
Abstract
Lupus erythematosus (LE) represents a spectrum of inflammatory autoimmune disease comprising varying clinical entities ranging from primary cutaneous to systemic disease. There is a clear relationship between ultraviolet irradiation (UVR) and the clinical manifestations of LE in both adult and pediatric populations. Although it has been established that UVR exacerbates pre-existing LE, it remains unclear whether UVR induces the development of the disease. This review serves to discuss effective photoprotective measures in LE and describe the pathogenic relationship of UVR and LE.
Introduction
Lupus erythematosus (LE) represents a spectrum of inflammatory autoimmune disease comprising varying clinical entities, ranging from primary cutaneous disease (cutaneous LE, CLE) to a severe systemic disease (systemic LE, SLE). Clinical features, histological changes, laboratory abnormalities, and duration of skin lesions further categorize CLE into the following: acute CLE, subacute CLE (SCLE), and chronic CLE. 1 Another subtype with characteristic clinical, histological, and laboratory features has been classified as LE tumidus. 1 Also noteworthy, neonatal LE is a rare, autoimmune disease caused by transplacental transfer of maternal IgG antibodies, in which 50% of patients initially present with a transient rash that resembles SCLE. 1
There is an evident relationship between ultraviolet (UV) irradiation (UVR) and the clinical manifestations of LE in both adult and pediatric populations.2,3 Even though it is well known that UVR exacerbates pre-existing LE, it remains unclear whether UVR induces the development of the disease. 4 An essential element in the management of LE, then, is the discussion of clinical importance and therapeutic goals of photoprotection. This review serves to describe the pathogenic relationship of UVR and LE and to discuss effective photoprotective measures in LE.
Mechanisms of photosensitivity in lupus
Factors that influence the intensity of UVR include the atmosphere, latitude, altitude, season, time of day, and presence of clouding, reflection, and water depth.5,6 Among UVR, only visible light, UVA (320–400 nm), and UVB (290–320 nm) penetrate the earth's stratospheric ozone layer, while UVC (200–290 nm) is completely blocked. 7 Depending on the glass coating, window glass is UVA permeable. 8 If the rays reach the skin, both UVA and UVB penetrate the epidermis. Approximately 10% of UVB reach the upper dermis and 30–50% of visible light and UVA reach the deeper dermis. The effects of solar irradiation causing tissue damage are a result of energy transfer from UVR to biopolymeric molecules, such as DNA, RNA, and peptides, with subsequent free radical formation. 7 Solar irradiation also transiently disables Langerhans cells' function as antigen-presenting cells. 7
Mechanisms of photosensitivity in lupus erythematosus
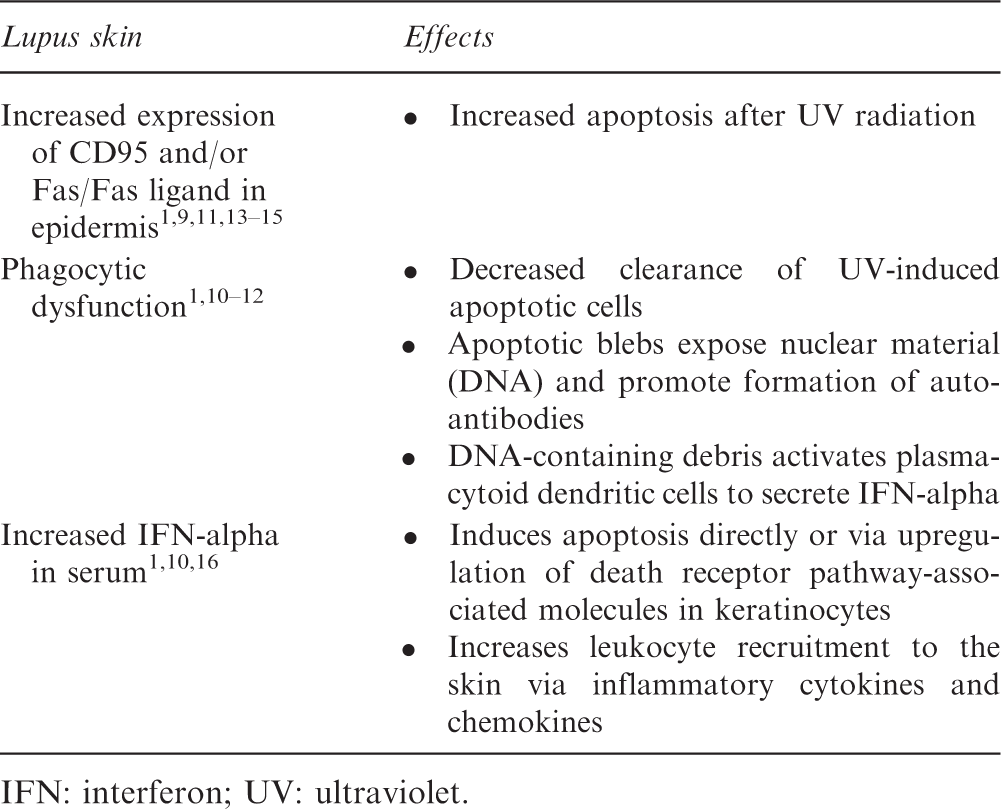
IFN: interferon; UV: ultraviolet.
