
Abstract
Introduction
Registries are essential to keep track of systemic lupus erythematosus (SLE) epidemiology and to provide better care to patients. The Colombian Ministry of Health has adopted a registry (SISPRO) to gather comprehensive information coming from the Colombian health system, which provides close to universal coverage (around 95%). The information collected from SISPRO is available for scientific analysis.
Objectives
We used data collected by SISPRO to estimate prevalence and specific characteristics of patients with SLE registered from January 2012 to December 2016.
Methods
This is a descriptive epidemiological study using the International Statistical Classification of Diseases and Related Health Problems as search terms related to SLE, based on SISPRO data. Criteria for diagnosis are not explicitly addressed in each individual case.
Results
National records report 41,804 patients with a diagnosis of SLE for an estimated prevalence of 91.9/100,000 subjects (based on a total population of 47,663,162), being more frequent in women (89% cases). When adjusted, female and male prevalences were 204.3 and 20.2 per 100,000 (ratio 10.1) with a 7.9:1 female:male ratio, and were highest in the 45–49-year age group.
Conclusions
This is the first study that describes demographic characteristics of SLE in Colombia, with useful information for decision makers. It also suggests a similar prevalence to other countries.
Introduction
Prevalence of systemic lupus erythematosus (SLE) and other autoimmune diseases (multiple sclerosis, rheumatoid arthritis, among others) seems to be increasing due both to a better diagnosis and increased survival of patients.1,2 Registries are essential to keep track of the local epidemiology and to provide better care for all affected individuals. The Latin American Group for the Study of Lupus (GLADEL, by its Spanish acronym) has made academic and research efforts to better understand the etiopathogenic, clinical and epidemiological aspects of SLE in our region. To contribute towards this goal, we present this study based on official statistics to obtain demographic information on Colombian patients with SLE.
Methods
Colombia has a health system based on single payer public funding and mixed private and public provision, with close to universal coverage (around 95%); the remaining are mostly minorities or informal sector workers that do not approach the health system or demand services. 3 The Colombian Ministry of Health has developed a tool to collect and store information, called Integrated Social Protection Information System (SISPRO, by its Spanish acronym); this system has four components: Health, Pensions, Occupational Risks, and Social Promotion. The basic data that the health system requires for management, regulation and control processes are stored and processed in the Health component. These processes are managed based on the Individual Registry of Health Services Delivery (RIPS, by its Spanish acronym). The information in these databases is available for research purposes. Through these online dynamic tables of the Ministry of Health we obtained the data from 1 January 2012 to 31 December 2016 period. Following the STROBE guidelines for observational studies (see checklist in Supplementary Material), we analyzed the RIPS databases using the codes of the International Classification of Diseases (ICD-10) for SLE (M320, M321, M328, M329). Variables such as gender, type of insurance and distribution in five-year age groups were used to estimate prevalence, using as denominators the official projections of the National Administrative Department of Statistics (DANE), based on data from the last 2005 national census. 4 Prevalence was adjusted by gender and age group to the 2014 Colombian population using the direct method, for each of the 32 Colombian political divisions (departments), during the five-year period analyzed, using the average population of the period. Results are presented as prevalences per 100,000 population, or as percentages, for qualitative variables. Diagnostic criteria for SLE in the SISPRO database are clearly not standardized, and depend on each physician. Additionally, only the “main diagnosis” is included, which could potentially lead to under reporting in patients with multiple diagnoses, but we could assume SLE should classify as main diagnosis in most, if not all, cases. It is important to highlight that the coverage of the Colombian health system is one of the highest in Latin America (45.2 million of the 47.6 million estimated Colombian population), according to the last official measurement by the Ministry of Health in 2017. 5 This high rate of coverage is important to highlight because, being almost universal, it allows us to infer that there are few patients with SLE that would be beyond the scope of this study.
