
Abstract
Introduction
In the GLADEL cohort, the bullous lupus (BSLE) prevalence was 0.41%. However, literature on pediatric BSLE is scarce. This study described the clinical, histological, and immunological characteristics and the treatment response in a series of children with BSLE as the first clinical manifestation of pediatric SLE.
Methods
The clinical, histological, and immunological characteristics of a series of 5 cases of BSLE between 2010-2019 from two reference centers in Colombia were analyzed.
Results
All cases had bullous lesions that resolved with residual hypopigmentation. One had a focal seizure, and another arthritis with thrombocytopenia. Two had transient proteinuria with normal urinalysis. Anti-nuclear antibody titers ranged from 1:160 to 1:2560, and four were anti-dsDNA (+). Five patients had anti-RNP antibodies, and four anti-Sm antibodies. All had low C3, and 80% low C4 counts; 80% had erythrocyte sedimentation rate (ESR) ≥20 mm/hour and 60% had C-reactive protein (CRP) ≥0.5 mg/dL. All patients responded to glucocorticoids and dapsone. Histology reports and direct immunofluorescence (DIF) test showed subepidermal blisters with neutrophils in the papillary dermis and linear deposits of Igs/complement proteins in 80% of the skin biopsies. IgG/IgM was present in 5 samples. IgA was positive in 60% and C3 in 80%.
Conclusions
In this pediatric series, BSLE tends to have a monophasic behavior associated with neuropsychiatric, skeletal, and hematological involvement in 40% of the patients, and with good prognosis.
Keywords
Introduction
Pediatric systemic lupus erythematosus (pSLE) is a more severe clinical entity than adult systemic lupus erythematosus (aSLE).1,2 It exhibits articular, renal, and neuropsychiatric as well as cutaneous manifestations, such as malar rash and photosensitivity. These are more frequent at the beginning stages of pSLE in 70% of the cases (unlike aSLE in which these are seen at an early stage in 53% of the cases). 1 Acute cutaneous lupus (ACLE) is associated with hematologic, renal, and neuropsychiatric involvement. However, there are scarce data about the course of bullous lupus (BSLE) in children and its systemic manifestations.
BSLE initially affects the photoexposed and unexposed skin and mucous areas, and resolved without scars or milium cysts. The pathogenesis of BSLE is related to the presence of antibodies that recognize epitopes in the region of the amino-terminal noncollagenous (NC1) domain of collagen VII present in the basement membrane.3,4 Bullous lesions were reported as a rare manifestation of ACLE (prevalence of 0.41% of cases in the GLADEL cohort). 5 The relationship between BSLE and systemic disease involvement in children is currently unclear. It has been reported that adult patients can have concomitant lupus nephritis (50-90% of cases) and hematologic involvement (in up to 100% of the cases).6–8
In Latin America, BSLE cases have usually been reported in adults with only one case report of 3 pediatric patients in Brazil. 9 The purpose of this study was to describe the clinical, histological, and immunological characteristics, and the response to treatment in a series of children with BSLE as the first clinical manifestation of pSLE.
Methods
A series of five patients with pSLE who were diagnosed between 2010 and 2019 in 2 hospitals in Colombia (Hospital Universitario San Vicente Fundación, Medellín and Hospital Universitario Fundación Valle del Lili, Cali) were reviewed. The Ethics Committee of the participating institutions approved the study before initiation of data extraction. The inclusion criteria were patients under 18 years of age who met the 2012 Systemic Lupus International Collaborating Clinics (SLICC) criteria for SLE, whose first manifestation was the presence of blisters with characteristic findings on histological and immunofluorescence tests, compatible with BSLE meeting the Camisa and Grimwood criteria. 10
Clinical investigations
A review of clinical, photographic, and laboratory records was performed. Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) was also measured in all patients.
Histological and immunopathological investigations
Biopsies of the injured skin were taken for hematoxylin-eosin staining (H&E) for histological evaluation. Direct immunofluorescence (DIF) was performed on the skin around the lesion using antibodies against IgG, IgM, IgA, and C3 or C1q, describing the fluorescence patterns. Two dermatologists evaluated all the samples, who are experts in autoimmune blistering diseases.
Results
Table 1 shows the clinical and histological characteristics of the evaluated cases. Five patients were included, of which 4 were girls; all had vesiculobullous lesions disseminated on the back, anterior thorax, abdomen, upper and lower extremities, and face.
Overview of patients with BSLE with relevant clinical, histopathologic and treatment features.