Another result of DNA-containing leftover nuclear debris from apoptosis is the activation of plasmacytoid dendritic cells which secrete interferon (IFN)-alpha. Some authors hypothesize that the increased serum IFN-alpha levels observed in lupus patients may be a direct result of this process. 1 Certain patients with CLE have mutations in IFN regulatory factor 5 (IRF5), tyrosine kinase 2 (TKY2) or three prime repair exonuclease 1 (TREX1), genes that increase IFN-alpha production. 16 IFN-alpha increases leukocyte recruitment to the skin by way of inflammatory cytokines and chemokines, which promote cutaneous inflammation. 16 In addition, increased serum IFN-alpha induces apoptosis directly or through upregulation of death receptor pathway-associated molecules in keratinocytes. 10 Additionally, UV light directly upregulates TNF-alpha and other pro-inflammatory cytokines, which are important in the pathogenesis of lupus. 16 In summary, an imbalance between the production and clearance of apoptotic cells and cellular debris may facilitate the development of skin lesions of LE. This complex pathogenic multi-step process may reflect the latency period observed between UV exposure and development of LE skin lesions, which can range from several days to three weeks and can last up to two months.1,17
The threshold UV dose to trigger LE flares is lower than that of sunburn. 7 The degree of photosensitivity varies with type of LE. A large European multicenter study revealed that patients with SCLE and LE tumidus had the highest percentage of UV-inducible lesions.8,18 Additionally, ethnicity impacts the level of photosensitivity as most patients (86%) in the aforementioned study who developed UV-induced skin eruptions were light-skinned (Fitzpatrick phototypes I or II).7,8 Moreover, it has been postulated that subsequent exposures to UVR after an initial UV-induced flare result in a significantly higher frequency of UV-induced eruptions as supported by a photoprovocation study.1,19
Photosensitivity in LE
Photosensitivity is one of the diagnostic criteria established by the American College of Rheumatology (ACR) for SLE. Abnormal photosensitivity is present in 40–90% of the adult population with LE; this variation is likely a result of the variability in patient populations, protocols, and definition of photosensitivity used in studies.17,18,20–26 Photosensitivity can not only manifest as skin symptoms, such as rash or tingling, but also as fatigue and arthralgia, which are especially important to elicit when evaluating patients with lupus. 2 While the ACR has defined photosensitivity as a “skin rash as a result of unusual reaction to sunlight,” this definition is not exclusive to lupus patients, and can include patients with other skin diseases, such as dermatomyositis. 2 This description can also include inflammatory lesions, other than CLE, such as polymorphous light eruption in lupus patients. 2 Thus, there is a lack of a standardized definition of photosensitivity and the description is open to varying interpretations. 2
The most photosensitive subtype of LE is LE tumidus, followed by SCLE. 18 The photoprovocation protocol is a standardized in vivo assay to test the capacity of a sunscreen to photoprotect LE patients under controlled conditions. 27 Utilizing this protocol, studies that evaluate the efficacy of sunscreen as a preventative measure for the development of UV-induced skin lesions in LE are primarily composed of the adult population.
