
Abstract

Sir,
A variety of diseases can develop aortitis such as large vessel vasculitis (giant cell or Takayasu arteritis), anti-neutrophil cytoplasmic antibody-associated vasculitis, Behcet’s disease, relapsing polychondritis, and IgG4-related disease. 1 In systemic lupus erythematosus (SLE), aortitis is extremely rare but a potentially fatal complication, and little is known about lupus aortitis.
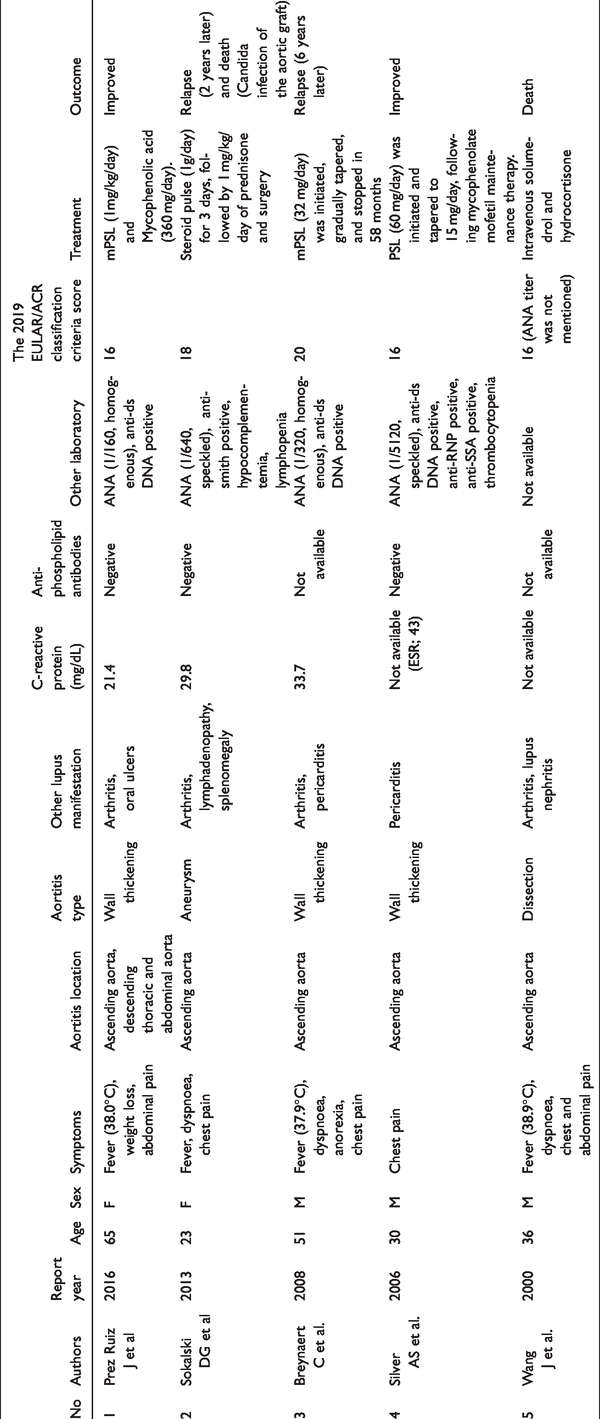
To elucidate characteristics and prognosis of lupus aortitis, we conducted a literature review of cases with aortitis which satisfied the 2019 EULAR/ACR classification criteria for SLE. 2 The cases with no history of glucocorticoid therapy were included in the present study to exclude cases with non-inflammatory aortic problems such as aortic aneurysms or dissection caused by long-term glucocorticoid therapy. 3 We used the PubMed database to identify all English publications using the Medical Subject Heading “lupus” and “aortitis” from the inception date until April 25, 2020. We identified 63 potentially relevant articles, of which 58 were excluded due to the followings; 31 non-related topic, 18 non-English articles, 7 long-term glucocorticoid therapy, 1 insufficient information, and 1 review. As shown in Table 1, a total of five cases with lupus aortitis have been rerported.4–8 Aortitis were diagnosed with imaging examinations including computed tomography, magnetic resonance imaging, and 18 F-fluorodeoxyglucose positron emission tomography in two patients, with pathological confirmation in two patients, and both in one patient. Their age ranged from 23 to 65 years old. Three were male and two were female. They presented with high fever, dyspnea, and chest pain in addition to arthritis. Most patients unusually showed extremely high levels of serum C-reactive protein (CRP, 21.4 to 33.7 mg/dL). Interestingly, all lupus aortitis involved in ascending aorta (Table 1) with either wall thickening (60%, 3/5), aneurysm (20%, 1/5), or dissection (20%, 1/5). Most patients did not have major organ involvement of typical lupus such as cutaneous lesions and nephritis, whereas pericarditis were noted in two patients. Serologically, patients showed high titer of anti-nuclear antibody positivity along with anti-double stranded DNA or anti-smith antibody (Table 1). Anti-phospholipid antibodies were negative in all patients whose data were available. Histological examinations revealed vasa vasorum vasculitis, diffuse lymphocytic infiltration, and necrosis of the tunica elastic without giant cells, glanuloma, and neutrophils. Infections were excluded in all patients, and they were treated with pulse or high dose glucocorticoids with or without mycophenolate. One patient with aneurysm caused by aortitis also received