
Abstract
In this study, we aimed to evaluate long-term patient survival according to demographic data, clinical manifestations of systemic lupus erythematosus (SLE) and previous and current treatments, collected retrospectively. Patient selection required a minimum of four American College of Rheumatology revised criteria for SLE, biopsy-proven lupus nephritis (LN) available for reclassification according to the modified National Institutes of Health proposal for activity and chronicity indices and a minimum follow-up of at least three years since the last renal biopsy. Selection criteria were fulfilled in 25 patients followed for a median of 21 years. Based on the last renal biopsy, an equal number of patients were thus classified as class I/II and IV (n=8) and class III and V (n = 4). The mortality rate for LN was 14%. Having ever been diagnosed with glomerulonephritis (GN) type III or type IV but not class IV alone (p = 0.046), a higher histological chronicity index at the last renal biopsy (p = 0.022), not attaining renal remission one year after induction therapy (p = 0.004), end-stage renal disease on dialysis (p = 0.033) and the extra-renal Systemic Lupus International Collaborating Clinics Damage Index score (p = 0.017) were all significantly associated with mortality. Our results may provide important clues for strict observation protocols in particular categories of LN patients with long-standing disease.
Introduction
Systemic lupus erythematosus (SLE) is a systemic autoimmune disease that overtly affects the kidney in approximately 30% of patients in Europe and in our own cohort.1,2 The aetiology of lupus nephritis (LN) remains obscure, with an unpredictable onset. While some patients with severe lupus lesions in other organs never develop renal disease, others may have a mild asymptomatic proteinuria or a fulminant onset with nephritis alone. 3 In a large inception cohort, despite current standard of care, LN was associated with end-stage renal disease (ESRD) and death. 4
Whereas for a correct diagnosis, with therapeutic implications, the importance of a diagnostic renal biopsy remains undisputed, whether the type of proliferative glomerulonephritis (GN) has an impact on the long-term prognosis remains controversial. Nevertheless, class IV nephritis has been traditionally associated with a more severe renal lesion than class III, 5 and a distinction between these classes of LN continues to be recommended by the International Society of Nephrology/Renal Pathology Society (ISN/RPS), in combination with scores reflecting acute and chronic tubulo-interstitial injury. 6 Reliable parameters associated with favourable renal outcomes, as well as those which disappointingly have been shown to have a poor/controversial predictive value, have been comprehensively reviewed recently. 7
In this study, we aimed to evaluate long-term patient survival according to demographic, clinical and histological features, including the most recently proposed modifications to the histological classification of LN, therapeutic strategies and outcomes.
Methods
Patient evaluation
The medical records of all patients were reviewed in December 2019. Patient selection required a minimum of four American College of Rheumatology revised criteria for SLE, 8 biopsy-proven LN recorded in the patient’s file according to the World Health Organization and 2004 ISN/RPS criteria5,9 and a minimum follow-up of at least three years since the last renal biopsy. Only those patients whose last renal biopsy was available for reclassification according to the modified National Institutes of Health proposal for activity and chronicity indices were included in the present data set. 6 Damage accrual was determined by the Systemic Lupus International Collaborating Clinics Damage Index (SDI) score, as previously described. 10 Treatment of the physician’s choice dictated the therapeutic approach, including the type of immunosuppression. Repeat renal biopsies were performed due to flares. Demographic data, clinical manifestations of SLE and previous and current treatments were identified. Ten patients with LN, all of whom were alive at the time of data retrieval, were excluded from this analysis because the renal biopsy could not be found or was not performed. Ethical approval was obtained from the Institutional Review Board (Centro Hospitalar Universitário de Lisboa Central protocol number 654/2018).
Statistical analysis
Continuous variables were recorded as medians (range or interquartile range (IQR)), and comparisons were made using the Mann–Whitney U-test. Dichotomous variables were examined by frequency distribution recorded as proportions, and comparisons were made using Fisher’s exact test. Cumulative survival curves were generated using Kaplan–Meier curves, and the difference between curves was compared using the log-rank test. Nominal two-sided p-values of <0.05 were considered statistically significant. Analyses were performed using IBM SPSS Statistics for Windows v23 (IBM Corp., Armonk, NY).
