
Abstract
Background
Despite the improvement in the live birth rate among patients with systemic lupus erythematosus (SLE), they are still at an increased risk of adverse pregnancy outcomes (APOs).
Objective
To determine the prevalence and factors associated with APOs in the multi-ethnic SLE populations in Malaysia.
Results
A total of 153 patients with 240 pregnancies were included and the majority of the patients were Malay (69.9%), followed by Chinese (24.2%) and Indian (5.9%). The prevalence of APOs was 61.7% with the commonest complication being prematurity (28.3%), followed by pregnancy loss (24.6%) and pre-eclampsia (21.8%). Logistic regression model-based GEE analysis revealed that the independent predictors of APOs were active haematological system during pregnancy, pre-pregnancy active disease, Indian patients and positive lupus anticoagulant. Hydroxychloroquine use was associated with lower APOs including pre-eclampsia, prematurity and IUGR in the univariate analyses but it was no longer significant in the GEE analysis.
Conclusion
The prevalence of APOs was high particularly among the Indian patients. Positive lupus anticoagulant and pre-pregnancy active disease were the factors strongly associated with APOs in our multi-ethnic cohort. Hydroxychloroquine may protect against APOs but further larger studies are needed to confirm this.
Introduction
Systemic lupus erythematosus (SLE) is characterised by production of autoantibodies resulting in inflammation of multiple organs with a relapse remitting pattern. 1 Malaysia is a multi-ethnic country and the prevalence of SLE was reported to be higher among Chinese (57/100,000), followed by Malays (33/100,000) and Indians (14/100,000). 2 In addition to that, involvement of the kidney (lupus nephritis (LN)) affects up to 70% of Malaysian SLE patients.2,3 In general, SLE affects women of childbearing age and pregnancy in SLE is associated with higher maternal and fetal risk. 4 However, the rate of live birth has improved from 60% in the published reports prior to 1990 to more than 80% in the more recent studies. 5 The improvement may reflect the enhancement of the overall care of pregnant women with SLE.
Despite improvement in the live birth rate, the number of maternal complications during pregnancy, including lupus flares (particularly LN), thrombotic event, pre-eclampsia, major infection and other haematological complications requiring transfusions (anaemia and thrombocytopaenia), are still high. 6 Maternal mortality was also reported to be 20-fold higher among women with SLE. 6 The most common fetal complications reported were fetal loss, prematurity, and intra-uterine growth restriction (IUGR) or small for gestational age.7,8
Predictors of adverse pregnancy outcomes (APOs) in SLE include active disease, use of antihypertensive agents, LN, 9 presence of antiphospholipid antibodies (aPLs),5,10 presence of anti-Ro and anti-La antibodies 11 and thrombocytopaenia.5,12 Women with SLE are also more likely to have comorbidities such as diabetes, hypertension and thrombophilia which are associated with APOs. 6 However, studies of pregnancy outcomes among SLE patients showed significant variations due to the differences in the study design and population characteristics.
The majority of the studies on the pregnancy outcomes among SLE patients were mainly from the predominant Caucasian patients in the USA, Canada and Europe. Studies in Asia were mainly from East Asia, namely Chinese,13–15 Korean16,17 and Japanese. 18 The influence of different ancestries in the pregnancy outcomes in lupus is not well studied due to lack of head-to-head comparisons. The LUMINA cohort of Hispanic, African American and Caucasian ethnicity showed higher APOs among Texan Hispanic and African American patients, but ethnicity was no longer a significant predictor of APOs in the multivariable model analysis. 19
Malaysia is a multi-ethnic country with a predominantly Malay ethnic, followed by Chinese and Indian ethnicities. Our study would like to determine the factors predicting poor pregnancy outcomes among our multi-ethnic SLE cohort.
