
Abstract
Background
Non-pharmacologic therapies have been deemed as potentially beneficial for patients with systemic lupus erythematosus. We conducted an updated review to determine the effects of these therapies to inform practice.
Methods
A literature search was performed using PubMed (MEDLINE), EMBASE, Cochrane, PsychINFO, the Cumulative Index to Nursing and Allied Health Literature, Web of Science, and Google Scholar from inception until August 2018. We included randomized controlled trials of non-pharmacologic therapies in systemic lupus erythematosus patients with sample size ≥10. Systemic lupus erythematosus was defined by 1982 or 1997 American College of Rheumatology criteria. Studies were synthesized separately by patient-reported outcomes and disease activity. Due to the heterogeneity of interventions and comparisons, a meta-analysis was not performed.
Results
A total of 15 randomized controlled trials involving 846 participants met the inclusion criteria. Of the 15 trials, eight used exercise interventions, six used psychological interventions (one group psychotherapy, three cognitive behavioral therapies, one psychoeducation, one mindfulness-based cognitive therapy) and one used electro-acupuncture. Five of 15 studies utilized control groups consisting of usual medical care. Other studies included control interventions of relaxation, attention placebo, symptom monitoring support, education, minimal needling, isotonic and resistance exercise. Compared with the control conditions, non-pharmacological interventions were associated with a significant improvement in fatigue in three out of six studies. Three out of eight studies reported improved anxiety and depression, and one study reported improved pain after interventions. Seven out of 11 studies reported improvement in overall quality of life in at least one domain of the Short-Form Health Survey. Of note, no studies demonstrated an improvement in disease activity after 5–52 weeks of non-pharmacological therapies.
Conclusion
This review showed promising results for physical exercise and psychological interventions as adjuncts to traditional medical therapy for improvement in fatigue, depression, pain and quality of life for systemic lupus erythematosus. Further high-quality randomized controlled trials with longer follow-up periods are warranted.
Introduction
Patients with systemic lupus erythematosus (SLE) report high levels of cognitive difficulties, depression, pain, and fatigue.1–5 More than 80% of SLE patients experience fatigue and up to 90% experience pain at one point during the disease course.1–3 Psychological disorders are also common in SLE patients. Several studies have found that depression is highly prevalent in SLE ranging from 17–75%,4,5 which is higher than in the general population. A study by Bachen et al. found that up to 65% of Caucasian SLE patients had mood or anxiety disorders. 5 These factors play an important role in the psychological and physical wellbeing of SLE patients.
Although pharmacologic treatments have improved overall survival, SLE continues to have a profound impact on quality of life. 6 Despite several new therapies, there are significant unmet needs that need to be addressed such as fatigue, pain, and psychological symptom management.7,8 In addition, conventional pharmacological therapies can cause a wide range of side effects. Therefore, non-pharmacologic therapies may be important adjunctive options for SLE patients.
Over the last two decades, interest in non-pharmacologic therapies has increased in patients with SLE. A study of health resource utilization in a cohort of 707 SLE patients showed that 50% used alternative therapies and at similar rates across Canada, the United States, and the United Kingdom. 9 Despite a high rate of integrative medical therapies used by SLE patients, the scientific study of various types of non-pharmacologic therapies in SLE is very limited.
Several non-pharmacologic remedies have been studied as potentially beneficial for patients with SLE, including physical, psychological, complementary, and integrative interventions. A previous systematic review and meta-analysis by Zhang et al. compared the effects of psychological interventions among SLE patients. 10 The authors identified six randomized controlled trials (RCTs) and found that psychological interventions significantly reduced anxiety, depression, stress, and disease activity, compared with controls. No statistically significant differences were observed in mental health, fatigue, and physical function. In terms of exercise interventions, a systematic review with meta-analysis by O’Dwyer et al. showed that exercise intervention improved cardiorespiratory capacity, reduced fatigue, and improved psychological functions, compared with controls. Moreover, exercise interventions were safe, did not adversely affect disease activity, and were well tolerated by a majority of SLE patients. 11 Another systematic review by Pino-Sedeno et al. identified seven RCTs, one nonrandomized trial, and four prospective observational studies. This review specifically focused on fatigue as an outcome in SLE. They concluded that aerobic exercise was effective and suitable for reducing fatigue, but results were not always consistent across instruments used. It seems premature to confirm the efficacy of psychological interventions, acupuncture, diets, and ultraviolet A radiation in improving fatigue. 12 The current review differs from previous reviews of non-pharmacologic interventions for SLE in that it is limited to RCTs and is focused on five specific outcomes: fatigue, depression, pain, quality of life, and disease activity. In addition, our review also includes various types of non-pharmacologic interventions including exercise interventions, psychological interventions, and mind-body intervention.