A representative study of adults with LE suggested that sunscreens protect against UV-induced LE lesions to varying degrees as a result of different capacities of protection from UVA. 27 Another larger, retrospective analysis showed that 96% of patients with LE were entirely protected by sunscreen, some of whom previously developed UVR-induced skin lesions. 28 Furthermore, the authors concluded that the efficacy of a sunscreen to shield UV-induced skin eruptions in LE could not be deduced from its ability to prevent sunburn. 28 Several years later, a prospective study demonstrated that the use of a broad-spectrum sunscreen with a high UV protection factor can prevent skin lesions in patients with CLE. 8 Two histological studies demonstrated that prior to standardized photoexposure, the application of a broad-spectrum sunscreen on patients with CLE prevents the prototypic inflammatory response.29–31 In a study, laboratory testing for specific antibodies, such as antinuclear antibodies, anti-dsDNA, SSA/Ro, SSB/La, RNP, Sm, has not shown to correlate with photosensitivity, though this study may not have been powered to detect a difference. 18 In addition, better systemic outcomes have been noted in SLE patients using consistent sunscreen. 8 Thus, substantial clinical and experimental evidence exists that support the use of broad-spectrum sunscreen as an effective photoprotection measure to prevent UVR-induced damage in photosensitive adults with LE.
Although studies on photoprotection in the pediatric population have not been performed, photoprotection for children is especially important, as estimates indicate that at least 50% of lifetime exposure to UVR occurs by 18 years of age. 32 Very early onset photosensitivity can occur in patients with neonatal LE, which is why avoidance of sunlight is especially recommended. 20 Pediatric photosensitivity is suspected to be more common than adult photosensitivity in cases of LE. A recent study indicated a higher statistical prevalence of photosensitivity in pediatric-onset SLE (20%) than the adult-onset disease (9%). 33 Supporting this observation, in a single study, it has been shown that photosensitivity appeared more frequently in patients younger than 40 years of age with CLE, although a pediatric population was not studied; however, another study showed no correlation.18,24 Further studies evaluating the efficacy of sunscreens in pediatric-onset LE is warranted.
The shielding benefits of sunscreen usage towards undesired effects of UVR, other than sunburn, have been controversial.28,34,35 Sunscreens protect by reflecting and absorbing UVR and come in two forms: physical and chemical sunscreens. Physical sunscreens are made of zinc and titanium oxides, which reflect, scatter, and absorb light. Special formularies and micronization or the creation of ultrafine particles can improve the cosmetic appearance of these sunscreens. In contrast, chemical sunscreens are composed of aromatic compounds, which absorb UVR by transiently exciting electrons to higher energy levels. 7 When these electrons return to the ground state, the energy released comes in the form of light in the visible and infrared spectrum. 7 The quantifiable measure of protection from UVB is the sun protection factor (SPF), which is the dose of UVB required to develop minimal erythema following an even application of 2 mg/cm2 of sunscreen when compared to the UVB dose inducing minimal erythema on unprotected skin. 7
Sunscreens and other photoprotective measures
Labeling provisions for sunscreens by the FDA. 36
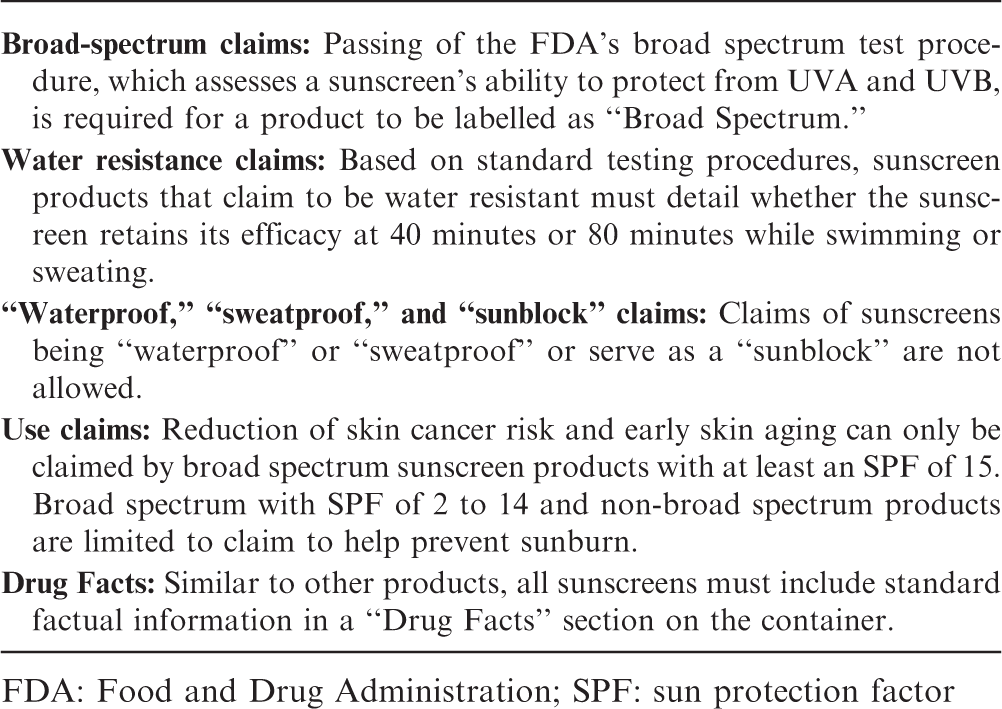
FDA: Food and Drug Administration; SPF: sun protection factor