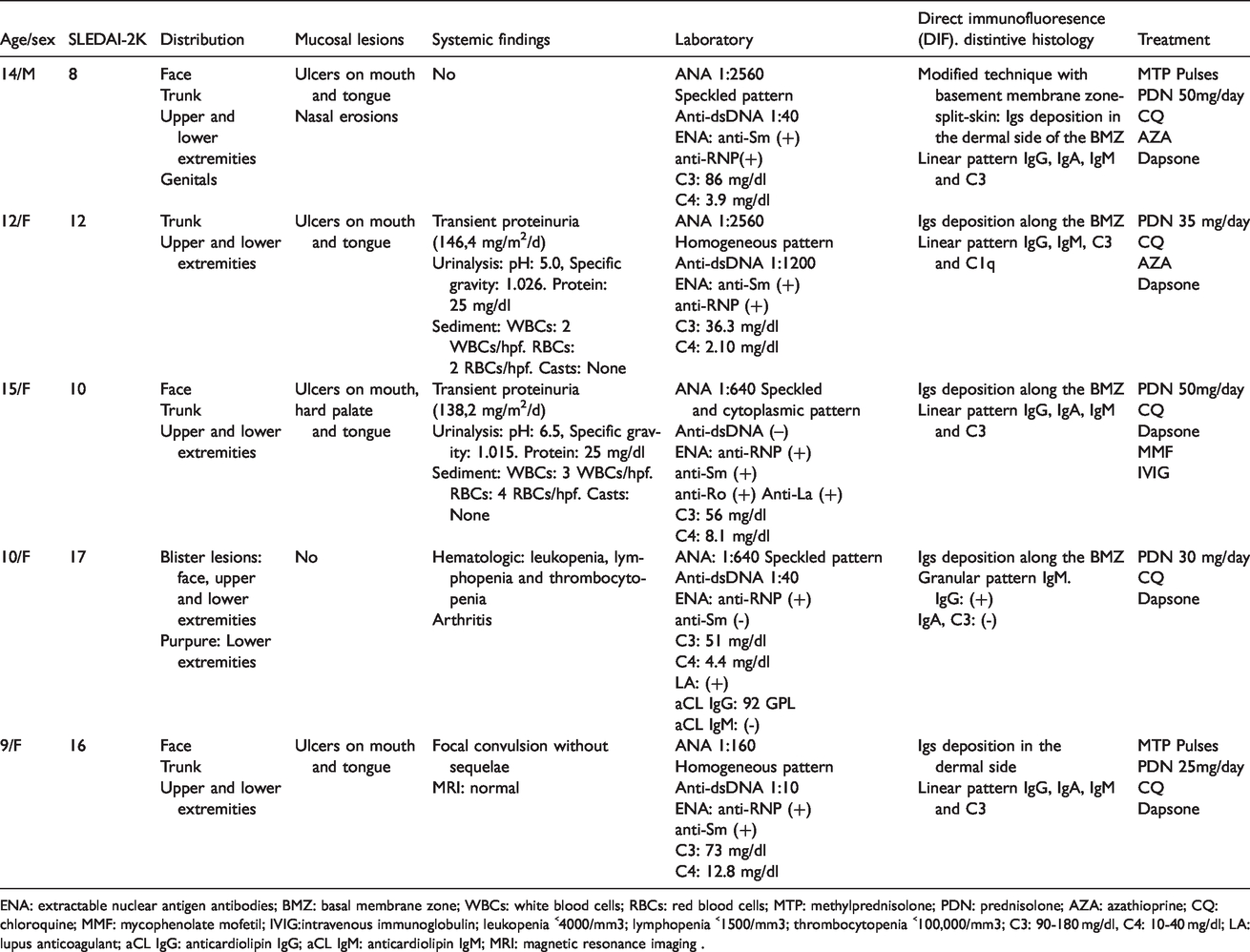
ENA: extractable nuclear antigen antibodies; BMZ: basal membrane zone; WBCs: white blood cells; RBCs: red blood cells; MTP: methylprednisolone; PDN: prednisolone; AZA: azathioprine; CQ: chloroquine; MMF: mycophenolate mofetil; IVIG:intravenous immunoglobulin; leukopenia ˂4000/mm3; lymphopenia ˂1500/mm3; thrombocytopenia ˂100,000/mm3; C3: 90-180 mg/dl, C4: 10-40 mg/dl; LA: lupus anticoagulant; aCL IgG: anticardiolipin IgG; aCL IgM: anticardiolipin IgM; MRI: magnetic resonance imaging .
These lesions affected the healthy skin in all cases, and in 1 patient, manifested as malar erythema. There was no difference in the lesions between photoexposed and unexposed skin. The blisters healed with residual hypopigmentation, without scars or milium. One patient had purpura in the lower extremities without vasculitis. Regarding mucous membrane, the oral mucosa was the most frequently involved (80% of cases) and there were no ocular lesions (Figure 1).