Results
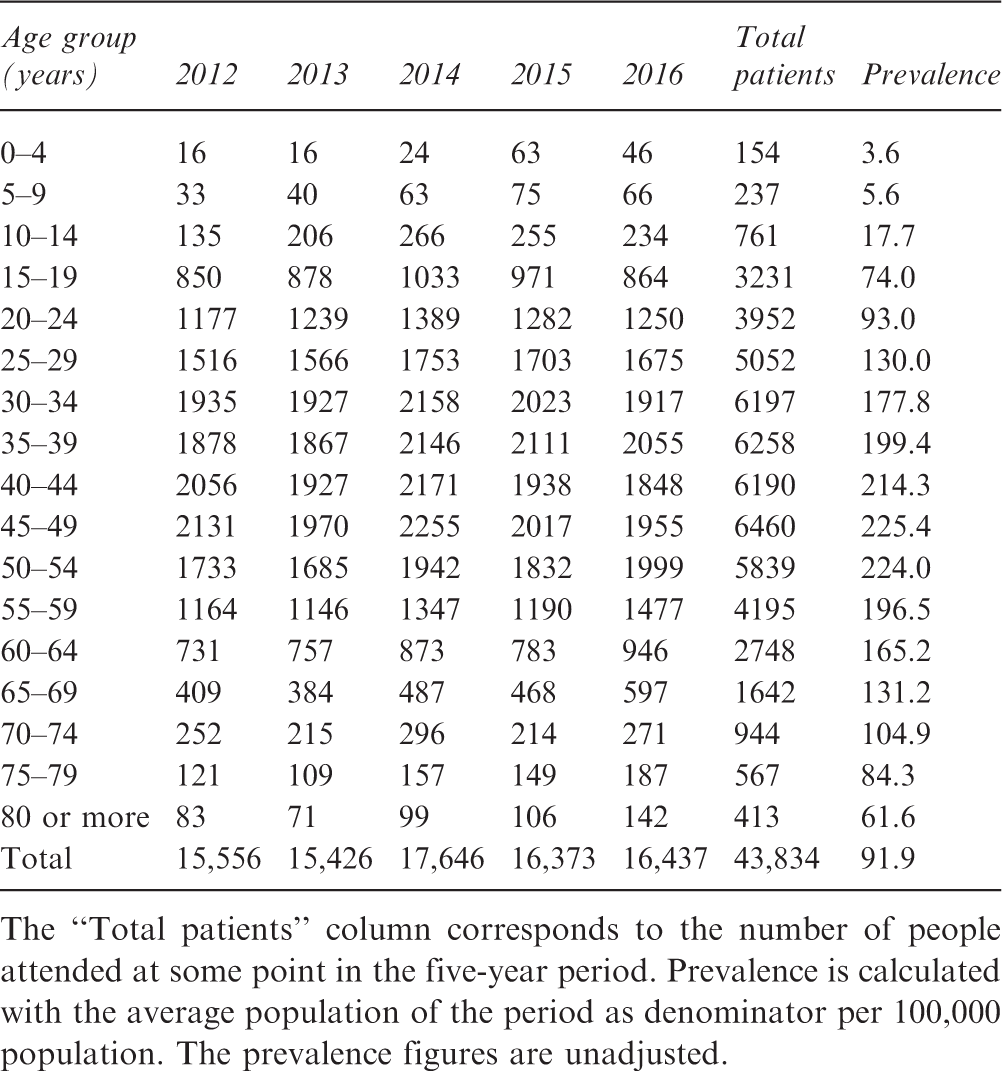
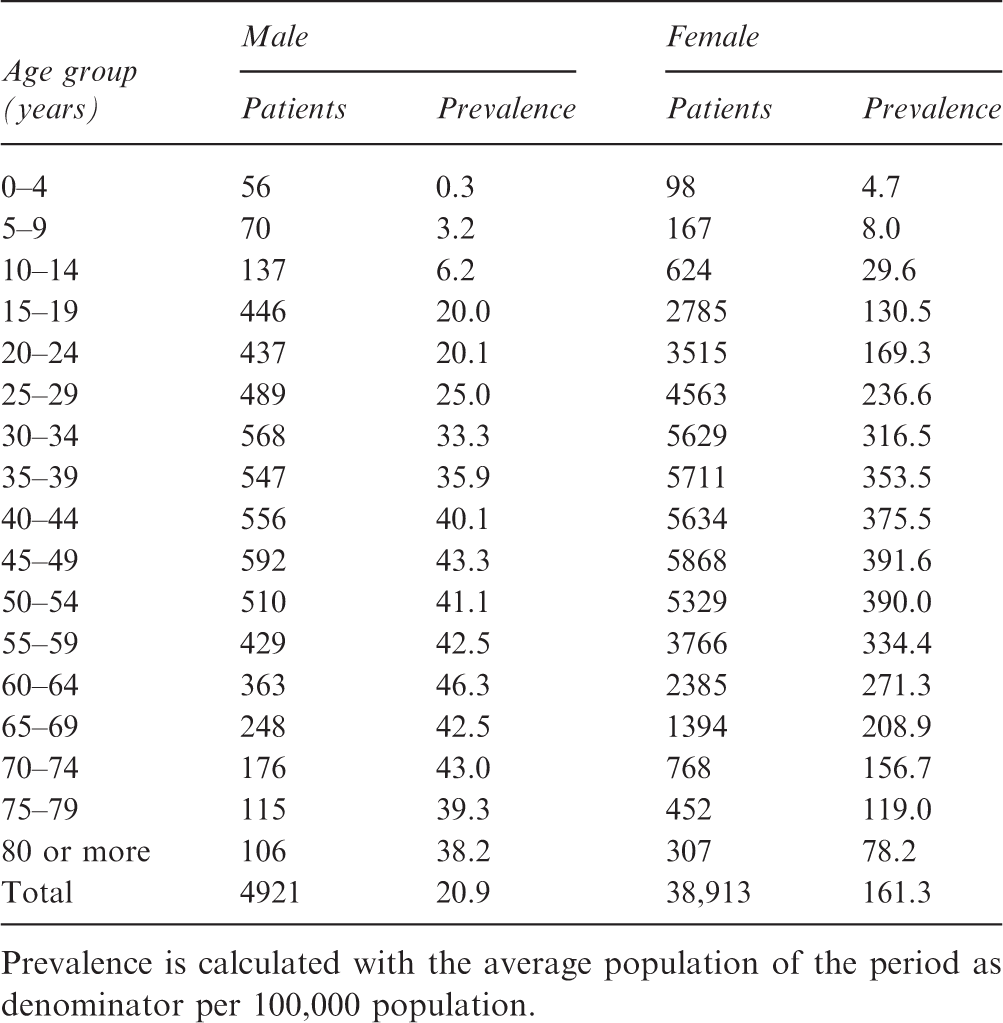
We identified 431,834 cases (“people attended”) with a primary diagnosis of SLE during the five-year period. The average estimated population during the five-year period was 47,663,162. This allowed us to calculate a five-year period unadjusted prevalence of 91.9 cases per 100,000 population, and 126.3 per 100,000 population in the population over 18 years of age (Table 1). When adjusted to the 2014 World Health Organization (WHO) world population, the female and male prevalence rates were 204.3 and 20.2 per 100,000, respectively. Women account for 89% of cases, with a 7.9:1 female:male ratio (10.1:1 when adjusted to the WHO population). When analyzing the prevalence for each five-year age group, we found a progressive increase, reaching the highest unadjusted prevalence in the 45–49-year group (Figure 1 and Table 1), and in the 50–54-year age group when adjusted to the world population. The number of patients in each age group by gender, as well as their prevalence, are presented in (Table 2). Due to the characteristics of the registry, and the fact that what is considered as “main diagnosis” in one year may vary in the next one, incidence rate estimation or duration of the disease are not believed to be accurate.