Results
Characteristics of the full cohort
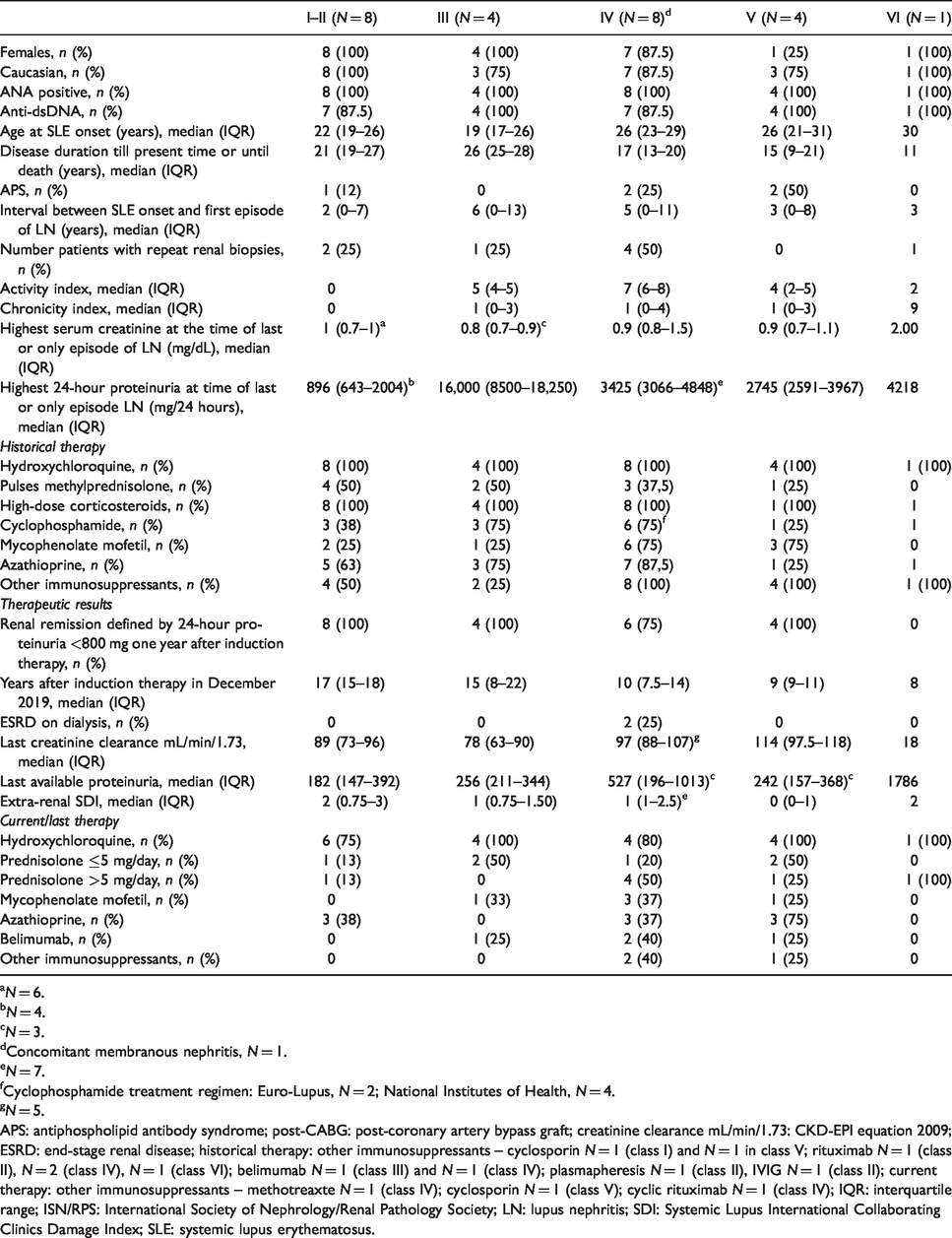
Between 1992 and 2016, 25/35 LN patients treated in our unit fulfilled the criteria for inclusion in the present study (demographic, clinical, histological and therapeutic descriptors in Table 1). The majority were Caucasian females, 100% ANA positive and 92% anti-dsDNA positive, with disease onset in early adulthood. The median follow-up was 21 years (IQR 13–25 years). Eight patients underwent repeat renal biopsies. These were repeated more than once in a single patient (class III and V to class II and then class IV+V) and also revealed changes in another two (class IV to class VI in one patient and class III to class II in another), with the rest maintaining the same GN classification. Based on the last renal biopsy, an equal number of patients were thus classified as class I/II and IV (n = 8) and class III and V (n = 4). The median interval between SLE onset and the first episode of LN was similar in classes III and IV (5–6 years), with class I/II and III patients presenting in earlier time frames (2–3 years). Activity and Chronicity indices are presented in Supplementary Table I.