Methodology
Subjects
This was a retrospective review of the consecutive SLE patients who attended the Rheumatology and Nephrology Clinic in Universiti Kebangsaan Malaysia Medical Centre and Hospital Putrajaya from January 2016 until December 2019. Patients with prior history of pregnancy/pregnancies with a complete pre-pregnancy, antenatal and intra-partum care at both centres were recruited. All patients fulfilled the 1997 American College of Rheumatology (ACR) classification criteria 20 or the 2012 Systemic Lupus International Collaborating Clinics classification criteria for SLE. 21 Each pregnancy was counted as a separate observation. All patients have given their informed consent and this study has obtained our institutional ethics committee approval, Universiti Kebangsaan Malaysia Medical Centre Ethics Committee (FF-2016-297).
Data collection and variables
Socio-demographic variables that were recorded include age at conception and ethnicity. Information on the SLE disease characteristics including age of onset, SLE duration at the time of conception and system or organ manifestations of SLE were obtained from the medical records. Immunologic characteristics such as anti-Ro/SSA, anti-La/SSB and aPLs (anticardiolipin, anti-β2 glycoprotein and lupus anticoagulant (LA)) were also determined from the medical records. Presence of other medical comorbidities such as hypertension, chronic kidney disease and thyroid dysfunction during pre-pregnancy were also recorded.
Renal involvement or LN was defined as present if patients met the ACR renal disorder criterion which is persistent proteinuria of more than 500 mg in 24 h 22 and/or had biopsy-proven LN. 23 Presence of any previous thrombotic events prior to pregnancy was also recorded and these include myocardial infarction, definite or classic angina, vascular procedure for myocardial infarction, stroke, peripheral arterial thrombosis and venous thrombosis (peripheral and/or visceral).
Pre-pregnancy, antenatal and pregnancy disease activity
The medical records were retrospectively analysed for SLE disease activity within 6 months of conception (pre-pregnancy disease activity) and during pregnancy. SLE Pregnancy Disease Activity Index (SLEPDAI) was used to assess the disease activity in pregnancy. 24 Disease remission was defined as a SLEPDAI score of 0 in the clinical items 25 with prednisolone dose of ≤10 mg daily. Complete LN remission was defined by proteinuria of <0.03 g/day. 26
APOs
For the purpose of this study, APOs included fetal adverse outcomes such as:
Early pregnancy loss which occurred during the first 13 weeks of pregnancy (the first trimester).
27
Late pregnancy loss (miscarriage occurred after 13 weeks of gestation) and intra-uterine death (fetal loss ≥20 weeks of gestation). IUGR and small for gestational age (birth weight below the 10th percentile). Premature birth (live birth before 37 weeks of gestation).
Maternal adverse outcomes included:
Pre-eclampsia based on new onset of both hypertension (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg) and proteinuria (≥300 mg of protein per 24-h urine collection, or protein to creatinine ratio ≥30 mg/mmol) after gestational week 20. Maternal death.
Treatment
Information on the use of immunosuppressive medications and hydroxychloroquine (HCQ) 3 months prior to conception and during the antenatal period and puerperium were obtained from the electronic prescriptions and medical records. The use of aspirin and low molecular weight heparin in pregnancy was also recorded. Since the impact of stopping HCQ on disease activity in pregnancy may take up to 2–3 months,
28
the level of exposure to HCQ among our subjects was divided into two groups:
Group 1: no exposure to HCQ treatment in the 3 months prior to pregnancy or stopped taking HCQ at any trimester of the pregnancy Group 2: took HCQ 3 months prior and throughout the pregnancy
Statistical analysis
Depending on the distribution of the data, the results were presented using mean (±standard deviation) or median (interquartile range) for quantitative variables and frequency (percentage) for qualitative variables. In all cases, p-values <0.05 were considered significant. The relationship between the APOs and variables from the different domains were then examined using standard descriptive statistical tests, the Student’s t-test or Mann–Whitney tests for continuous variables and the chi-squared test for the categorical variables. For comparisons of continuous variable between three or more groups, one-way analysis of variance was used for normally distributed variables while Kruskal–Wallis was used for non-normally distributed variables. Binary logistic regression analyses were conducted using generalised estimating equations (GEEs) to adjust for multiple pregnancies and possibility of APOs that may be correlated within a patient. All variables that were significant in univariate analyses with p<0.05 were included as independent variables in the model, in order to determine the predictors associated with APOs, including the specific fetal and maternal adverse outcomes. Analyses were performed using the SPSS (SPSS Inc., Chicago, Illinois, USA) package.