Methods
We searched PubMed, EMBASE, Cochrane Library, PsychINFO, the Cumulative Index to Nursing and Allied Health Literature, Web of Science, and Google Scholar from their inception to August 2018. The search strategies used both controlled vocabulary terms and keywords for ‘systemic lupus erythematosus’ and ‘non-pharmacologic therapy’ and related methods. We did not restrict by date.
We included RCTs of non-pharmacologic interventions in SLE patients with sample size ≥10, measuring fatigue, depression, pain, quality of life, or disease activity. SLE was defined by 1982 or 1997 American College of Rheumatology (ACR) criteria. To narrow the focus of this review, we include interventions that utilized physical activity, psychological or mind-body approaches in conjunction with or as a part of the interventions. We delineate literature categories into exercise, psychological/educational, and mind-body interventions.
Data extraction and quality assessment were performed by one investigator and confirmed by at least one other investigator. Disagreements were resolved by consensus among team members. We extracted information on study characteristics, population characteristics, type, duration, frequency of interventions, and outcomes.
We qualitatively synthesized all included studies and grouped them into the following five categories of outcomes including fatigue, depression, pain, quality of life, and disease activity. Due to the heterogeneity of interventions and comparisons, a meta-analysis was not performed.
Results
Literature search
Figure 1 summarizes the flow of the literature search and publication selection process following PRISMA guidelines. A total of 2,466 references were identified by our search. After title and abstract screening, 49 articles remained for full-text screening. In total, 20 articles were excluded because they did not meet our inclusion criteria. We acquired 29 full text articles for further review. Of these 