Demographic, clinical, tubulo-interstitial, therapeutic parameters and response according to histological classification of glomerulonephritis (2004 ISN/RPS criteria).
aN = 6.
bN = 4.
cN = 3.
dConcomitant membranous nephritis, N = 1.
eN = 7.
fCyclophosphamide treatment regimen: Euro-Lupus, N = 2; National Institutes of Health, N = 4.
gN = 5.
APS: antiphospholipid antibody syndrome; post-CABG: post-coronary artery bypass graft; creatinine clearance mL/min/1.73: CKD-EPI equation 2009; ESRD: end-stage renal disease; historical therapy: other immunosuppressants – cyclosporin N = 1 (class I) and N = 1 in class V; rituximab N = 1 (class II), N = 2 (class IV), N = 1 (class VI); belimumab N = 1 (class III) and N = 1 (class IV); plasmapheresis N = 1 (class II), IVIG N = 1 (class II); current therapy: other immunosuppressants – methotreaxte N = 1 (class IV); cyclosporin N = 1 (class V); cyclic rituximab N = 1 (class IV); IQR: interquartile range; ISN/RPS: International Society of Nephrology/Renal Pathology Society; LN: lupus nephritis; SDI: Systemic Lupus International Collaborating Clinics Damage Index; SLE: systemic lupus erythematosus.
Renal remission defined by 24 hour proteinuria <800 mg one year after induction therapy was achieved in all but two patients with class IV GN. There was no record for the estimated glomerular filtration rate (eGFR) values for the patients on dialysis. At last follow-up visit, classes I and II and V presented no kidney damage, and class III presented a mild decrease in renal function. Historically, in most patients, induction therapy consisted of high-dose intravenous cyclophosphamide until 2007 replaced by the low-dose of either the cyclophosphamide (Euro-Lupus) regimen or mycophenolate mofetil, followed by maintenance regimens with long-term mycophenolate mofetil or azathioprine. Cyclophosphamide was also used in two patients with class II nephritis due to concomitant severe neuropsychiatric disease. Rituximab was not used in the 1990s when both class IV patients lost renal function, at a time when no other alternative therapies were available for the treatment of refractory disease. Angiotensin II-converting enzyme inhibitors or angiotensin receptor blockers were used in most patients (data not shown). Of note, hydroxychloroquine was prescribed to 100% of the patients historically, having been discontinued because of asymptomatic retinal toxicity (diagnosed in the setting of a dedicated ophthalmological screening program). We were unable to calculate cumulative corticosteroid use but documented that all the patients were treated historically with high-dose steroids in the initial phase of the induction regimen. The vast majority of patients (18/25) remained on immunosuppressive drugs, five on prednisolone equivalent >5 mg/day at last entry. Over the course of their disease, many patients required a switch in immunosuppressants, either due to adverse events or due to failure to control overall SLE disease activity. Final SDI revealed permanent damage accrual in the 18/25 (72%) patients.
Characteristics of patients who died
The mortality rate for LN was 14% (5/35; accounting for all the patients treated in the unit). A comparison between alive and deceased patients (Table 2) shows that demographic, auto-antibody profile, age of SLE onset and disease duration were very similar between both groups of patients. Having ever been diagnosed with GN type III or type IV but not class IV alone (p = 0.046), a higher chronicity histological index (p = 0.022), not attaining 24-hour proteinuria of <800 mg one year after induction therapy (p = 0.004), ESRD on dialysis (p = 0.033) and the extra-renal SDI score (p = 0.017) were all significantly associated with mortality. No other statistically significant associations with any other continuous or ordinal variable presented in Table 1 were found. Demographic, clinical, histological and therapeutic characteristics as well as detailed information as regards co-morbidities and circumstances that led to deaths are provided in Supplementary Tables S2 and S3. The Kaplan–Meier survival curve is shown for the present cohort (n = 25) as a function of disease duration (Figure 1(a)), statistically different according to the histological classes of GN obtained in the last renal biopsy (Figure 1(b)). Class III and IV GN patients exhibited a statistically significant poorer survival when compared to other classes of GN (Figure 1(c)). Failure to achieve remission after one year of induction therapy led to ESRD and a statistically significant difference in mortality (Figure 1(d)).
Demographic and clinical comparisons between alive and deceased patients.