6
Age-specific unadjusted prevalence of patients with systemic lupus erythematosus during the years 2012–2016. Number of patients with a main diagnosis of systemic lupus erythematosus according to age group between 2012 and 2016. The “Total patients” column corresponds to the number of people attended at some point in the five-year period. Prevalence is calculated with the average population of the period as denominator per 100,000 population. The prevalence figures are unadjusted. Number of patients with a main diagnosis of systemic lupus erythematosus according to sex and age group between 2012 and 2016. Prevalence is calculated with the average population of the period as denominator per 100,000 population.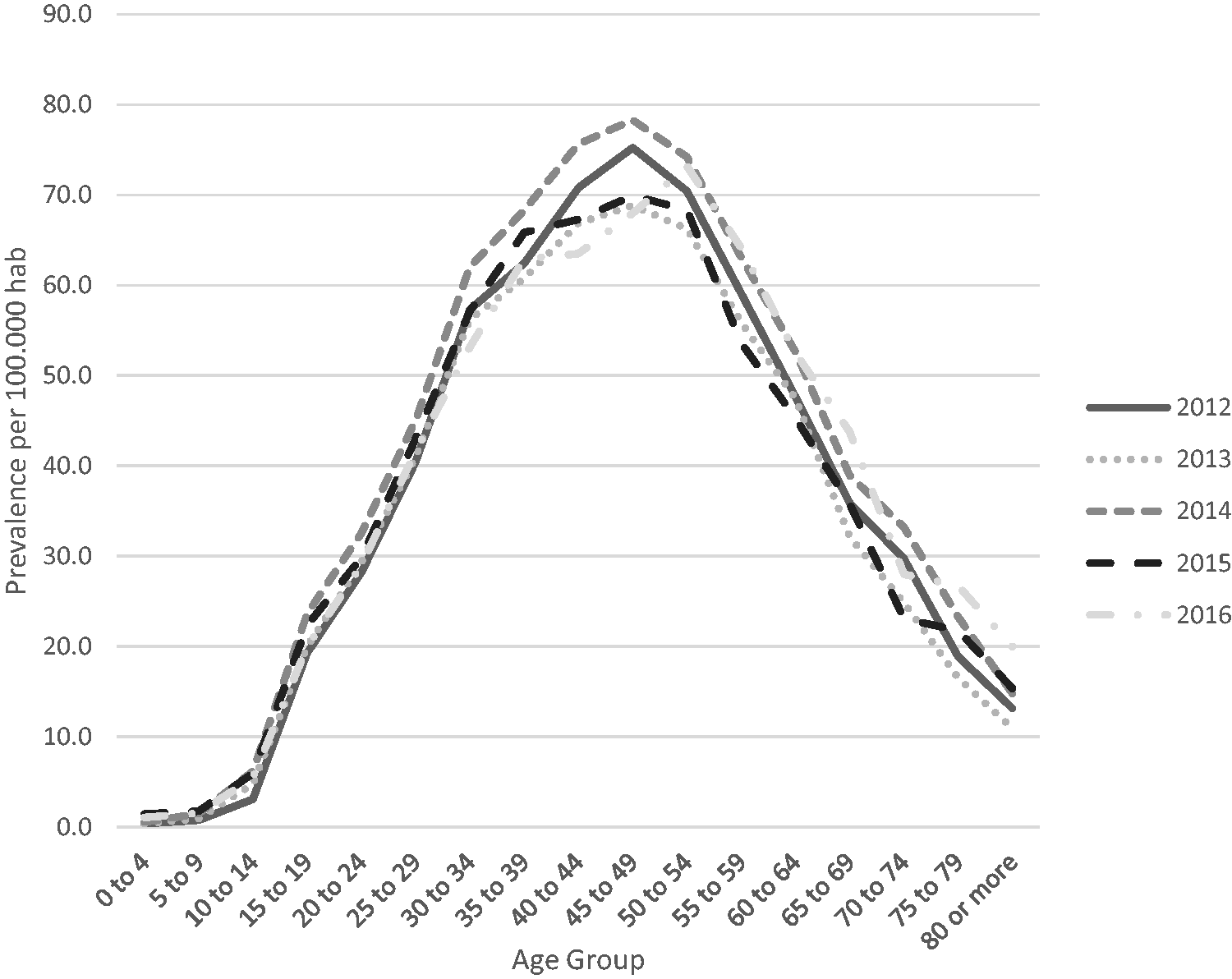
When analyzing the type of coverage they have according to the health insurance regime, we found that the majority of SLE patients belong to the contributory regime (72.9%), which represent nationals with a higher income, followed by the subsidized regime (23.3%), mostly for the less well off. Private health insurance plans represented 3.3% of patients; special regimes, which mostly cover the military, were the remaining 0.5%.
Regarding the distribution of SLE by departments, we found that the male-adjusted prevalence ranges from 0 to 46 per 100,000 population, and the female-adjusted prevalence from 7 to 346 per 100,000 population (see Figure 2). The departments with the highest industrial development seem to have the highest prevalence; these are the capital district of Bogotá, Antioquia and Valle del Cauca, where Colombia’s three largest cities are located. The departments of the regions of Orinoco (Arauca and Vichada), Amazonas (Guainía, Guaviare and Vaupés), Chocó and La Guajira have the lowest prevalence of the disease. The reason could be that they have a lower population density and less urban development, which implies less access to specialists, and therefore a lower probability of obtaining an accurate diagnosis.