Case 1 (a,b) Blisters, erosions, crust and hypopigmented scars on trunk and extremities. (c,d) Blisters, erosions, crust and hypopigmented scars on face, neck and hands. Note the involvement of vermilion border of the lips. Case 3 (e,f) Tense blisters, some of them with an annular configuration, erosions and crust on the trunk and extremities. Case 5 (g) Tense blisters of serous and hemorrhagic content, erosions and crust on face, trunk and extremities
All patients had an anti-nuclear antibody (ANA) (+) with titers between 1:160 and 1:2560 with a speckled and homogeneous pattern. Anti-dsDNA was found in 4 patients with titers between 1:10 and 1:1200. Extractable Nuclear Antigens were 100% positive for Ribonucleoprotein (RNP) antibodies, and 80% for Smith (Sm) antibodies. Only 1 patient was positive for anti-SSA/SSB. All patients had hypocomplementemia with low C3 levels in all 5 and low C4 levels in 4. Erythrocyte sedimentation rate (ESR) was ≥20 mm/hour in 80% of the children, and C-reactive protein (CRP) was ≥0.5 mg/dL in 60%. Antiphospholipid antibodies tested positive in 1 case (lupus anticoagulant –LA- and anticardiolipin IgG -aCL IgG-).
Among the systemic manifestations of pSLE, none had lupus nephritis, 2 patients had transient proteinuria (146.4 and 138.2 mg/m2/day) and normal urinalysis results. None had hypertension. One patient had an episode of focal seizure, without recurrences or sequelae with normal cerebrospinal fluid, brain computed tomography, and magnetic resonance imaging (MRI) studies. Another case exhibited leukopenia, thrombocytopenia, and arthritis. The median SLEDAI-2K score was 12 (IR: 8-17).
Histology reports showed the presence of subepidermal blisters, neutrophilic infiltrate in the papillary dermis, and thickening of the basement membrane. This pattern was indistinguishable from that observed in herpetiform dermatitis and linear IgA dermatosis. DIF showed pure linear immunoglobulin and complement deposits in most cases (75% of cases), and 1 patient had pure granular-type deposits; none had a mixed pattern. IgG and IgM were present in 100% of the samples; IgA was positive in 60% of the cases and C3 in 80% (Figure 2).
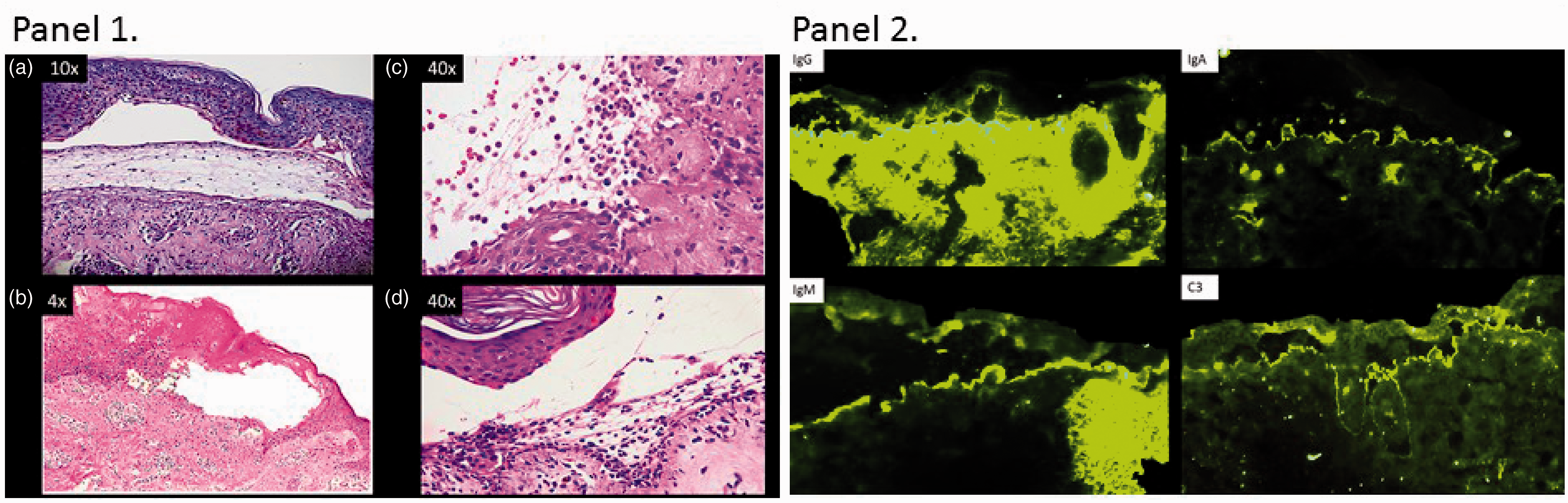
Panel 1. Hematoxylin and eosin staining. (a,b) Cases 2 and 4: Subepidermal blisters with inflammatory infiltration in subpapillary chorion. (c,d) Cases 3 and 5: Abundant neutrophil infiltration. Panel 2. Direct immunofluorescence: Case 1: Linear pattern for IgG, C3, IgM and IgA. (Full house).