Results
A total of 153 patients with 240 pregnancies were included and analysed. Eight patients with eight pregnancies had to be excluded due to incomplete or inadequate data. Four patients were diagnosed to have SLE during pregnancy. The mean age at conception was 29.9 ± 4.8 years and the mean interval between diagnosis of SLE and conception was 7.1 ± 4.9 years. The majority of the patients were Malay (n = 107, 69.9%), followed by Chinese (n = 37, 24.2%) and Indian (n = 9, 5.9%).
More than two-thirds of the patients had musculoskeletal involvement of SLE, n = 118 (77.1%), while more than half of the patients had haematological (n = 92, 60.1%) and mucocutaneous SLE manifestations (n = 91, 59.5%). The haematological manifestations include leucopaenia (n = 35), autoimmune haemolytic anaemia (AIHA) (n = 26), thrombocytopaenia (n = 16), Evan’s syndrome (n = 10), pancytopaenia (n = 10) and thrombotic thrombocytopaenic purpura (TTP) (n = 2).
Approximately half of this cohort had LN, n = 75 (49.0%) and the majority of them had class IV with/without class V LN (n = 32/75, 42.7%). A total of 18 (11.8%) patients were diagnosed with antiphospholipid syndrome (APS). APS was significantly higher among Indian patients compared with Malay and Chinese with p = 0.03 (Table 1).
Demographics and disease characteristics among the multi-ethnic systemic lupus erythematosus patients.
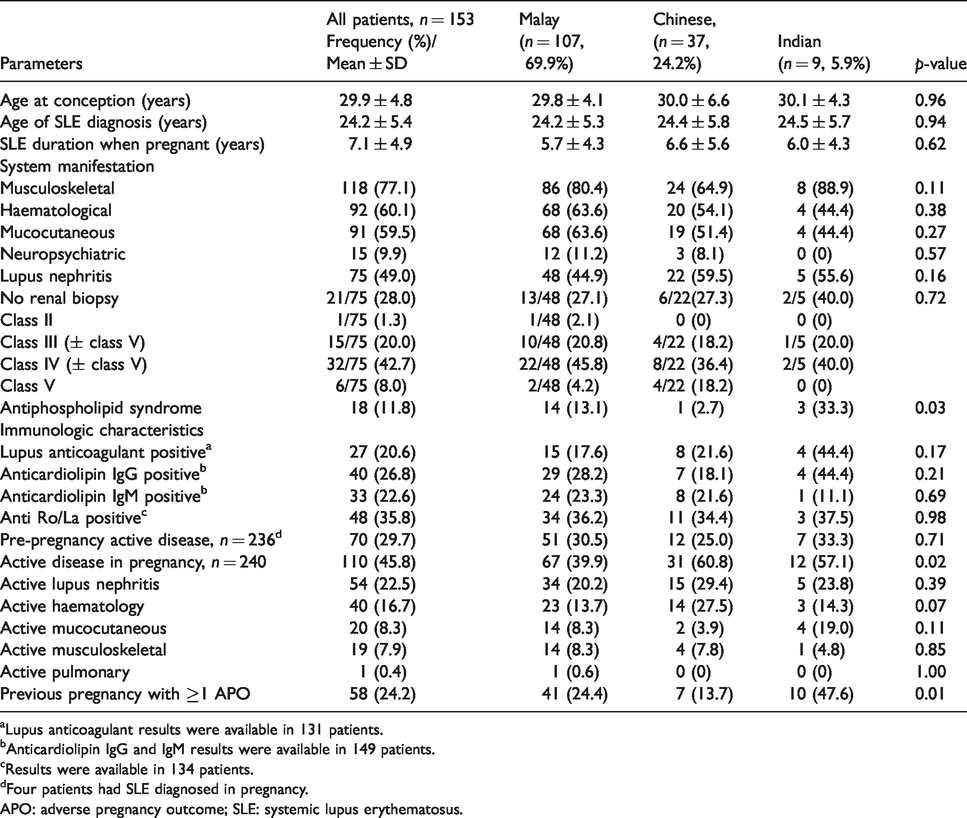
aLupus anticoagulant results were available in 131 patients.