surgery. The more details of treatments and outcome for each patient are shown in Table 1. Four of the five patients improved with the treatment, however, one patient relapsed with aortitis 6 years later, and one patient relapsed 2 years later with alveolar hemorrhage, spotty alopecia, symmetric arthritis, leukopenia, thrombocytopenia, and proteinuria resulting in death due to candida infection of the aortic graft. The other one patient deceased due to aortic dissection caused by lupus aortitis.
Summary of lupus aortitis cases.
The characteristics of lupus aortitis is high serum CRP levels. CRP is not usually elevated in patients with SLE and if elevated, infection or lupus serositis (pleuritis or pericarditis) should be considered as differential diagnosis. 9 Our results suggest lupus aortitis as an emerging etiology of high levels of serum CRP. Interestingly, one lupus aortitis patient in our present study was complicated with pericarditis demonstrating pericardial small vessel vasculitis, 7 indicating common pathogenic mechanisms between serositis and aortitis in lupus patients. Considering the fatality of lupus aortitis in addition to an increased risk of vascular complications with long-term glucocorticoid therapy, specifying therapeutic targets for aortic lesions is warranted. The high levels of CRP in lupus aortitis can evoke the involvement of interleukin-6 in its pathogenesis. Therefore, it is of great interest to investigate the potential effectiveness of interleukin-6 inhibition in patients with lupus aortitis since recent studies have highlighted promising efficacy of anti-interlueking-6 receptor antibody in patients with large vessel vasculitis. 10
In conclusion, when rheumatologists face with atypically high levels of serum CRP in patients with SLE, lupus aortitis should be considered as one of manifestations. Early recognition of lupus aortitis is important for appropriate immunosuppressive treatment and, if necessary, surgical intervention. Further accumulation of cases are needed in future.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YK has received grants or speaker fees from AbbVie, Astellas, Ayumi, Bristol-Myers Squibb, Chugai, Eisai, Eli Lilly, Hisamitsu, Jansen, Kissei, Pfizer, Sanofi, Takeda, Tanabe-Mitsubishi and UCB. TT has received research grants or speaking fees from Astellas Pharma Inc., Bristol–Myers K.K., Chugai Pharmaceutical Co, Ltd, Daiichi Sankyo Co., Ltd, Takeda Pharmaceutical Co., Ltd, Teijin Pharma Ltd, AbbVie GK, Asahi Kasei Pharma Corp., Mitsubishi Tanabe Pharma, Astra Zeneca K.K., Eli Lilly Japan K.K., Novartis Pharma K.K., AbbVie GK, Nippon Kayaku Co. Ltd, Janssen Pharmaceutical K.K., Taiho Pharmaceutical Co., Ltd., and Pfizer Japan Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.