
Abstract
Objective
To investigate the profiles of anti-RPLP0, anti-galectin3 antibodies, interferon-α (IFN-α), interferon-λ1(IFN-λ1) and interleukin-17A/F(IL-17A/F) in the subtypes of cutaneous lupus erythematosus (CLE) including acute CLE (ACLE), subacute CLE (SCLE) and discoid lupus erythematosus (DLE).
Methods
Serum levels of autoantibodies and cytokines were determined by enzyme-linked immunoabsorbent assay (ELISA). Lupus lesions were evaluated by cutaneous lupus erythematosus disease area and severity index (CLASI).
Results
Serum anti-RPLP0, anti-galectin3 antibodies and IFN-λ1 were higher in systemic lupus erythematosus (SLE) patients with skin lesions than those without skin lesions, compared to healthy controls. IFN-α, IL-17A and IL-17F was elevated in all patients regardless of skin lesions. The two antibodies, IFN-α and IL-17A were positively correlated with the CLASI score in all patients with CLE. In addition, serum IL-17A was positively correlated to the CLASI score of ACLE, SCLE and DLE, while anti-RPLP0 and anti-galectin3 antibodies were only correlated to the score of SCLE and IL-17F to DLE.
Conclusion
Serum anti-RPLP0, anti-galectin3 antibodies, IFN-α, IFN-λ1 and IL-17A/F are associated with the occurrence of lupus skin lesions regardless of the systemic complications, whereas the profiles of these inflammatory mediators vary with the subtypes of lupus skin lesions.
Keywords
Introduction
Skin lesions are the most common clinical findings in lupus patients. It is referred as cutaneous lupus erythematosus (CLE) when the disease is confined to the skin, while known as one of the damaged organs in systemic lupus erythematosus (SLE). 1 CLE is classified into three subtypes including acute CLE (ACLE), subacute CLE (SCLE) and chronic CLE (CCLE) based on medical history, clinical and histological manifestations. Discoid lupus erythematosus (DLE) is the most common type of CCLE. 1
The pathogenesis of CLE remains largely unknown. Clinically, ACLE is highly indicative of SLE disease, a proportion of SCLE patients develop SLE in their lifetime, 2 whereas the majority of SLE patients may present one or more subtypes of CLE in the disease-duration. These evidences suggest that autoantibodies and cytokines identified in SLE might be associated and even varied with the subtypes of CLE. Our previous study suggested that anti-RPLP0 and anti-galectin3 antibody played a key role in the pathogenesis of lupus skin lesions in SLE. 3 Therefore, in this study we evaluated the serum levels of anti-RPLP0, anti-galectin3 antibodies and cytokines such as interferons and interleukin-17 (IL-17) in patients with ACLE, SCLE and DLE and analyzed the correlation of these inflammatory mediators with the activity of lupus skin damages.
Materials and methods
Patients
Patients were diagnosed with SLE according to the American College of Rheumatology (ACR) revised criteria for SLE. 4 CLE was diagnosed based on the clinical features, histological examination and laboratory tests, and classified into three different groups known as ACLE, SCLE and DLE according to the consensus. 1 SLE disease activity and the severity of lupus skin lesions was assessed by the systemic lupus erythematosus disease activity index (SLEDAI) and the cutaneous lupus erythematosus disease area and severity index (CLASI), respectively.5,6 Healthy controls were 15 sex- and age-matched blood donors. The study was approved by the research ethics board of Sun Yat-sen Memorial Hospital and the informed consents were obtained from all participants.
ELISA
Serum levels of anti-RPLP0, anti-galectin3 antibodies, IFN-α, IFN-λ1, IL-17A and IL-17F were measured using ELISA kit (eBioscience, USA) according to the manufacturer’s instructions. All experiments were performed in duplicates.