29 studies, 14 were excluded for the following reasons: non-RCTs (n = 8), the SLE diagnosis was not defined by ACR criteria (n = 3), the outcomes of interest were not assessed (n = 1), poor methodologic design (n = 1), and the sample size was less than the minimum of 10 (n = 1). Finally, 15 RCTs were included in our systematic review for data abstraction and critical appraisal.
The flow of the literature search and publication selection process following PRISMA guidelines.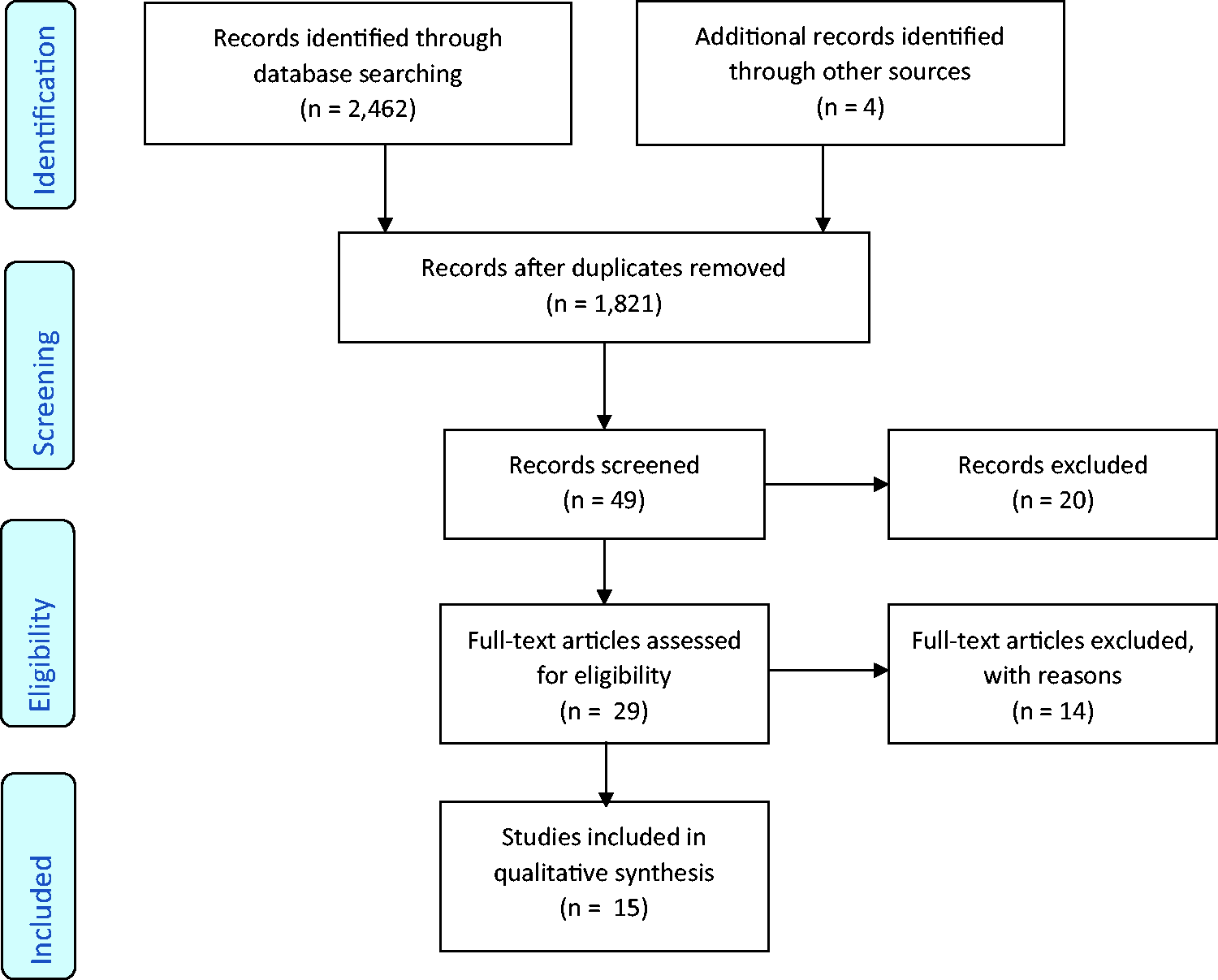
Participant characteristics and study setting
Overall, 15 RCTs involving 846 participants met the inclusion criteria and were included in this review.13–27 One study also included patients with chronic cutaneous lupus. 24 SLE was defined by 1982 or 1997 ACR criteria. SLE disease duration ranged between 2.5 to 21 years. SLE disease activity was low in all studies that were measured. Out of 15 studies, 13 were of adult subjects, two studies included only pediatric subjects.17,25 The mean age ranged from 13 to 53 years. In the 15 studies, 95.2% of subjects were female, with eight studies enrolling only females.
Intervention and control group characteristics
Non-pharmacologic interventions varied in their content, dosage, duration, and intensity. Of the 15 trials, eight used exercise interventions, six used psychological interventions (one group psychotherapy, three cognitive behavioral therapies (CBT), one psychoeducation, one mindfulness-based cognitive therapy (MBCT)), and one used electro-acupuncture. Individual sessions varied from 15 to 90 minutes, with session frequency ranging from one to three times per week. Lengths of the overall programs ranged from 5 to 52 weeks. Five of 15 studies utilized control groups consisting of usual medical care. Other studies included control interventions of relaxation, attention placebo, symptom monitoring support, education, minimal needling, and home, isotonic, and resistance exercise.