bAnticardiolipin IgG and IgM results were available in 149 patients.
cResults were available in 134 patients.
dFour patients had SLE diagnosed in pregnancy.
APO: adverse pregnancy outcome; SLE: systemic lupus erythematosus.
In the 240 pregnancies, pre-pregnancy hypertension was present in 26.3% (n = 63) while 12 (5.0%) had prior thrombotic event, 7 (2.9%) had thyroid disorders, 5 (2.1%) had diabetes mellitus, 3 (1.3%) had chronic kidney disease, 2 (0.8%) had prior cerebrovascular accidents and 1 (0.4%) had ischaemic heart disease. A total of 58 (24.2%) pregnancies had prior history of APO which include fetal death >10 weeks (n = 22), recurrent miscarriages ≥2 before 10 weeks period of gestation (n = 21), pre-eclampsia (n = 13), prematurity (n = 10) and IUGR (n = 6).
In 236 pregnancies with pre-existing SLE prior to conception, 29.7% (n = 70) of them had active disease pre-pregnancy. The majority of them had active LN (35, 14.6%), followed by haematological (n = 25, 10.4%), mucocutaneous (n = 12, 5.0%) and musculoskeletal (n = 10, 4.2%). One patient who conceived while having active interstitial lung disease with severe restrictive pulmonary function had refused termination of pregnancy. A total of 152 pregnancies (64.4%) were planned and received pre-pregnancy counselling, including four patients who conceived when the disease was still active.
A total of 110 pregnancies (45.8%) had active SLE disease during pregnancy with a higher prevalence among Chinese patients with p = 0.02 (Table 1). The majority of the active disease occurred in renal (n = 54, 22.5%), followed by haematological (n = 40, 16.7%), mucocutaneous (n = 20, 8.3%), and musculoskeletal (n = 19, 7.9%). Thrombocytopaenia is the commonest haematological manifestation during pregnancy (n = 24) and one of them occurred concurrently with a severe impending eclampsia episode. However, this patient did not have deranged liver function. Other active haematological manifestations during pregnancy include leucopaenia (n = 12), AIHA (n = 2), Evan’s syndrome (n = 1), pancytopaenia (n = 1) and TTP (n = 1). Table 1 illustrates the demographic and disease characteristics among the SLE patients.
Less than half of the 236 pregnancies had a continuous HCQ treatment from 3 months pre-conception and throughout the pregnancy (n = 101, 42.7%). In the 240 pregnancies, a total of 73 (30.4%) had azathioprine treatment while 26 (10.8%) had cyclosporine and 23 (9.6%) had a combination of azathioprine and cyclosporine treatment in pregnancy. Low-dose aspirin during pregnancy was given in 78.3% (n = 188) of cases while 39.6% (n = 95) received low molecular weight heparin in pregnancy.
APOs and their associated factors
The prevalence of APOs was 61.7% (n = 148). The fetal loss rate was 24.6% (n = 59) with early trimester (≤13 weeks) fetal loss or miscarriage accounting for 16.3% (n = 39) and late trimester fetal loss the remaining 8.3% (n = 20). The prevalence of premature delivery was 28.3% (n = 68), followed by pre-eclampsia/eclampsia (n = 52, 21.8%), and IUGR (n = 42, 17.6%). Maternal death occurred in one patient due to worsening pneumonitis with sepsis.