Statistical analysis
Data were summarized with mean ± SD and median (interquartile). Median age between patients and controls was compared using Mann-whiney U test. The comparisons of CLASI score, cytokines and autoantibodies among groups were analyzed using Kruskal-Wallis test and followed by Dunn’s post hoc multiple comparison tests. The correlation analyses were performed by Spearman’s rank correlation test, using prism 8. P < 0.05 was considered statistically significant.
Results
Patients
Fifty-two LE patients and 15 healthy controls were enrolled in this study. The median age and gender ratio in patients’ group was 32.5 years old and 38:14 (female: male), respectively, which is comparable to the healthy controls (28 years old, 10:5). Of 52 LE patients, 10 were SLE patients without skin lesions (SLE skin−) and 42 were LE patients with skin lesions (LE skin+) consisting of 15 SLE patients with ACLE (referred as ACLE/SLE thereafter), 14 with SCLE and 13 with DLE. Patients with SCLE and DLE did not fulfill the diagnostic criteria of SLE. The median CLASI activity score was comparable among the three subtypes of CLE (ACLE/SLE v.s SCLE v.s DLE: 7 v.s 9 v.s 5, P = 0.28), whereas the damage score was relatively higher in patients with DLE than those with ACLE/SLE and SCLE (ACLE/SLE v.s SCLE v.s DLE: 1 v.s 2 v.s 4, P < 0.05).
Serum levels of autoantibodies and cytokines