Outcome measures
Summary of evidence and effect of non-pharmacologic interventions for SLE
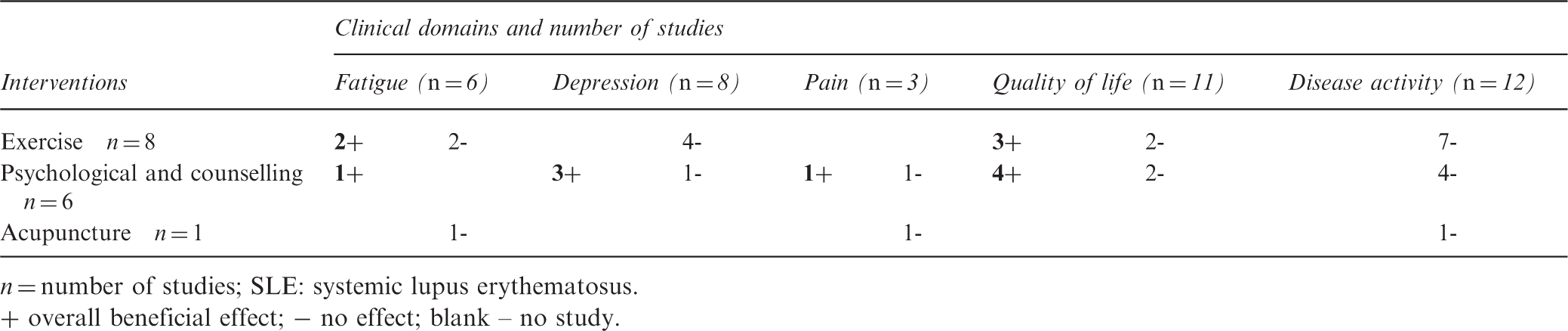
n = number of studies; SLE: systemic lupus erythematosus.
+ overall beneficial effect; − no effect; blank – no study.
Non-pharmacologic interventions in SLE
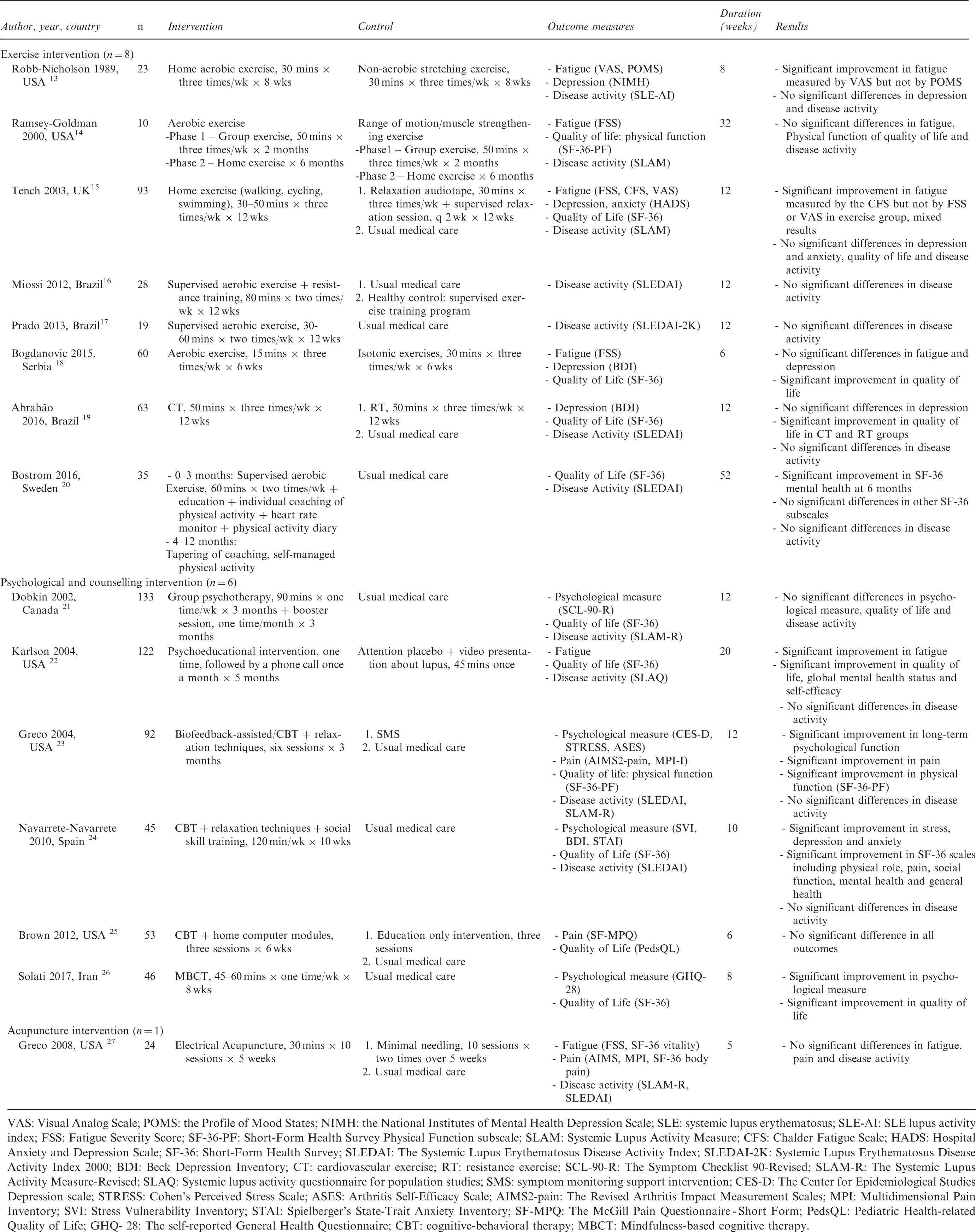
VAS: Visual Analog Scale; POMS: the Profile of Mood States; NIMH: the National Institutes of Mental Health Depression Scale; SLE: systemic lupus erythematosus; SLE-AI: SLE lupus activity index; FSS: Fatigue Severity Score; SF-36-PF: Short-Form Health Survey Physical Function subscale; SLAM: Systemic Lupus Activity Measure; CFS: Chalder Fatigue Scale; HADS: Hospital Anxiety and Depression Scale; SF-36: Short-Form Health Survey; SLEDAI: The Systemic Lupus Erythematosus Disease Activity Index; SLEDAI-2K: Systemic Lupus Erythematosus Disease Activity Index 2000; BDI: Beck Depression Inventory; CT: cardiovascular exercise; RT: resistance exercise; SCL-90-R: The Symptom Checklist 90-Revised; SLAM-R: The Systemic Lupus Activity Measure-Revised; SLAQ: Systemic lupus activity questionnaire for population studies; SMS: symptom monitoring support intervention; CES-D: The Center for Epidemiological Studies Depression scale; STRESS: Cohen’s Perceived Stress Scale; ASES: Arthritis Self-Efficacy Scale; AIMS2-pain: The Revised Arthritis Impact Measurement Scales; MPI: Multidimensional Pain Inventory; SVI: Stress Vulnerability Inventory; STAI: Spielberger’s State-Trait Anxiety Inventory; SF-MPQ: The McGill Pain Questionnaire - Short Form; PedsQL: Pediatric Health-related Quality of Life; GHQ- 28: The self-reported General Health Questionnaire; CBT: cognitive-behavioral therapy; MBCT: Mindfulness-based cognitive therapy.