The established treatment for this condition is a combination of glucocorticoids (prednisolone 30–50 mg/day), dapsone (25-100 mg/day), and antimalarials. One patient developed methemoglobinemia of 12.3% and hypoxemia at a dose of 100 mg/day of dapsone. After 72 hours of improvement in hypoxemia, dapsone was re-initiated at a lower dose (25 mg/day) with a good response. Azathioprine and mycophenolate mofetil were administered to 3 patients as steroid-sparing agents. One patient received intravenous immunoglobulin (IVIG) before the diagnosis of BSLE because of suggested toxic epidermal necrolysis (TEN). At 3 months, BSLE did not recur in 4 patients. One case had a relapse due to non-adherence to treatment.
Discussion
This is the first series of BSLE as an early manifestation of pSLE reported in our country. Blisters with sloughing and bleeding were the most frequent cutaneous manifestations, and only 1 case with purpura in the lower extremities was observed. Purpura is an unusual finding in BSLE; hence, other conditions like particularly vasculitis and TEN should be considered in the differential diagnoses.
There was significant involvement of the face, anterior thorax, abdomen, and upper extremities with lower extremities involvement in 100% of cases, which is higher than what was reported in a previous series (frequency between 36 to 50%). 8
As reported in adults, anti-DNA was positive in 80% of the patients, and the positivity of anti-DNA varied between 60-90% in this series.7,8 An interesting finding was that the patients with more extensive involvement had high titers of anti-RNP/Sm. So far, there is no known correlation between the skin phenotype in BSLE and the autoantibody profile. Elevation of acute phase reactants and C3/C4 hypocomplementemia was not related to the severity of skin lesions.
The appearance of systemic manifestations was seen in 2 cases, with a self-limited course, and without sequelae: 1 case had a focal seizure, leukopenia, thrombocytopenia, and arthritis; 2 cases had transient proteinuria. These findings are in contrast with those reported in the literature, where lupus nephritis has been found in 50-90% and anemia/leukopenia in 45-100% of BSLE patients.5–8 BSLE in children as an initial manifestation of pSLE might be a more benign condition in terms of prognosis and systemic complications than other forms of ACLE or manifestations in adulthood.
DIF findings on skin biopsy showed IgG and IgM deposits along with C3. These characteristics associated with the presence of subepidermal blisters and neutrophilic infiltration of the papillary dermis allow differentiation of BSLE from other bullous diseases in the appropriate clinical context (hypocomplementemia, elevated ESR/CRP and positive ANA).11–13
Dapsone, combined with glucocorticoids and antimalarials, was the pharmacological treatment of choice with improvement in 100% of the cases.11–14 In children, it might be preferable to begin with the lowest possible dose of dapsone (25 mg/day) with a progressive escalation of up to 2 mg/kg/day. Hemogram and pulse oximetry should be performed to detect complications such as hemolytic anemia and methemoglobinemia; however, the decision to measure glucose-6-phosphate dehydrogenase (G6PD) levels is controversial. In this study, one of the cases presented methemoglobinemia with a dose of 2 mg/kg/day of dapsone and there were no cases of hemolytic anemia. All the children had normal values of G6PHD.
Despite the few numbers of cases reported, this study shows that it is important to consider the diagnosis of BSLE in children with bullous diseases. BSLE might be the isolated manifestation of pSLE. Specific clinical clues such as lymphopenia, active urinary sediment, proteinuria, the elevation of ESR/CRP levels, and hypocomplementemia should alert the pediatrician to initiate appropriate treatment 14
Conclusion
BSLE may be the first manifestation of pSLE. Systemic manifestations are not always present with greater lower limb involvement, hypocomplementemia, and anti-RNP/Sm antibodies as they are in adults. In this pediatric series, BSLE tends to have a more benign clinical course than other forms of ACLE. The best treatment is the combination of dapsone, glucocorticoids, and antimalarials, although the lowest dose of dapsone should be started to avoid adverse effects. BSLE tends to have a monophasic behavior; however, because of persistent immunological alterations, it is necessary to monitor relapses, mainly renal, hematologic, and neuropsychiatric.
Footnotes
Acknowledgements
The author(s) would like to thank all the staff of the Department of Rheumatology, and Dermatology of the Hospital Universitario San Vicente Fundación, Hospital Universitario Fundación Valle del Lili, and the families of the patients for their collaboration in the compilation of the cases.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.