Anti-RPLP0, anti-galectin3 antibodies and IFN-λ1 were elevated in all three groups of patients with skin lesions but not in SLE patients without skin lesions compared to healthy controls. However, IFN-α, IL-17A and IL-17F was elevated in all groups of patients, in the presence and absence of skin lesions (Figure 1).
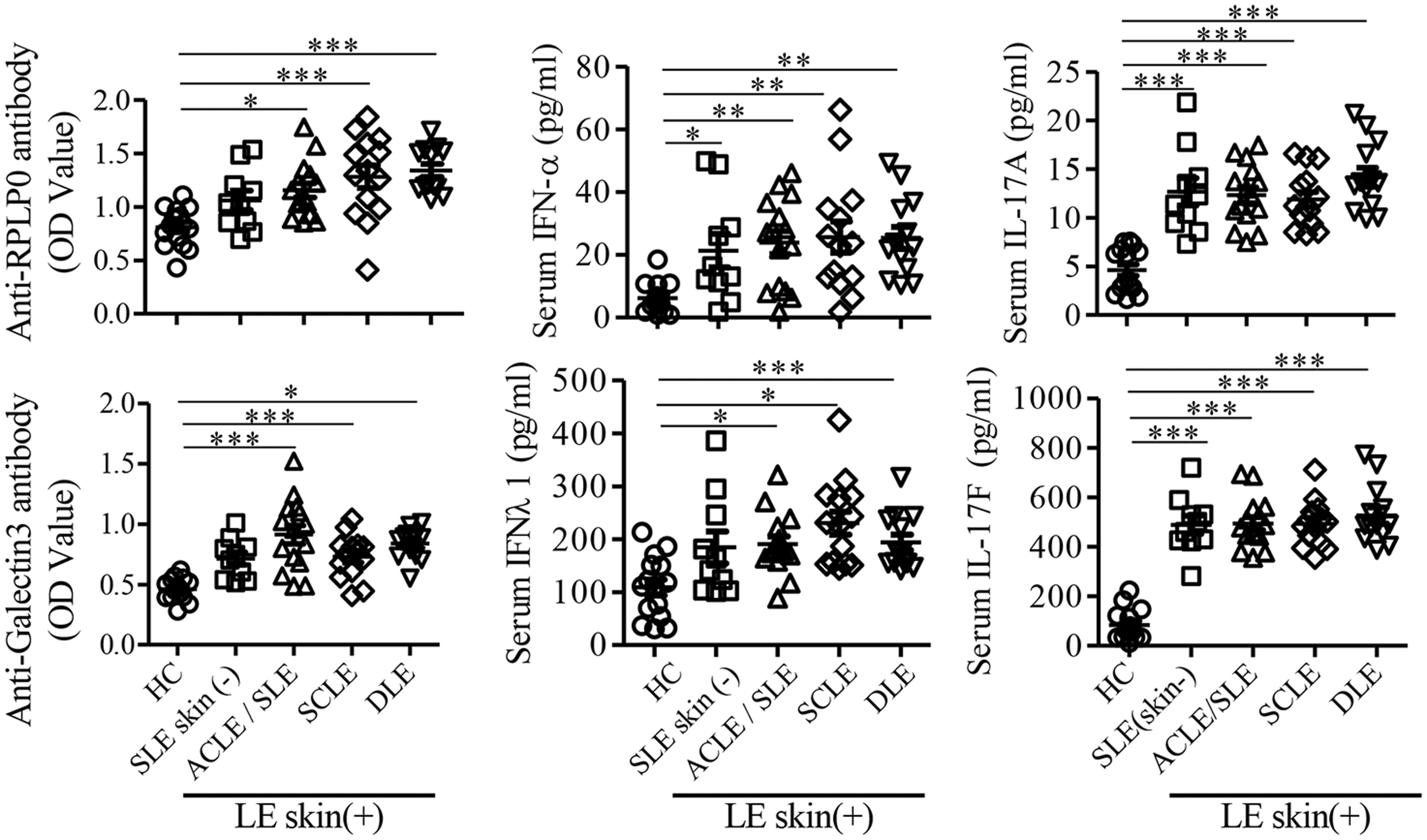
Comparison of serum levels of autoantibodies and cytokines between LE patients and healthy controls. ELISA analysis of serum levels of anti-RPLP0, anti-galectin3, IFN-α, IFN-λ1, IL-17A and IL-17F in healthy controls (n = 15) and LE subtypes: ACLE/SLE (n = 15), SCLE (n = 14), and DLE (n = 13). Data are representative of two or more independent experiments. *P < 0.05 **P < 0.01 ***P < 0.001 by Dunn’s multiple comparison tests. LE: lupus erythematosus; SLE: systemic lupus erythematosus; ACLE/SLE: ACLE + SLE+; SCLE: SCLE + SLE−; DLE: DLE + SLE−.
Correlation of serum levels of autoantibodies and cytokines with skin disease activity
Since the examined autoantibodies and cytokines were increased in all LE patients with skin lesions, we then evaluated if they were correlated with skin disease activity measured by CLASI. We found that anti-RPLP0, anti-galectin3 antibodies, IFN-α and IL-17A, but not IFN-λ1 and IL-17F were positively correlated with the overall CLASI activity score (Figure 2). In addition, IL-17A was positively correlated with the CLASI activity score of ACLE/SLE, SCLE and DLE. Anti-RPLP0 and anti-galectin3 antibodies were positively correlated with the CLASI activity score of SCLE, while IL-17F was associated with DLE disease activity (Figure 3(a) to (c)).