Studies have raised concerns about the environmental effects of some of the commonly used organic UV filters including oxybenzone (benzophenone-3), 4-methylbenzylidene camphor, octocrylene, and octinoxate (ethylhexyl methoxycinnamate).37,38 Oxybenzone, octocrylene, octinoxate and ethylhexyl salicylate have been identified in nearly all water sources worldwide and standard waste water treatment plant techniques are not sufficient for their removal. Some of these UV filters have also been identified in various fish species worldwide. Even more concerning are the implications of oxybenzone on coral reef bleaching, which has been shown to be a contributor in the laboratory setting. With sunscreens representing a front-and-center issue at the FDA, it will be noteworthy to follow further changes and new regulations to sunscreen products.
The frequency of sunscreen utilization, the SPF, and the amount applied have increased from the 1990s to 2016. 39 Sunscreens have been shown to be beneficial only when used properly, including repeat applications every two hours when outdoors, application approximately 20 minutes before sun exposure, and an appropriate amount of sunscreen. The American Academy of Dermatology recommends at least 30 mL of sunscreen to cover the skin's surface to achieve the goal concentration of 2 mg/cm2. 40 In actuality, approximately 25–50% of the desired amount is commonly applied. 41 A recent study aimed to assess sunscreen application habits found that difficult to reach areas, such as the back, hands, and feet, and areas surrounding the swimming suit, were surfaces that were not covered by sunscreen. 42 Moreover, sunscreen usage has shown to decrease significantly on overcast days despite UV index being greater than 6 (dangerous levels). 43 Thus, there are opportunities for improvement in public education about the use of sunscreens.
Besides photoprotection with sunscreen, other photoprotective agents for lupus patients include systemic drugs, such as chloroquine or hydroxychloroquine.44–46 Antimalarials shield UV light from absorption, which inhibits the development of CLE lesions. 47 It may also be inferred that since antimalarials impair the processing of autoantigens, the defective immune response to UVR-induced apoptosis may be blocked with these agents. 8 Chloroquine hinders UVB-induced upregulation of cytokine and chemokine expression. 46 Interestingly, one study reported that concurrent use of hydroxychloroquine with sunscreen does not preclude the detection of photosensitivity in patients with LE; however, only a single patient was tested. 18
Currently, there are no studies in literature that evaluate the efficacy of protective clothing in the development of UVR-induced skin lesions in LE. However, wearing tightly woven clothing and a broad-brimmed hat have been widely encouraged. Cultural customs, including protective clothing wear, and general misconceptions have significant influence on photoprotective habits. 48 Males and dark-skinned and middle-aged patients were least likely to practice recommended photoprotection when compared with the remainder of the CLE adult population. 48 Additional studies in this area in the pediatric population would be useful to emphasize further education regarding the importance of photoprotection.
Conclusions
In summary, the general recommendation to prevent UVR-induced cutaneous lesions in LE requires guidance about avoidance of excessive sun exposure, proper sunscreen application with broad-spectrum coverage, photostability, and high substantivity, and protective clothing wear. Of careful consideration is the pediatric population, as studies demonstrate that photosensitivity is more prevalent in child-onset LE than the adult equivalent. The clinician must also recognize cultural customs and respond to common misconceptions when attempting to encourage optimal photoprotection.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.