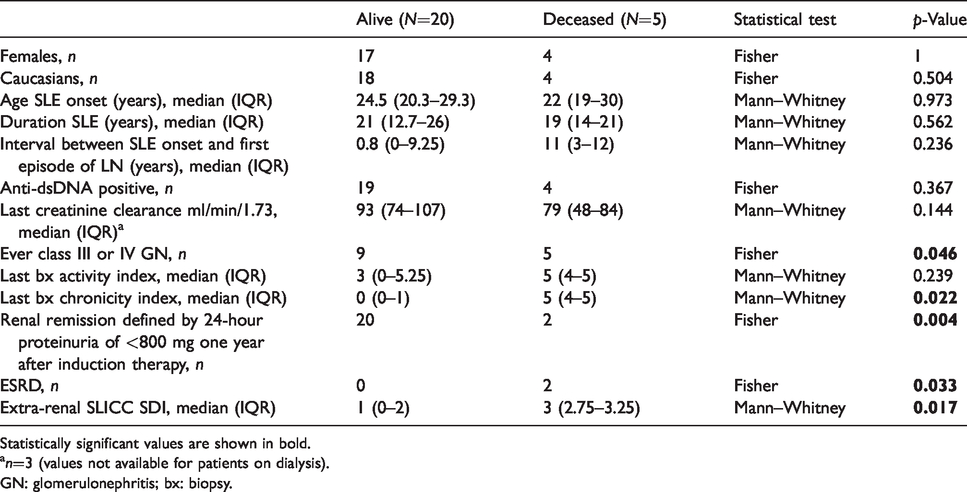
Statistically significant values are shown in bold.
an=3 (values not available for patients on dialysis).
GN: glomerulonephritis; bx: biopsy.
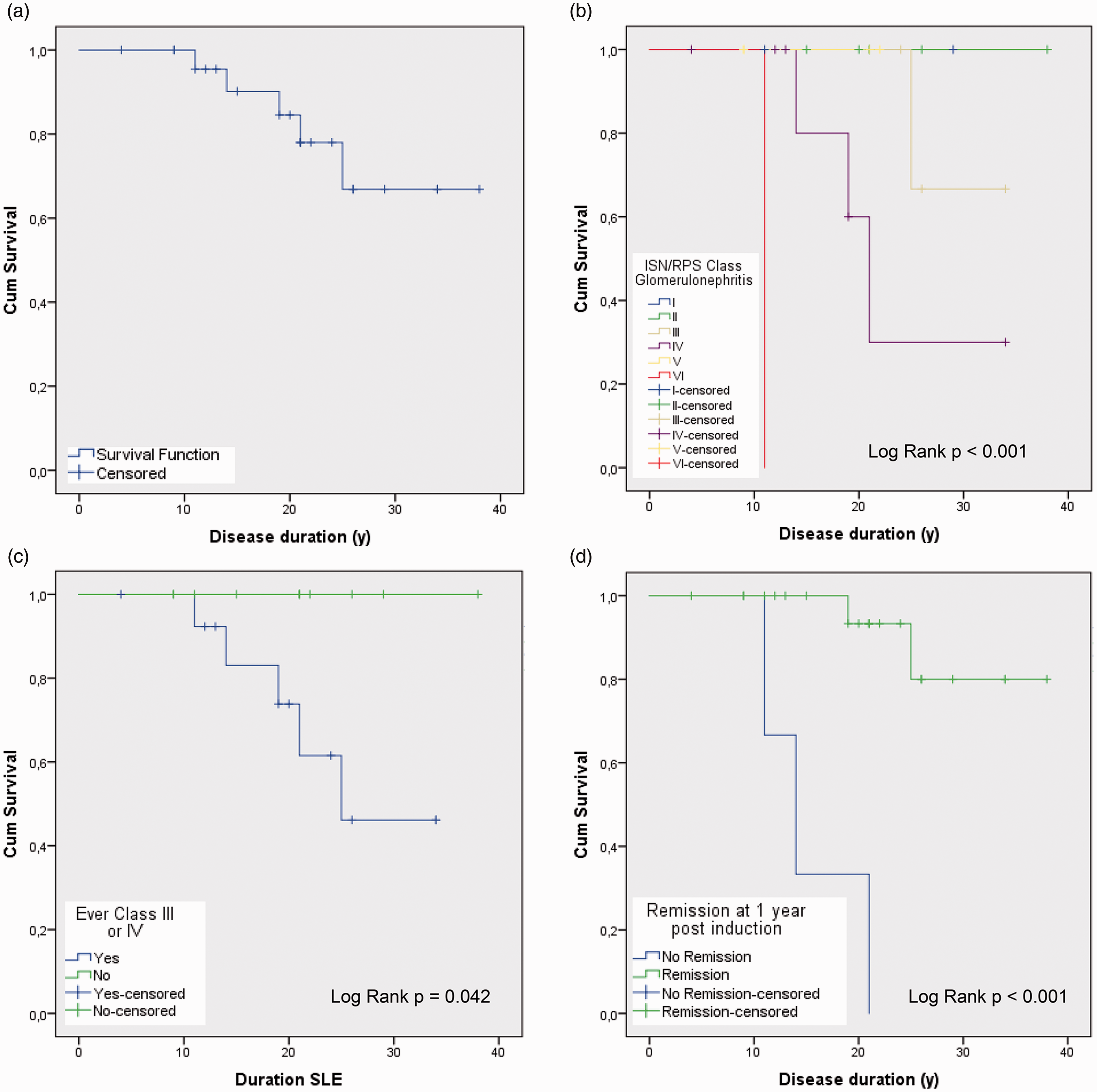
Survival curves. (a) Overall survival. (b) According to glomerulonephritis (GN) class. (c) Class III and IV GN versus other classes of GN. (d) Failure to achieve remission as defined by proteinuria at one year post induction therapy onset.