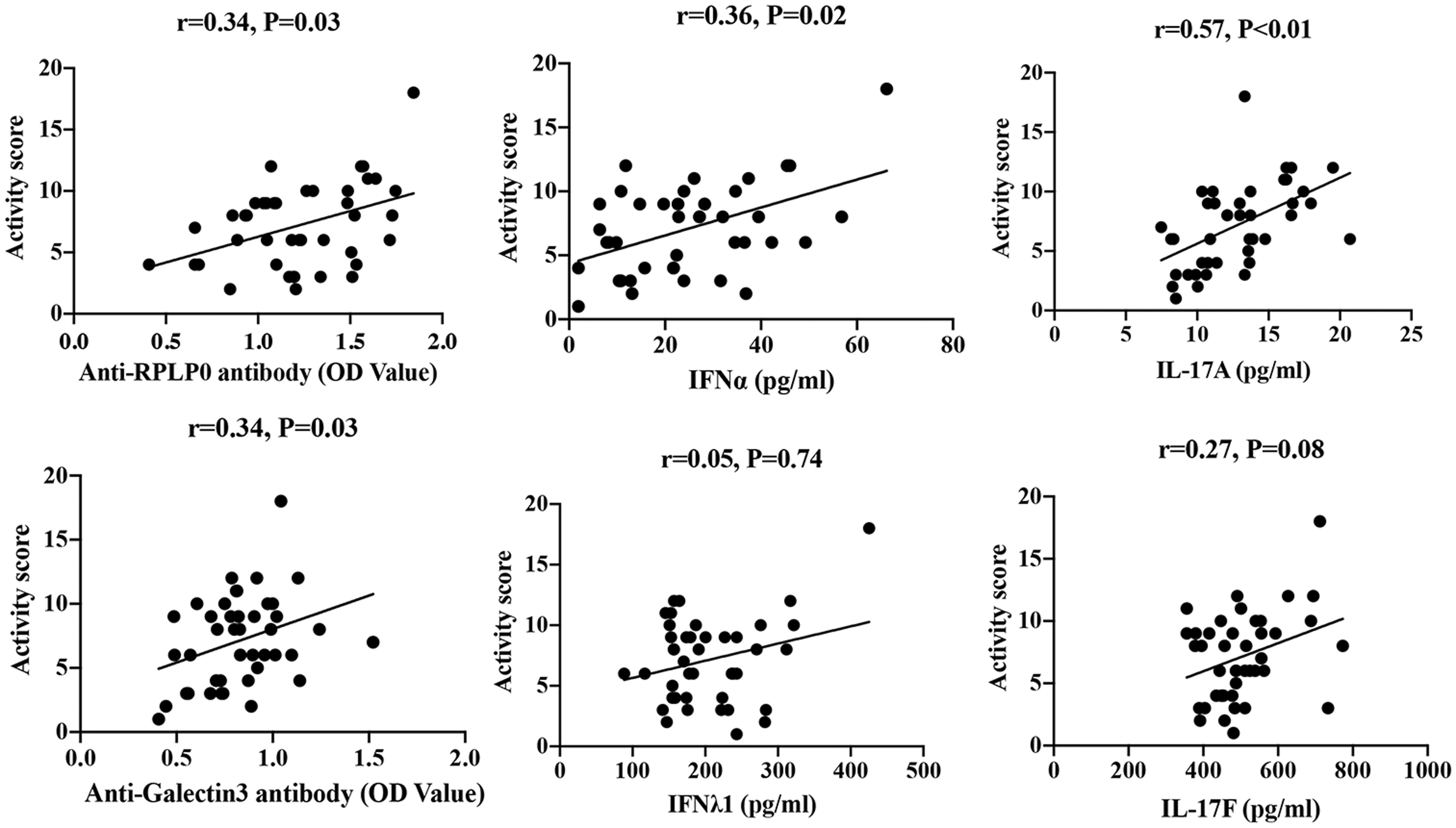
Correlation of autoantibodies and cytokines with the CLASI score in LE skin+ patients. Correlation of serum anti-RPLP0, anti-galectin3, IFN-α, IFN-λ1, IL-17A and IL-17F with skin lesion activity measured by cutaneous lupus disease area and severity index (CLASI) in 42 LE patients. Data are representative of two or more independent experiments. By Spearman’s rank correlation test. LE: lupus erythematosus.