Fatigue
The effect of non-pharmacologic interventions on fatigue was evaluated in six studies.13–15,18,22,27 Sample sizes ranged from 10 to 122 with a total of 332 subjects. In four studies, all subjects were female.13–15,18 In the remaining two studies, the majority of the subjects were female, 98% and 96%.22,27 Of the six studies, four used exercise interventions (two home exercise, two aerobic exercise), one used psychological intervention (psychoeducation) and one used electro-acupuncture. The fatigue outcome measurement tools used in these studies were the Fatigue Severity Scale (FSS), Chalder Fatigue Scale, Visual Analog Scale, the Profile of Mood States, Short-Form Health Survey (SF-36) vitality, and one study used a fatigue scale designed specifically for lupus patients. 22 Compared with the control conditions, non-pharmacologic interventions were associated with a significant improvement in fatigue in three out of six studies (two exercise and one psychological intervention).
Four studies evaluated the effects of exercise on fatigue. Two studies used home exercise intervention and two studies used aerobic exercise intervention. Both home exercise studies demonstrated the potential benefit on fatigue.13,15 The two RCTs evaluating aerobic exercise revealed no significant difference in fatigue measured by the FSS compared with muscle strengthening or isotonic exercises.14,18 However, both studies demonstrated statistically significant improvement in fatigue after the implementation of physical activity intervention in both aerobic and isotonic exercise groups.