Discussion
The cumulative incidence of death at 10 years following the diagnosis of LN is currently reported between 6% and 8%.2,4 A longer disease duration is considered an independent risk factor for mortality, as corroborated in a multi-ethnic SLE cohort followed for up to 40 years, in which the cumulative incidence of death was 29%, strongly associated with damage accrual and target organ damage such as renal involvement. 11 In the latter, sepsis was the main cause of death, followed by cancer and cardiovascular events. The causes of death in our study follow a similar pattern, also associated to higher damage accrual. The dynamic nature of the disease, several therapeutic changes and ongoing use of immunosuppressants over a long follow-up period may have contributed to infection, cardiovascular disease and cancer, all of these reflecting the ongoing search for a definite cure for SLE.
The strengths of our study were a long follow-up and knowledge on extra-renal damage accrual. In addition to its retrospective nature and unstandardized therapeutic regimens, we recognize the major limitation to our study was the inability to identify predictors of mortality through a multivariate Cox regression analysis. It was therefore not possible to adjust for collinearity, an example of which is failing to achieve remission one year after induction therapy, occurring in the patients with class IV GN who then went on to develop ESRD. We nevertheless wish to point out that while the major obstacle to performing a Cox regression analysis was the overall small number of overall number of patients and deceased, the events that led to the patients’ deaths were not directly associated with LN. It could be argued that the effects of the predictor variables upon survival were not constant over time and not additive in one scale, and as such, a proportional regression model may not have been appropriate for modelling mortality in this cohort. We recognize that the log-rank test is univariate and may exaggerate the prognostic significance of a particular group and therefore interpret our results with caution.
Our data suggest increased long-term mortality for classes III and IV GN when compared to all other classes of GN, either class alone having no significant association. Likewise, a recent study of 98 patients found that upon treatment, after a mean follow-up of 6.4 years, renal parameters improved with the same kinetics and to the same extent in GN classes III and IV. 12
Endorsement of histomorphological indexes for evaluation of LN has been actively encouraged.6,13 Our results are in line with the observation that response to induction treatment with a reduction in proteinuria at one year forecasts good long-term renal prognosis, 14 extending this benefit to long-term survival.
Clinical presentation of LN has become less severe in the last years, leading to better long-term renal survival. 15 It is hoped that together with curative strategies, improved outcomes for SLE patients can be achieved.
Conclusion
Long-term prognosis in LN was associated with the histological differentiation of GN in the proliferative spectrum. The histological chronicity index and failure to achieve remission at one year after induction therapy were also associated with long-term mortality. While we recognize that this is a small series of patients and that there is a need for non-invasive and more specific biomarkers, our results may provide important clues for rigorous surveillance protocols in patients with long-standing disease.
Supplemental Material
sj-pdf-1-lup-10.1177_0961203320937472 - Supplemental material for Rubrics for mortality: a real-world observational long-term lupus nephritis cohort
Supplemental material, sj-pdf-1-lup-10.1177_0961203320937472 for Rubrics for mortality: a real-world observational long-term lupus nephritis cohort by Maria Francisca Moraes-Fontes, Ana Carolina Ferreira, Nuno Riso, Helena Viana and Fernanda Carvalho in Lupus
Footnotes
Acknowledgements
The authors thank the following colleagues: Bárbara Batista, Susana Escaria, Rui Isidoro and Filipe Morais Almeida for collecting patient data; Ana Catarina Rodrigues, Ana Lladó, Anna V. Taulaigo, António Panarra, Eunice Patarata, Filipa Lourenço, Heidi Gruner, Inês Figueiredo, Margarida Antunes, Melissa Fernandes, Sara Castro and Vera Bernardino for patient care; and António Panarra (Director Medicina 7.2) for ongoing support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.