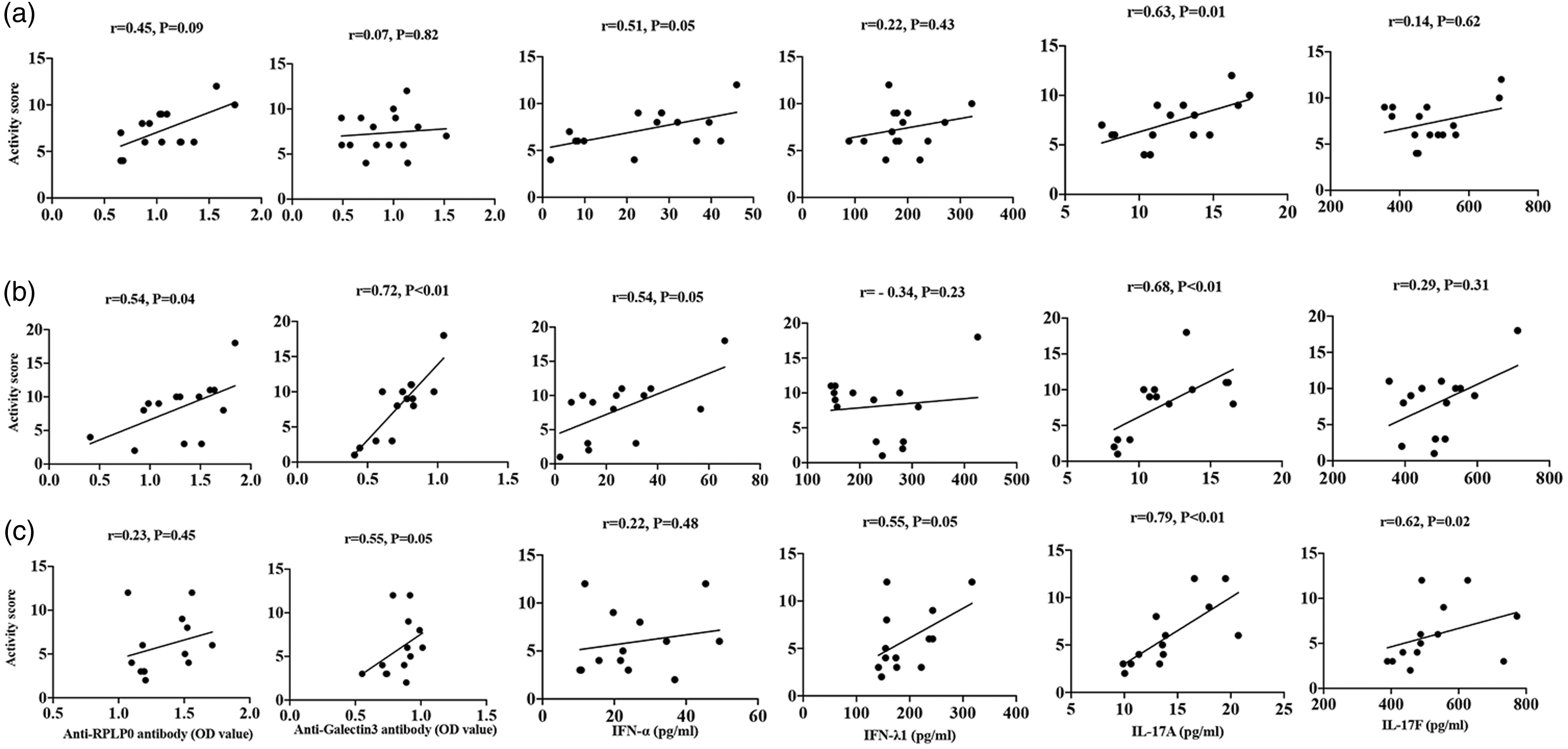
Correlation of autoantibodies and cytokines with the CLASI score in the subtypes of CLE. Correlation of serum anti-RPLP0, anti-galectin3, IFN-α, IFN-λ1, IL-17A and IL-17F with skin lesion activity measured by cutaneous lupus disease area and severity index (CLASI) in ACLE/SLE (n = 15) (a), SCLE (n = 14) (b), DLE (n = 13) (c) subtypes. Data are representative of at least independent experiments. By Spearman’s rank correlation test. CLE: cutaneous lupus erythematosus; ACLE/SLE: ACLE + SLE+; SCLE: SCLE + SLE−; DLE: DLE + SLE−.