The RCT examined the effect of 5 months of a psychoeducation intervention on fatigue in SLE patients and showed statistically significant reduction in fatigue score measured by a fatigue scale designed specifically for lupus patients in the experimental group compared with the attention placebo control. 22 In a study of electro-acupuncture intervention, 5 weeks of electro-acupuncture may improve fatigue compared with usual medical care control but was not statistically significant. 27
Depression
Eight RCTs evaluated the benefits of mind-body interventions on depression or psychological function in SLE patients.13,15,18,19,21,23,24,26 Sample sizes ranged from 23 to 133 with a total of 555 subjects. A majority of study subjects were female (67–100%) with four studies including only female subjects.13,15,18,21 These studies used various forms of the evaluation instruments including the National Institutes of Mental Health Depression Scale, Hospital Anxiety and Depression Scale, Beck Depression Inventory, Symptom Checklist 90-Revised (SCL-90-R), Center for Epidemiological Studies Depression scale, Cohen’s Perceived Stress Scale, Stress Vulnerability Inventory, Spielberger’s State-Trait Anxiety Inventory, and self-reported General Health Questionnaire (GHQ-28).
Of the eight studies, four used exercise interventions (two home exercise, two aerobic exercise) and four used psychological interventions (one group psychotherapy, two CBT with relaxation techniques, one MBCT). Out of these eight studies, three studies reported improved psychological function. These three positive studies used psychological interventions including biofeedback-assisted CBT, CBT, and MBCT. An RCT using biofeedback-assisted CBT intervention observed a greater improvement in psychological function compared with the control and the symptom monitoring support intervention and the improvements in psychological function persisted at 9-month follow up. 23 Another RCT using MBCT intervention also reported similar results. The study reported significant improvement in psychological symptoms measured by GHQ-28 and mental health domains of the SF-36 in MBCT groups immediately after the intervention and at 6 months follow up. 26 Similar positive findings of CBT demonstrated improvement in stress, anxiety, and depression after the intervention compared with patients in a no-intervention control. In addition, patients in the CBT also benefited in mental health domains of the SF-36. 24
In contrast, five studies found no improvement in emotional health after interventions. An RCT by Dobkin did not demonstrate a significant benefit in the psychotherapy group using the psychological measuring instruments (SCL-90-R) for SLE patients. 21 This study did not find any clinically important improvement in any of the parameters including psychological distress, quality of life, and disease activity compared with usual care. All four studies on exercise interventions did not demonstrate benefit in psychological function in SLE patients compared with the control group.13,15,18,19 However, an RCT by Bogdanovic et al. used isotonic exercise as a control group and showed significant improvement in depression after all physical activity interventions in both experiment and the control group. 18
Pain
Three studies (two CBT and one electro-acupuncture) involving 169 patients evaluated pain.23,25,27 The pain evaluation instruments used in these trials were the Revised Arthritis Impact Measurement Scale-Pain Subscale (AIMS2-Pain), the Multidimensional Pain Inventory (MPI), the Bodily Pain scale of the SF-36 (SF-36 BP) and the McGill Pain Questionnaire - Short Form (SF-MPQ). One out of three studies reported pain reduction after interventions. 23 The study of 3 months of biofeedback-assisted CBT with relaxation techniques revealed the CBT intervention significantly greater reductions in pain measured by the AIMS2-Pain and MPI compared with the control group. 23 In contrast, the study by Brown et al. found that when compared with the control group, the patients in the CBT with a home computer module group had no improvement in pain measured by the SF-MPQ. However, this study did not find any significant improvement in any outcomes. 25 The third RCT evaluated the effect of 5 weeks of electro-acupuncture intervention by using the AIMS2-Pain, MPI, and the SF-36 BP to assess pain severity found that electro-acupuncture is feasible and safe, and may be of benefit for reducing pain. However, this pilot study did not have the appropriate sample size and power to determine the statistical significance of treatment benefits. 27
Quality of life
A total of 11 studies with 752 participants assessed quality of life of SLE patients before and after non-pharmacologic interventions.14,15,18–26 Six studies involved only female subjects and majority of the SLE subjects evaluated in other studies were female. Five studies on exercise interventions (one home exercise, four aerobic exercise) and six studies on psychological interventions (one group psychotherapy, three CBT, one psychoeducation, one MBCT) were identified. Ten studies used SF-36 to evaluate quality of life. One study used only the SF-36 physical function subscale. 14 One study used the Pediatric Health-related Quality of Life (PedsQL) as a measurement tool. 25 The results of these studies showed that seven out of 11 studies (three aerobic exercise, four psychological interventions) indicated improvement in at least one subscale of quality of life as measured by SF-36, compared with control. Four studies (one aerobic exercise, one home exercise, two psychological interventions) showed no significant improvement in any subscales of quality of life between the intervention groups and control groups.
