated they would treat patients according to all guidelines. Three major differences deserve particular discussion:
Time point of evaluation of response to induction therapy: According to a recent analysis of several major cohorts with long term outcome data, the best predictor of long term renal outcome is proteinuria of less than 0.8 g/d after 12 months. 10 This study further showed that the assessment of microscopic hematuria is actually not helpful in outcome prediction. Of note, in accordance with ACR guidelines, 60% of survey participants still base their clinical adjudication on the presence of RLN on this finding. In fact, even early histological findings might not be representative, questioning an all too permissive practice of early re-biopsy (60% of participants). Delayed healing of the glomerular filtration barrier is a frequent cause of persistent proteinuria at six or 12 months and cannot be considered as persistent autoimmune disease activity RLN without further proof, i.e. repeated kidney biopsy.11,12 Numerous urinary and serum biomarkers have been proposed as potential substitutes for repeated kidney biopsy in this context but validation using the gold standard repeated kidney biopsy is usually not performed. 13
Concerns on cumulative drug toxicity: Participants from Asia are significantly more concerned with cumulative drug toxicity and mortality, probably because of the excess rate of severe adverse events observed in MMF trials between Asian and non-Asian patients.14,15
Differences between nephrologists and rheumatologists: We observed a highly significant difference in the rate of RTX prescription between rheumatologists and nephrologists, independent of RLN treatment line (i.e. first, second, or third line). Although case series suggest that RTX may be effective in RLN, randomized trials failed to meet their primary endpoints.16–18 While doubtlessly rheumatologists have more experience with the use of RTX given its value in rheumatoid arthritis therapy, 19 the reason for our finding remains unclear. Nephrologists relied more on clinical symptoms to define RLN but we failed to specify ‘clinical symptoms’ any further, which remains a limitation of this study.
Despite this apparent discrepancy in patient care on different sides of the Atlantic, there are also features where large consensus was present. Namely, guideline use/adherence in general was reported by 99% of participants, with almost 50% reporting adherence to all major guidelines. This underlines the value of guidelines in LN patient care, yet it underlines the necessity for adequate representation of RLN in these guidelines. Given the lack of specific recommendations for RLN treatment in the current guidelines and the subsequent variability in de facto medical care for RLN patients as evidenced by our survey, we advocate to include a consensus definition of RLN into such recommendations.
Another common finding of this survey was that, despite the common notion of drug non-adherence as a cause of RLN by 80% of participants, objective testing for drug adherence such as drug plasma level monitoring and tablet counting were performed by less than 20% of participants. This practice needs to be critically evaluated given the non-adherence to lupus medication is substantial (43 to 75%). 20 Lastly, around 50% of participants recognize the importance of genetic factors for RLN, both pertaining to the presence of non-lupus kidney disease (e.g. podocytopathies or APOL1 genotype) as well as pharmacogenetic reasons for therapy failure.
Obviously, this survey is not representative of all physicians that are involved in the treatment of LN, whether refractory or not. In fact, it has been shown that mortality for LN patients is lower in a hospital treating more than 50 patients per year compared to hospitals admitting fewer patients. 21 It is currently unknown how this translates into quality of care in the outpatient setting. The significant difference in clinical practice even among experienced specialists, however, argues for referral of RLN patients to large-volume centers, the continued development of guidelines as well as more clinical trials to replace uncertainty with evidence. In this regard, it should not be omitted that guidelines and evidence-based medicine can never substitute individualized therapy by an experienced specialist. While there are already recommendations for initial LN drug choice based on ethnicity, 22 personalization of therapy will continue to change the traditional style of guidelines (‘one drug fits all’) towards an informed and individual therapy for each patient, based on validated clinical, pathological as well as pharmacogenomic patient characteristics.5,21
Supplemental Material
Supplemental material for Refractory lupus nephritis: a survey
Supplemental Material for Refractory lupus nephritis: a survey by M Weidenbusch, Y Bai, J Eder and H-J Anders; for the Lupus Nephritis Trials Network in Lupus
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HJA was supported by European Union’s Horizon 2020 research and innovation program under grant agreement No. 668036 (project RELENT) and by the Deutsche Forschungsgemeinschaft (AN372/24-1). MW was supported by the BMBF (grant No. FKZ 01PL12016); the Lehre@LMU (grant No. FöFoLe 51/2015 and 932); and the Friedrich-Baur-Stiftung (grant No. 33/16). YB was supported by a scholarship from the China Scholarship Council Program (CSC).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.