Discussion
In the present study we showed that serum IFN-α and IL-17A was elevated in all lupus patients and positively correlated with the CLASI score in patients with lupus skin lesions, suggesting that the two cytokines may be involved in the pathogenesis of both systemic disease and lupus skin damages.
The pathogenic role of interferons (IFNs) in CLE has been recognized in the first place because the IFN signature genes were not only upregulated in skin lesions and blood, but even more prominent in skin than blood.7–10 Besides, IFN-α expression in skin was well correlated with the CLASI score,7,10 whereas serum IFN-α alone was inferior to the panel of serum type I interferon related genes in assessing disease activity.7–9 IFN-λ1 belongs to the type III interferon group. We showed that serum IFN-λ1 was increased in SLE patients with skin lesion, but not in those without skin lesions, which is in line with the previous report that serum IFN-λ1 was elevated in patients with DLE, especially in those with disseminated skin lesions. 11 However, inconsistent with the findings of IFN-λ1 declining with clinical remission, 11 we did not show the correlation of serum IFN-λ1 with the CLASI score. This could be due to the small sample size and majority of patients with mild-moderate diseases (median CLASI activity score 7.5) in the present study. IFN-λ1 was not only elevated in serum but highly expressed in DLE and SCLE skin lesions. 11 Keratinocytes were not only the major sources but the responders of IFN-λ in skin. Skin damage was significantly attenuated in a murine lupus model with IFN-λ receptor deficiency.11,12 Together, these data suggest that IFN-λ1 plays a critical role in lupus skin damages.11,13
The role of IL-17 in lupus skin damage was acknowledged because serum IL-17 and IL-17+ cells infiltrating in lupus lesions were increased in patients with SCLE and DLE compared to healthy controls.10,14,15 Moreover, the expression of IL‐17A was positively associated with the expression of IFN‐α determined by immunohistochemistry staining. 10 However, compared to Th1 cells, Th17 cells were a minimal population infiltrating in DLE lesions that was determined by whole-skin transcriptomic analyses and in vitro cells stimulation. 16 Of interest, circulating Th17 cells were closely related to the expression of CCL17 and CXCR3 in skin in DLE but not SCLE patients. 15 We showed that IL-17F was increased in all subtypes of CLE, but only correlated with the CLASI score in DLE. Thus, the members of IL-17 family may particularly link to certain subtype of CLE. Serum IL-17A was highly correlated with the CLASI score of all subtypes of CLE, suggesting a general pathogenic role of IL-17A in LE skin damages. Indeed, Ro52 knockout lupus mice failed to develop skin lesion after depletion of IL-17 gene. 17 Recently, Ustekinumab, an inhibitor of Th17 cell differentiation was used to successfully treat a patient with psoriasis and SCLE. 18 Also, a clinical trial of Secukinumab, an inhibitor of IL-17A to treat DLE is to be conducted (NCT03866317). 19 The growing evidences suggest IL-17A blockades are a potential treatment for CLE.
Anti-RPLP0 and anti-galectin3 antibodies were involved in lupus skin damages that was demonstrated both by our previous and current study. 3 However, the association of serum autoantibodies with the CLASI score varied with the subtypes of CLE. It is of note that ACLE/SLE patients presented higher SLEDAI score than SLE skin− patients (12 vs 5, P<0.05), suggesting patients may undergo different grades of immune response. Indeed, the cytokine profile was changed when CLE patients progressed into SLE. 20 DLE was featured by increased circulating IL-17+ T cells, reduced regulatory T cells, lower frequency of autoantibodies and stronger cellular response in skin compared to SCLE.14,15 Thus, the pathogenic role of anti-RPLP0 and anti-galectin3 antibodies may be weighted according to the subtypes of CLE .
Taken together, our results suggest that lupus skin lesions are orchestrated by many circulating cytokines and autoantibodies in the presence and absence of systemic complications. The profile of inflammatory mediators varies with the subtypes of CLE while grants common features at the same time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the National Natural Science Foundation of China (grants 81872524, 81673063).