APOs were significantly higher among those with longer disease duration and shorter duration of remission prior to conception (p < 0.05). A total of 90.5% pregnancies among ‘other’ ethnics (predominantly Indian) developed APOs compared with 58.8% and 58.9% in Chinese and Malay ethnics respectively (p < 0.05). Disease activity in pre-pregnancy and during pregnancy were significantly associated with APOs (all p < 0.05). However, patients who received HCQ treatment 3 months prior to conception and throughout the pregnancies had significantly lower APOs (p < 0.05).
Anticardiolipin IgG/IgM and LA results were available in 236 and 209 pregnancies respectively. Positive anticardiolipin IgG and LA were associated with higher prevalence of APOs (p < 0.05). In addition to that, positive anti-Smith was associated with significant APOs in this cohort (p < 0.05). Table 2 illustrates the factors associated with APOs among SLE patients in this study.
The associated factors of adverse pregnancy outcomes among systemic lupus erythematosus women.
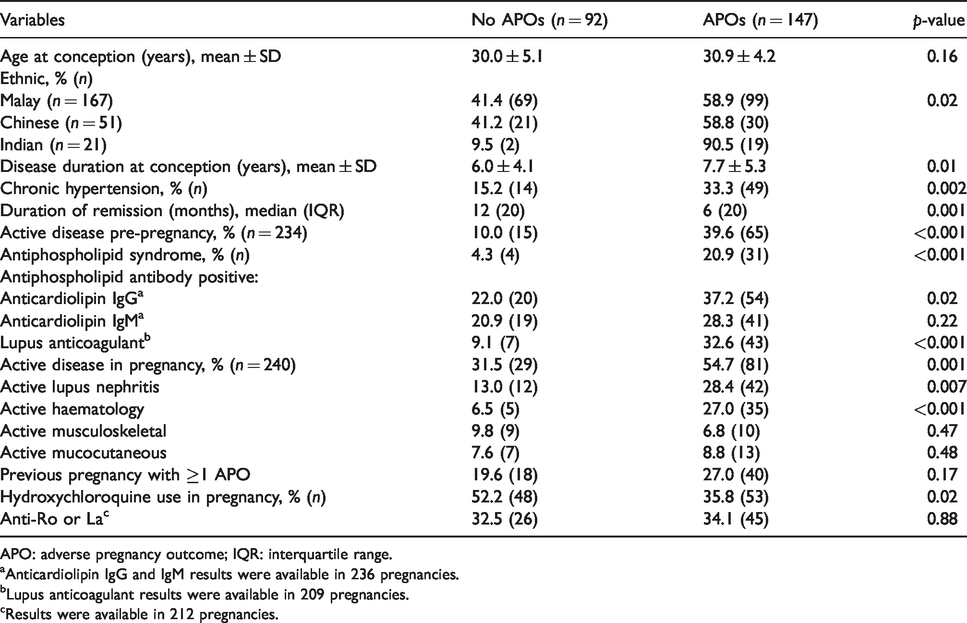
APO: adverse pregnancy outcome; IQR: interquartile range.
aAnticardiolipin IgG and IgM results were available in 236 pregnancies.
bLupus anticoagulant results were available in 209 pregnancies.
cResults were available in 212 pregnancies.
Logistic regression model-based GEEs were used to determine the independent predictors of APOs in our SLE cohort. From the analysis, the predictors of APOs were found to be active haematological system during pregnancy, pre-pregnancy active disease, Indian patients and positive LA. Table 3 illustrates the factors associated with APOs in our cohort of SLE patients from the GEE analysis.
Logistic regression analysis with generalised estimating equations of factors associated with adverse pregnancy outcomes among systemic lupus erythematosus patients.

CI: confidence interval; OR: odds ratio.