Five studies evaluated the effects of exercise interventions on quality of life. Three out of these five studies demonstrated the benefit of exercise on quality of life. All of these three studies used aerobic exercise intervention. Bogdanovic et al reported that 6 weeks of aerobic exercise significantly improved in pain, general health and mental health subscales of SF-36 compared with isotonic exercises control. 18 A three-armed, RCT reported similar results. Compared with the resistant exercise and no intervention control, 12 weeks of cardiovascular exercise statistically significantly improved on the role physical and vitality subscales of SF-36 scores. 19 These two studies also showed that the patients in both exercise groups had significant improvement of all areas of quality of life measured by the SF-36 after physical activity intervention compared with baseline.18,19 In addition, an RCT of aerobic exercise intervention followed by self-managed physical activity provided improvements in mental health subscale of SF-36 compared with no intervention control. 20 In contrast, these findings were not confirmed in the other two exercise studies.14,15 There were interesting points to address in these two negative studies. One study evaluated only physical function subscale of SF-36 and used a strength-training exercise as a control group. However, in this study the authors observed that both aerobic and strength-training exercises showed improvement in SF-36 physical function subscale after exercise intervention but no significant different between groups. 14 Another study allocated 93 SLE patients to three groups (home exercise, relaxation, and control). This was the only study that evaluated the effect of home exercise intervention on quality of life. The authors reported no significant differences in SF-36 physical function, role physical and vitality subscales between the groups after 12 weeks of intervention. 15 We may conclude that aerobic exercise intervention improved quality of life in SLE patients. The effect of home exercise on quality of life remains unclear.
Six studies evaluated the beneficial effects of psychological interventions on quality of life. Four of the studies (one psychoeducation, two CBT, one MBCT) indicated improvement in at least one of the SF-36 subscales.22–24,26 This is in contrast to the results from two RCTs that could not demonstrate the benefit of psychological interventions on quality of life.21,25 One RCT evaluated quality of life measured by SF-36 after 3 months of psychoeducation intervention. 21 Another RCT used CBT with home-computer modules. This study used the PedsQL as a measurement tool. 25 However, these two studies did not find any clinically important improvement in any of the outcomes.
Disease activity
Twelve RCTs examined the effects of non-pharmacologic interventions on SLE disease activity in a total of 687 SLE patients.13–17,19–24,27 Seven studies used exercise interventions (two home exercise, five aerobic exercise) and four used psychological interventions (one group psychotherapy, two CBT, one psychoeducation) and one used electro-acupuncture. Indices for assessing SLE disease activity that used in these studies were SLE lupus activity index, Systemic Lupus Activity Measure (SLAM), Systemic Lupus Erythematosus Disease Activity Index (SLEDAI), SLEDAI 2000, SLAM Revised (SLAM-R) and Systemic Lupus Activity Questionnaire for population studies. None of the studies demonstrated an improvement in disease activity with 5 to 52 weeks of non-pharmacologic interventions.
Discussion
Our review indicated that several non-pharmacologic treatments showed promising results as adjuncts to current medical therapy for improving fatigue, depression, pain, and quality of life. However, none of the interventions demonstrated a decrease in SLE disease activity.
Fatigue is the most prevalent symptom in SLE and affects up to 80% of patients 28 with approximately 50% of patients considering fatigue their most disabling disease symptom. 29 Fatigue in SLE is complex with multifaceted origins including disease activity, mood disorders, sleep disturbance, physical inactivity, and chronic pain.2,28,30–34 Our study found that non-pharmacological interventions were associated with a significant improvement in fatigue, particularly the exercise intervention with home exercise the preferable method. Our review also suggested that psychological interventions improved depression and pain, which also have a profound impact on fatigue. Non-pharmacologic therapies may be adjunctive options for improving fatigue patients with SLE.