Geographic distribution of the prevalence of systemic lupus erythematosus for the period by departments by gender and age group adjusted to the Colombian population.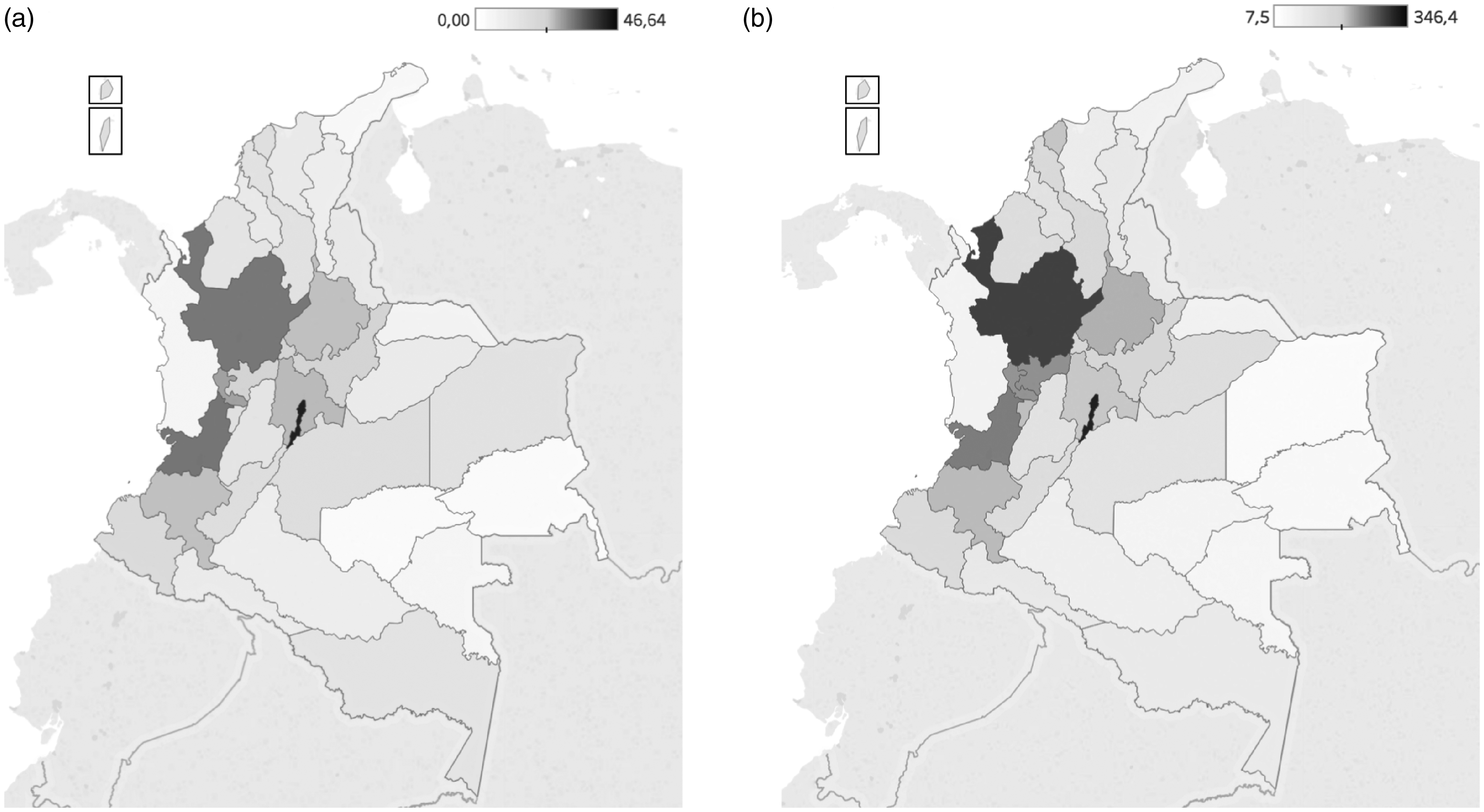
Discussion
Epidemiological and demographic characteristics of SLE vary from one country or region to the next. In Latin America, the Pan-American League Against Rheumatism (PANLAR) and GLADEL have made a joint effort to reach a deeper understanding of the characteristics of SLE in our populations. This has enabled us to have recommendations regarding the treatment of SLE from the perspective of Latin American rheumatologists. 7 This study adds to this Latin American initiative to improve knowledge about autoimmune diseases in our population. In Argentina, for example, the age group with the highest prevalence is the 40–50-year group, which is similar to what we found in our study. 8
Worldwide, the prevalence of SLE ranges from 20 to 178 cases per 100,000 population. A progressive increase of this wide range has been observed, and has been attributed to longer survival, as well as to earlier detection of mild to moderate varieties, as more is learned about the clinical spectrum of the disease.9–11 In Colombia, there is a big difference between patients affiliated to different insurance models. This could be explained by an earlier detection due to better access to specialized medicine, as well as longer survival due to timely treatment, associated with better economic conditions in those with the contributory regime, as compared with the subsidized regime group; this socioeconomic gap has been described by others.12,13
Studies by Pons-Estel et al. 9 in 2017 and by Petri 14 in 2002 compile the large studies on SLE, which show that there is a higher prevalence in certain regions and ethnic groups. When comparing this with our results, we observe that Colombia is in the group of countries with a high prevalence of SLE, surpassing regions known for their high prevalence, as is the case in Asia,9,14–16 where different prevalence data have been reported in different studies. One of these showed a range of prevalence between 4.3 and 45.3 cases per 100,000 population in the Pacific region. Another study found a prevalence of 50 cases per 100,000 population in Pakistan, and a third study showed a prevalence of 70 cases per 100,000 population in China.17–19 The prevalence of SLE in Europe varies widely, from 9 cases per 100,000 in Russia, to 69 cases per 100,000 in Sweden, the country with the highest prevalence reported in Europe, which is below the prevalence found in our study.20,21