Further univariate and GEE logistic regression analyses of the factors associated with the specific fetal and maternal adverse outcomes revealed that active LN in pregnancy and pre-existing hypertension were the predictors of pre-eclampsia. Pre-pregnant active disease and disease duration were associated with early fetal loss while APS was associated with late fetal loss. Pre-eclampsia was associated with prematurity and IUGR. In addition to that, active disease in pregnancy and active haematological manifestation in pregnancy were associated with prematurity and IUGR, respectively. The use of HCQ was associated with a lower risk of pre-eclampsia and IUGR, but it was no longer significant in the GEE model. Table 4 illustrates the factors associated with the specific fetal and maternal adverse outcomes in pregnancy.
Factors associated with the specific adverse pregnancy outcomes.
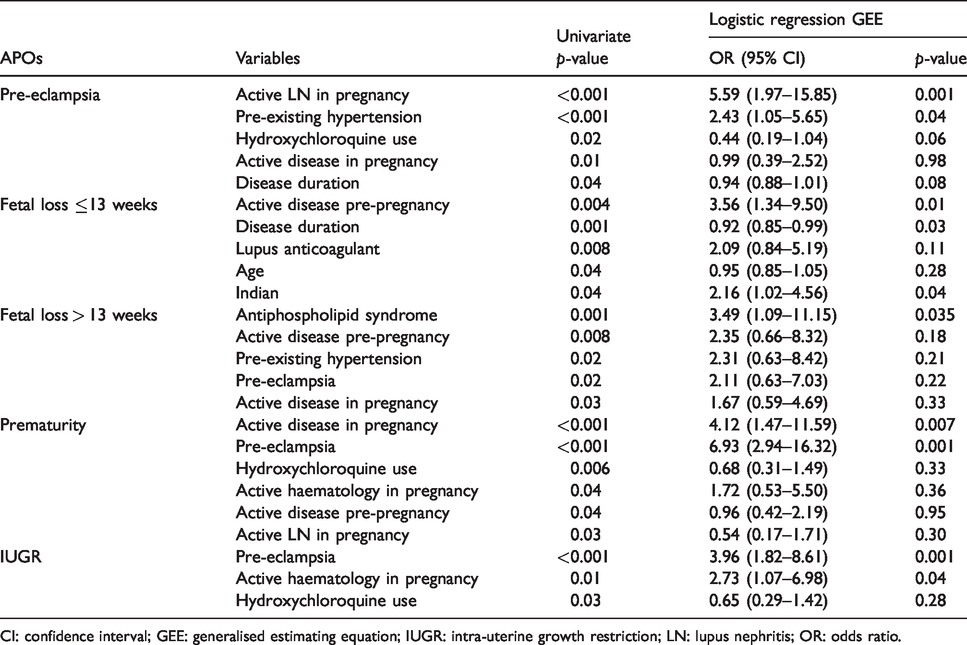
CI: confidence interval; GEE: generalised estimating equation; IUGR: intra-uterine growth restriction; LN: lupus nephritis; OR: odds ratio.