Several studies show the quality of life in patients with SLE is lower than in the general population. 6 Pharmacologic treatments that are effective for SLE disease activity may not improve quality of life in SLE patients because quality of life is an independent outcome from SLE disease activity. 35 The patients and physicians may rate SLE disease activity differently 36 with patients prioritizing quality of life over physician-derived outcomes, resulting in an unacceptable persistence of care needs not being met. Our study provides important evidence to support aerobic exercise and psychological interventions as efficacious options for promoting overall quality of life in patients with SLE. The effect of home exercise on quality of life remains unclear.
In our review, there was only one mind-body practice (acupuncture) study that met inclusion criteria. This study did not have the appropriate sample size and power to determine statistical significance of treatment benefits. However, the non-pharmacologic interventions in this review are multifaceted and include several components. The mind-body component including mindfulness-based meditation are among the most frequently used mind-body interventions in SLE; however, evidence to support these practices in SLE is still lacking. 9 Although there was one MBCT study that found considerable improvement in psychological symptoms and quality of life in patients with SLE, 26 to date there is no study of mindfulness-based stress reduction (MBSR) training, one of the most recognized forms of relaxation or mindfulness-based training as developed by Kabat-Zinn. 37
Tai chi and yoga are also widely used mind-body interventions. Although the effectiveness of tai chi has been demonstrated in RCTs and observational studies in various rheumatic conditions such as osteoarthritis, rheumatoid arthritis, and fibromyalgia, 38 its impact on patient-reported outcomes has not been evaluated in SLE patients. Yoga has also yet to be studied in SLE patients. This indicates the need for further research to evaluate the effects of the complementary or integrative therapies including MBSR, tai chi, and yoga given the lack of existing literature in this area uncovered by this study.
Strengths and limitations
Strengths
The previous reviews of non-pharmacologic interventions in SLE have included quasi-RCT, non-RCT, and prospective observational studies. Our review was limited to RCTs and we included additional articles that were not used in previous reviews. A strength of this review is that we included a wide variety of non-pharmacologic interventions including exercise, psychological interventions, and acupuncture. In addition, mind-body interventions for SLE have not been included in previous reviews of exercise or psychological interventions. This review also examined a wide variety of outcomes including fatigue, depression, pain, quality of life, and disease activity, presenting a fuller picture of the potential benefits of these interventions.
Limitations
Many studies of non-pharmacologic interventions lack rigorous scientific methods and randomized control design, and have a small sample size. The duration of non-pharmacologic interventions in most studies we evaluated was short. Therefore, long-term effects of non-pharmacologic interventions are still unknown. The length and intensity of interventions should be evaluated to determine the optimal dose. It is also difficult to obtain overall quantitative estimates of treatment effects due to the heterogeneity of details of the intervention, and outcome definitions and measurements. Most of the outcome measures in these studies are not disease specific. Other co-morbidities and medications can confound the results. Choice of comparison groups in RCTs is a study design element that deserves careful consideration. Several studies used different types of exercise, education or relaxation interventions for the control group.13–15,18,19,22,23,25 These control interventions sometimes prove to be efficacious and affect the outcomes so it is critical to specify the components of the comparisons. Engagement in non-pharmacologic interventions outside of the research setting is likely to enhance treatment effects both during and following study interventions. In addition, the mechanisms of the benefits from these interventions in SLE patients are not well understood.
Conclusion
This review showed promising results for physical exercise and psychological interventions as adjuncts to traditional medical therapy for improving fatigue, depression, pain and quality of life. However, many studies had small sample sizes and short intervention durations. Importantly, many complementary and alternative therapies with proven benefit in other rheumatic diseases have not been evaluated. Future high-quality RCT studies that examine specific components of interventions, report effectiveness, short- and long-term risks, and benefits of these non-pharmacologic interventions for SLE patients are needed to better integrate these interventions into the care of the SLE patient population. In addition, future studies should attempt to measure engagement in non-pharmacologic treatments outside of the research setting such as home practice, and conduct follow-up assessments to evaluate the impact of continued practice on symptoms.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Center for Complementary and Integrative Health (K24AT007323 and K23AT009374) (CW and RB) and National Center for Advancing Translational Sciences (1KL2TR002545) (SK) at the National Institutes of Health. The contents of this manuscript are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.