The compilation by Lim et al. is interesting because of the way it breaks down the prevalence of SLE in the United States according to the ethnic characteristics of the population. It shows a prevalence in Arab Americans of 62.6 cases per 100,000 population, and in the African American population the prevalence increases to 178 cases per 100,000 population. 22 These results show the importance of ethnicity in the frequency of presentation of SLE, which is not only related to African American or Asian populations but also to Latin American population groups; this is very important, because there is also a high prevalence among them.10,14,23 These studies in which the demographic characteristics of SLE are analyzed by subgroups could be of importance in Latin America, because it cannot be said that our continent is a homogeneous region, but it has a wide ethnic, socioeconomic, educational and geographic variety, and these factors relate directly with the manifestations and prognosis of SLE.8,12,13
Regarding the female:male ratio, an average 9:1 ratio is mentioned, but changes noticeably with age, presumably reflecting the relationship with estrogen status. 24 The Euro-lupus study showed a 10:1 ratio, 25 similar to what is documented in our work. Other studies have found a maximum ratio of 13.6:1 in the study by Johnson et al. in 1995, and a lower one like that of Hopkinson et al. of 4.3:1.26,27 In general, studies conducted in Asia and Europe corroborate the difference in presentation between women and men; the data reported in our work are within the range usually documented.9,14,15 Interestingly, the female:male ratio is lowest in both extremes of life, as we found in our population, and has been documented elsewhere.24,28
Regarding the weaknesses of our study, it should be noted that, unlike studies conducted in other countries, we took data from the national registry of the Ministry of Health that includes patients diagnosed with SLE in which compliance with the classification criteria was not necessarily taken into account; this could overestimate the prevalence.
In addition, it is not possible to determine the ethnic group to which the patients belong, an important factor given the great ethnic variety of Colombia. It should be noted that it is difficult to compare the different epidemiological studies due to the different methodologies used to identify cases and estimate prevalence. However, this is an approximation from the statistics of the Colombian Ministry of Health, with which public health policy decisions are made, which is important for a disease that generates a great economic and social impact. More studies are needed to better characterize the clinical and demographic characteristics of SLE patients in Latin America.
Author's note
Diana N. Rincón-Riaño is now affiliated to Rheumatology Unit, Hospital Militar Central – Universidad Militar Nueva Granada, Bogotá, Colombia.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for Prevalence of systemic lupus erythematosus in Colombia: data from the national health registry 2012–2016
Supplemental Material for Prevalence of systemic lupus erythematosus in Colombia: data from the national health registry 2012–2016 by D G Fernández-Ávila, S Bernal-Macías, D N Rincón-Riaño, J M Gutiérrez Dávila and D Rosselli in Lupus
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.