Discussion
Despite the improvement in the rate of live birth, pregnancies among SLE women are still considered high risk as they are associated with various adverse outcomes particularly pre-eclampsia, prematurity and stillbirth.8,14,29 However, the prevalence of APOs among SLE varies due to the heterogeneity of populations, disease activity and definition of APOs. The prevalence of APOs can be lower in patients with low disease activity and Caucasian patients.5,30 Meanwhile, up to one-third of patients with active disease particularly with renal involvement experienced APOs which are demonstrated in the majority of the studies among the Chinese.13,15,31–33
Our multi-ethnic study showed that Indian patients were significantly at increased risk of APOs compared with Malay and Chinese. Ethnic disparities in the pregnancy outcomes are well documented among the multi-ethnic US cohorts where the African American and Hispanic ethnicities are reported to be at a higher risk of APOs.19,34–36 There are few small studies among Indian SLE patients which have reported substantial APOs among them. 37 The live birth rate was lower among SLE patients in India compared with other developing countries but these are not head-to-head studies. 38 From our study, a significantly higher APS was diagnosed among Indians compared with Malay and Chinese. In addition to that, there was high frequency of LN, pre-pregnancy active disease, active disease in pregnancy and positive LA seen among Indians. However, due to the small number of Indians, the differences were insignificant. Indeed these factors could have contributed to the poor pregnancy outcome among them and therefore a larger number of Indian subjects are needed to confirm this. There are several genetic variants that have been identified among the Indian SLE patients,39,40 and few of them have been associated with renal and haematological manifestations. 40 However, the associations of these gene variants with severity of the SLE compared with other ethnicities is largely unknown as no head-to-head multi-ethnic study is available yet. In addition, we did not examine the socio-economic characteristics of the different ethnicities which may have influenced the pregnancy outcomes.
In our study, disease activity pre-pregnancy was found to be one of the independent predictors of APOs in our cohort. In addition to that, poorly controlled disease prior to conception was also independently associated with early fetal loss or miscarriage. This finding concurs with a Chinese study. 31 Thus, it is prudent to ensure that all pregnancies in SLE are well planned and carried out when the disease in quiescent. Active disease during pregnancy was the independent predictor of prematurity and this is consistent with the literature.31,41,42 Active haematological manifestations during pregnancy was independently associated with APOs, particularly IUGR. Indeed, active lupus haematological manifestations such as leucopaenia, thrombocytopaenia and anaemia in pregnancy have been reported to be associated with APOs and fetal loss. 13
Historically, pregnancy was discouraged in patients with a history of LN as it was strongly associated with higher maternal and fetal adverse outcomes in the earlier literature. 43 However, with the advance of LN treatment in pregnancy, more favourable and improving trends of fetal outcome among LN patients are observed in the recent studies.13,30,42,44,45 Nevertheless, the maternal adverse outcomes are still more significant among them such as pre-eclampsia and SLE flares, particularly in those with active LN in pregnancy.13,30,44 Correspondingly, those with active LN during pregnancy had significantly higher adverse fetal outcomes. 31 Similarly, our study demonstrated that active LN in pregnancy was significantly associated with pre-eclampsia and, in turn, pre-eclampsia was associated with fetal prematurity and IUGR.
APS in SLE has long been recognised as one of the predictors of poor pregnancy outcomes and continued to be the important poor prognostic factor in the recent pregnancy studies.13,29,31 It is well established that APS is associated with late trimester fetal loss, 46 as has been demonstrated in our study. Among all of the aPLs, LA was demonstrated to be the strongest predictor of APOs and was associated with early trimester fetal loss. This is consistent with many other studies including the PROMISSE study.5,47
The use of HCQ was associated with lower risk for APOs including pre-eclampsia, prematurity and IUGR in the univariate analysis. However, it was no longer significant in the multivariate analysis model as the number of cases was small. A few studies have reported reduced rate of APOs including fetal loss, IUGR and prematurity.31,48,49 Although the evidence of HCQ in preventing APOs in our study is less robust, it should be continued during pregnancy as HCQ use is associated with lower risk of disease flare in pregnancy.28,49,50
Due to the retrospective nature of this study, there are several limitations which include incomplete data, selection bias and misclassification bias as some of the pregnancy complications such as pre-eclampsia may be difficult to be distinguished with active LN in pregnancy. In addition to that, we did not examine other key factors of APOs such as socio-economic and educational status.19,35 However, our study has highlighted several important predictors of poor pregnancy outcomes including the specific adverse events in pregnancy.
Conclusion
SLE patients remain at an increased risk of APOs particularly pre-term deliveries and pre-eclampsia. LA and disease activity prior to and during pregnancy, as well as Indian patients, are at a higher risk of APOs. Further larger prospective studies are needed to further confirm these risk factors.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.